Purpose
To propose a unifying theory regarding the pathogenesis of maculopathy associated with cavitary optic disc anomalies and to describe a rational approach to achieving a permanent cure in affected eyes.
Design
Interpretive essay.
Methods
Review and synthesis of selected literature, with interpretation and perspective in relating pathoanatomic features to pathogenesis and treatment.
Results
Congenital cavitary anomalies of the optic disc, including typical coloboma, optic pit (and other atypical colobomas), morning glory anomaly, and extrapapillary cavitation, are associated with an enigmatic maculopathy characterized by schisis-like thickening and serous detachment. The unifying anatomic theme of these anomalies is the presence of a scleral (or lamina cribrosa) defect permitting anomalous communications between intraocular and extraocular spaces. These communications enable the critical pathogenic mechanism responsible for the maculopathy, namely, dynamic fluctuations in the gradient between intraocular and intracranial pressures that direct the movement of fluid (vitreous humor or cerebrospinal fluid) into and under the retina. Vitreous traction does not seem to play a significant pathogenic role. Permanent cure of the maculopathy requires either elimination of the translaminar pressure gradient or closure of the pathway for fluid flow into the retina. We advocate carefully titrated juxtapapillary laser photocoagulation followed by vitrectomy with gas tamponade for creation of a permanent intraretinal and subretinal fluid barrier.
Conclusions
The peculiar features of cavitary optic disc maculopathy can be explained only by considering the pressure gradients that develop along anomalous communications between intraocular and extraocular spaces. A permanent cure for this condition can be achieved by closing the pathway for fluid migration from the cavitary lesion into and under the retina.
A peculiar and enigmatic maculopathy commonly occurs in association with several congenital cavitary anomalies of the optic disc, including typical optic nerve coloboma, optic pit (and other atypical colobomas), morning glory anomaly, and extrapapillary cavitation. Although usually described as distinct clinical entities, these anomalies likely fall within a spectrum with variable pathoanatomic features but similar embryogenesis and pathologic sequelae.
The pathogenesis of serous maculopathy complicating cavitary disc anomalies is as intriguing as it is controversial, and for many decades has defied attempts to understand it clearly. This lack of clarity has spawned a diversity of treatment approaches with variable efficacy. Attempting to understand the fluid origin and pathophysiology of this condition informs us about the structure of the optic disc and juxtapapillary retina and the dynamic forces that influence these tissues. In this Perspective, we discuss the varying clinical presentations of the cavitary disc anomalies and associated maculopathy, the probable pathophysiologic mechanisms involved, and key considerations regarding management.
Classification of Congenital Cavitary Optic Disc Anomalies
Typical coloboma of the optic nerve is a congenital excavation located in the inferonasal aspect of the disc ( Figure 1 , Top left). It is typically a sporadic and unilateral condition. The juxtapapillary tissues inferior to the disc may be involved. Often, the affected eye is otherwise normal, and visual field loss is confined to the site of the defect. Localized serous maculopathy may develop in eyes with optic nerve coloboma, whereas extensive rhegmatogenous retinal detachment more likely occurs in eyes with large associated chorioretinal coloboma.
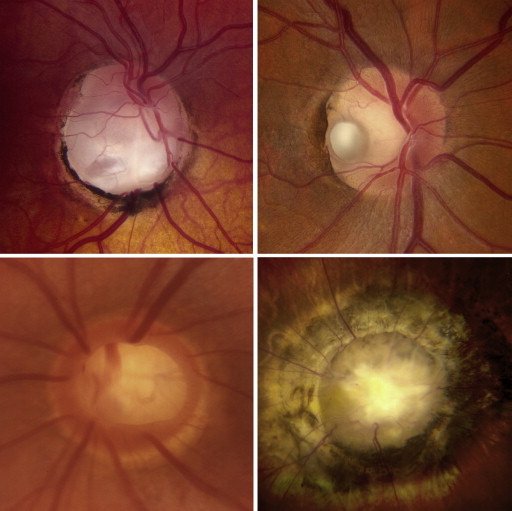
Optic disc pits are focal cavitations isolated to the disc that are typically small and temporally located, but can also be quite large and involve other portions of the disc. They lie on a spectrum of anomalies often referred to as atypical optic nerve colobomas . Although classic optic pits usually are unilateral and appear as focal grayish cavitations ( Figure 1 , Top right), when atypical colobomas are bilateral, large, and centrally located, they can be mistaken for glaucomatous optic cupping ( Figure 1 , Bottom left). Optic pits may cause congenital field defects because of associated nerve fiber layer defects. Serous maculopathy develops in more than 50% of cases, particularly in eyes with large and temporally located excavations.
Morning glory disc anomaly is a unilateral markedly enlarged optic papilla with funnel-shaped excavation involving the optic disc and peripapillary retina ( Figure 1 , Bottom right). It features a characteristic radial arrangement of retinal vessels emanating from the disc, glial hyperplasia over the center of the disc, a rim of elevated peripapillary pigmented tissue, and traction on adjacent retina. Affected patients typically have poor vision.
Because of its inferonasal location, typical optic disc coloboma is attributed to faulty closure of the embryonic ocular fissure. However, several lines of evidence suggest that all of the congenital cavitary disc anomalies associated with macular detachment may share similar embryogenic mechanisms. Because the normal embryonic fissure extends along the inferior aspect of the globe and completely surrounds the optic papilla at its most posterior extent, it is anatomically plausible that faulty closure of this fissure could result in the diversity of cavitary disc lesions under discussion. Furthermore, histopathologic specimens demonstrate similarities between optic pit, morning glory syndrome, and typical coloboma. In each case, dysplastic retina is herniated posteriorly through a defect in the lamina cribrosa, juxtapapillary sclera, or both, ranging from a focal defect in optic pits to a circumpapillary defect in morning glory anomalies. Finally, both optic pit and morning glory discs frequently occur in association with typical coloboma in the same or contralateral eye. In 1 extended family spanning 5 generations with an autosomal dominant inheritance pattern, 35 members had a phenotypically diverse range of optic disc anomalies, including disc pit, coloboma, and morning glory syndrome.
In addition to these anomalies involving the optic nerve itself, cavitary anomalies that lie separate from but near to the optic nerve occasionally can cause a maculopathy identical to that seen with cavitary disc lesions. On optical coherence tomography (OCT) imaging, the pathoanatomic features of such lesions, as with the disc anomalies, seem to involve herniation of abnormal retinal tissue through a scleral defect.
Clinical Features of Cavitary Disc Maculopathy
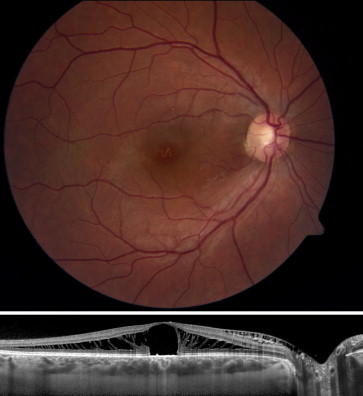
The maculopathy associated with cavitary optic nerve anomalies typically develops in a 2-step process, starting with fluid accumulation within the retinal stroma that results in a peculiar schisis-like retinal edema. Lincoff and associates first observed the schisis-like intraretinal fluid with biomicroscopy and noted that it seems to emanate from the disc anomaly. Optical coherence tomography imaging later confirmed this observation, demonstrating that the intraretinal fluid accumulates most prominently in the outer plexiform layer. More recent high-resolution OCT imaging has shown that fluid from an optic pit can enter into and accumulate within many different retinal layers. The intraretinal fluid then may percolate into the subretinal space, sometimes through an outer layer break that may be detectable biomicroscopically, histopathologically, or by OCT. Although the intraretinal fluid communicates with the optic disc cavitation, the submacular fluid typically does not ( Figure 2 ). Only rarely does fluid appear to enter the subretinal space directly from the optic disc without intraretinal fluid accumulation.

Serous maculopathy occurs in more than 50% of eyes with cavitary disc anomalies, with onset typically in early adulthood. However, macular detachment can be seen in early infancy as well as late in life. Detachment typically is confined to the posterior pole, but can be more extensive in some cases, particularly in eyes with large atypical colobomas or morning glory anomaly. Untreated serous maculopathy associated with optic disc pits and related anomalies typically leads to poor visual outcomes. One natural history study of 15 untreated subjects over 9 years reported that 80% lost vision to a level of 20/200 or worse.
Clinical Features of Cavitary Disc Maculopathy
The maculopathy associated with cavitary optic nerve anomalies typically develops in a 2-step process, starting with fluid accumulation within the retinal stroma that results in a peculiar schisis-like retinal edema. Lincoff and associates first observed the schisis-like intraretinal fluid with biomicroscopy and noted that it seems to emanate from the disc anomaly. Optical coherence tomography imaging later confirmed this observation, demonstrating that the intraretinal fluid accumulates most prominently in the outer plexiform layer. More recent high-resolution OCT imaging has shown that fluid from an optic pit can enter into and accumulate within many different retinal layers. The intraretinal fluid then may percolate into the subretinal space, sometimes through an outer layer break that may be detectable biomicroscopically, histopathologically, or by OCT. Although the intraretinal fluid communicates with the optic disc cavitation, the submacular fluid typically does not ( Figure 2 ). Only rarely does fluid appear to enter the subretinal space directly from the optic disc without intraretinal fluid accumulation.
Serous maculopathy occurs in more than 50% of eyes with cavitary disc anomalies, with onset typically in early adulthood. However, macular detachment can be seen in early infancy as well as late in life. Detachment typically is confined to the posterior pole, but can be more extensive in some cases, particularly in eyes with large atypical colobomas or morning glory anomaly. Untreated serous maculopathy associated with optic disc pits and related anomalies typically leads to poor visual outcomes. One natural history study of 15 untreated subjects over 9 years reported that 80% lost vision to a level of 20/200 or worse.
Cause of Cavitary Disc Maculopathy
There has been vigorous and long-lasting debate regarding the cause of the maculopathy associated with cavitary disc anomalies. Since Gass proposed in 1969 that cerebrospinal fluid (CSF) from the subarachnoid space migrates into the subretinal space, this has been an area of particular curiosity. Much of what we know about this maculopathy derives from careful clinical examination, histopathologic analysis, and embryologic studies performed in the pre-OCT era. In recent years, OCT technology has expanded our understanding and corroborated earlier hypotheses.
Anatomic Considerations
We endorse a mechanical basis for the serous maculopathy based on congenital structural defects in the optic nerve head. The normal optic nerve exits the eye through a physiologic opening in the eye wall where 2 pressurized, fluid-containing compartments (the vitreous cavity and subarachnoid space) meet each other and abut the retina and the potential subretinal space. Disruption of these normal anatomic features by congenital cavitary defects allows vitreous, CSF fluid, or both to travel down pressure gradients, occasionally into the retinal stroma and subretinal space.
That a similar maculopathy does not occur in normal individuals is testament to the integrity provided by the intricate and robust architecture of the lamina cribrosa and associated tissues of the optic disc. In normal eyes, the 1.2 million retinal ganglion cell axons from the retinal nerve fiber layer converge to form the optic nerve head and exit the globe through the optic nerve. In the prelaminar region, these axons are grouped into 1000 fascicles, separated by glial columns. The glial columns are contiguous with the adjacent collagenous and elastic tissues that surround the optic nerve head and separate it from the adjacent retina and choroid. This elastic tissue seems to provide a fluid barrier as the nerve traverses past the retina and choroid. The axons then pass through the lamina cribrosa to exit the eye. The lamina cribrosa is relatively rigid and, along with its surrounding lining of astrocytic glia, provides a pressure- and water-tight seal between the intraocular and extraocular (including subarachnoid) spaces.
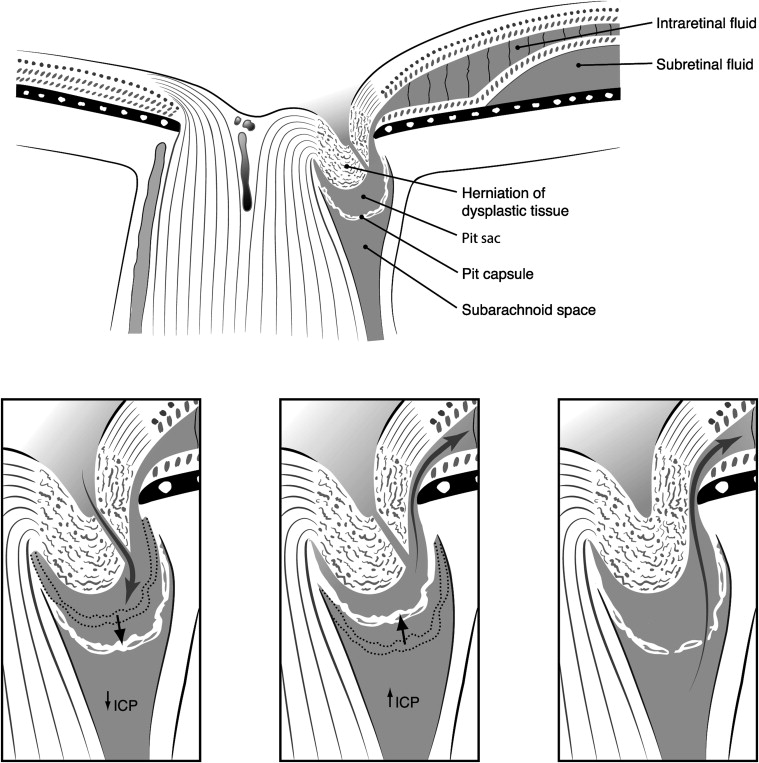
Congenital cavitary anomalies of the optic disc disrupt the intricate organization of axons and connective tissues at this critical juncture where the optic nerve exits the globe. Histologic studies and swept-source OCT imaging reveal that cavitary disc anomalies consist of a herniation of dysplastic retina through a defect in the juxtapapillary sclera, lamina cribrosa, or both into a collagen-lined sac that protrudes into the subarachnoid space. A diaphanous membrane may cover the pit, but defects in this membrane commonly are observed and provide a channel for fluid flow into the pit. As a result of the abnormal anatomic features in affected eyes, the vitreous, subretinal, subarachnoid, and possibly orbital spaces may be variably interconnected through the relatively compliant and porous tissues comprising the excavated disc anomaly.
Source of Fluid
Investigators have proposed many sources of the intraretinal and subretinal fluid in cavitary disc maculopathy, including liquefied vitreous, CSF, and plasma leakage from retinal vasculature, choroid, or orbital tissues. The most plausible fluid sources are the vitreous cavity and subarachnoid space, depending on the particular conformation of the congenital disc pathologic features in each affected eye.
Vitreous cavity
Clinical and experimental studies have demonstrated conclusively a connection between the vitreous cavity and subretinal space in eyes with cavitary disc anomalies. This may account for the observation that the serous maculopathy usually begins in early adulthood, coinciding with the onset of progressive vitreous liquefaction.
Histopathologic studies with Alcian blue have shown vitreous mucopolysaccharides within optic disc pits. India ink studies in Collie dogs with cavitary disc lesions similar to human optic disc pits demonstrated migration of the chromophore into the subretinal space via the disc anomaly. Numerous reports describe the passage of intraocular gas, silicone oil, or other vitreous substitutes into the subretinal or sub–internal limiting membrane (ILM) space in eyes with cavitary disc anomalies. Furthermore, as additional evidence of this connection, surgeons have reported successful drainage of subretinal fluid by aspiration over the disc anomaly.
Vitreous fluid accesses the disc cavitation directly or via small breaks in diaphanous tissue overlying the excavation. Such breaks may be visible clinically or may be detected with OCT imaging of excavated disc anomalies as well as extrapapillary cavitary anomalies. We previously reported the postoperative finding of gas trapped within a disc cavitation, having passed through a small visible break in the overlying neural membrane. As described below, the fact that gas bubbles pass through tiny breaks overlying cavitary disc anomalies provides critical insights into the pathogenesis of the unusual maculopathy in these eyes.
Subarachnoid space
Histologically, congenital anomalous disc cavitations are known to extend posteriorly into the subarachnoid space, and OCT images often show an apparent communication between the macular fluid and a perineural space associated with the disc lesion. Recent imaging with swept-source OCT has shown subarachnoid space immediately posterior to the thin layer of tissue (thought to be pia mater) lining the bottom of the disc excavation. Furthermore, there is unequivocal proof that CSF may access the subretinal space in eyes with cavitary disc anomalies, a fact that may explain cases of serous maculopathy or extensive retinal detachment that occur in infants and young children before the age of significant vitreous liquefaction. Chang and associates describe a case of morning glory disc anomaly with total retinal detachment in which radiopaque dye injected into the subarachnoid space migrated into the subretinal space. Irvine and associates reported a case of morning glory disc where gas in the vitreous cavity was noted to bubble out of the perineural subarachnoid space at the time of optic nerve sheath fenestration. Kuhn and associates describe a patient with bilateral optic nerve pits in whom persistent headache developed as a result of intracranial migration of silicone oil after repair of complex retinal detachment. Patel and associates analyzed subretinal fluid in 2 infants with retinal detachment resulting from optic disc coloboma, finding composition consistent with CSF. In these 2 patients with microphthalmos-coloboma syndrome, the CSF fluid was thought to derive from a retrobulbar optic nerve cyst, a congenital anomaly that occasionally also is seen in association with optic pits.
Although there are relatively few such reports of direct communication between the subretinal space and retrobulbar spaces such as the perineural subarachnoid space and optic nerve cysts, they provide convincing evidence that CSF can access the subretinal space in some eyes with cavitary disc anomalies. In fact, as detailed below, we believe that recognition of anomalous communications between intraocular (vitreous cavity and intraretinal or subretinal) and extraocular (subarachnoid, cyst cavity, or both) spaces is a necessary component of any theory of pathogenesis that purports to explain the unique features of cavitary disc maculopathy. Appreciation of these communications and their anatomic variability also has critical implications for therapeutic approaches to this condition.
Pathogenic Mechanisms
Vitreous traction hypothesis
Several authors have suggested a possible role for vitreous traction in the pathogenesis of serous maculopathy associated with cavitary disc anomalies. Although a precise mechanism has not been elucidated, vitreous traction is believed possibly to induce a small tear in diaphanous tissue overlying the disc excavation, allowing for passage of liquefied vitreous into the retina. Additionally or alternatively, vitreous traction on the peripapillary retina, macula, or both is thought potentially to facilitate the accumulation of fluid in the macula. The following lines of evidence have been offered in support of a vitreous traction mechanism:
- 1.
Posterior vitreous detachment (PVD) typically is absent when the maculopathy first appears, and resolution of serous macular detachment occasionally has been seen after spontaneous PVD.
- 2.
Vitreous and glial tissue abnormalities often are present on or near the optic disc in eyes with pits and other cavitary anomalies. These have been interpreted by some authors as evidence for traction on the roof of the cavitation. For example, unusual vitreous strands may be observed over the optic disc, and an anomalous condensed Cloquet’s canal may be seen terminating at the margin of an optic pit or optic nerve coloboma. Studies using various OCT imaging technologies have demonstrated vitreous strands or glial tissue extending into pits and related anomalies.
- 3.
Pars plana vitrectomy with PVD induction results in resolution of cavitary disc maculopathy in most eyes. Although most of the reported series included barrier laser photocoagulation at the time of surgery, slow resolution of the maculopathy also has been described after vitrectomy alone, without laser photocoagulation or even gas tamponade. Tight vitreous adhesion to the disc margin often is noted during surgery and has been interpreted as evidence for vitreous traction.
- 4.
Macular buckling is successful in most eyes with this condition, possibly by reducing vitreous traction on the juxtapapillary retina and macula. Alternatively, resolution of the maculopathy may result from closure by the buckle of the connection between the optic disc pit and adjacent retina, as originally suggested by the pioneers of this procedure.
Conceptually, there are a number of serious limitations to the vitreous traction hypothesis that can be summarized as follows:
- 1.
Optical coherence tomography images of eyes with definite vitreomacular or vitreopapillary traction show an obvious traction profile, with anteroposterior tissue elevation and sharp angulations at the point of vitreous insertion. However, critical review of OCT images from eyes with cavitary disc anomalies reveals no anterior tenting of the pit roof nor of the peripapillary retina. In 1 study using time-domain OCT, the authors speculated that shallow posterior vitreous separations in 10 of 16 eyes represented vitreomacular traction, but a traction profile was seen in only 1 of these eyes. Other studies using OCT imaging have not shown evidence for vitreomacular traction.
- 2.
All known examples of true vitreous traction are associated with partial PVD states, where traction is exerted by the separating posterior hyaloid membrane on areas of residual vitreoretinal adhesion. However, cavitary disc maculopathy routinely develops long before the earliest stages of partial PVD have begun (including in very young children). Optical coherence tomography images only rarely show partial vitreous separations in eyes with maculopathy. Furthermore, because the posterior hyaloid membrane is absent over the optic disc, it is not anatomically feasible to develop traction by the posterior hyaloid membrane on the tissue overlying cavitary disc anomalies.
- 3.
Tight vitreous adhesion to the immediate peripapillary retina (as noted during surgery in many cases of cavitary disc maculopathy) is a routine finding in normal young eyes and, in the absence of partial PVD, does not imply vitreous traction on the optic disc margin.
- 4.
Surgical removal of glial or vitreous strands found in optic pits does not seem to alter the surgical outcome, as would be expected if traction from these tissues were important in pathogenesis.
- 5.
A vitreous traction model cannot explain the common and frustrating observation of recurrent macular detachment after vitrectomy with peeling of the posterior hyaloid membrane. Neither can it account for maculopathy that develops in eyes with total PVD.
- 6.
Importantly, the vitreous traction hypothesis cannot account for the unique and enigmatic features of cavitary disc anomalies such as subretinal migration of vitreous substitutes and the intermittent sucking of vitreous strands or debris into the pit.
Dynamic pressure gradients
The observation that vitreous substitutes such as gas, silicone oil, and perfluorocarbon liquid can migrate into the subretinal space after vitrectomy in eyes with cavitary disc maculopathy provides critical insight into the pathogenesis of this disorder. As noted above, such migrations clearly prove a communication between the vitreous cavity and subretinal space through the anomalous disc excavation. However, this phenomenon also implies an unusual and complex pathogenesis, because surface tension physics dictate that passage of intravitreal gas through a small opening is not possible without a substantial pressure gradient across the opening. We previously reviewed the relevant surface tension considerations and calculated that the pressure gradient required to push a gas bubble through a generous 200-μm defect in the roof of an optic pit is at least 11 mm Hg.
It is critical to point out that within the closed system of the normal eye, significant pressure differences between various compartments (eg, vitreous cavity and subretinal space) do not exist. For a pressure gradient to be present across the roof of a cavitary disc anomaly, there must be communication with a space outside the eye. Given its close anatomic proximity to optic disc cavitations, the perineural subarachnoid space likely is involved in most cases.
Measured with lumbar puncture in the lateral recumbent position, normal intracranial pressure ranges from 5 to 15 mm Hg, with a mean of 12 mm Hg. Given a mean intraocular pressure of 16 mm Hg, the average pressure gradient across the lamina cribrosa in normal individuals is 4 mm Hg. However, intracranial pressure varies with factors such as body position and venous pressure, and large fluctuations in CSF pressure have been measured in both normal and pathologic situations. Thus, the translaminar (intraocular–intracranial) pressure gradient fluctuates throughout the day and is likely sometimes to be large enough to force gas (or liquid) into a cavitary disc anomaly.
As shown in Figure 3 , intracranial pressure fluctuations can be transmitted to the pit by direct CSF flow if the connective tissue capsule is porous. In cases where the pit capsule is impermeable, pressure alterations may be transmitted via small pressure-induced excursions of the capsule. In this case, the pit may behave as a bulb syringe, drawing fluid (or a vitreous substitute) into the pit sac when intracranial pressure drops, and ejecting it again when CSF pressure rises. Given the variable anatomic features and anomalous interconnections that characterize cavitary disc lesions, the fluid ejected from the pit sac in a given eye could be liquid vitreous, CSF, or even a mixture of the 2 fluids. Repeated small aliquots of fluid driven into the retinal stroma would be expected to cause progressive schisis-like retinal edema and eventually to dissect into the subretinal space.