Parasitic Keratitis and Conjunctivitis
Joseph Tauber
Faisal Jehan
Parasitic ocular infections are a common cause of worldwide ocular morbidity and vision loss. The incidence of parasitic ocular infections is increasing, due in part to the worldwide epidemic of AIDS, the increase in airline travel across the world, increased contact lens wear, and the increase in movement of refugee populations across traditional national boundaries. This chapter is not intended as an encyclopedic review of every known parasite, but instead aims to present and review the major classes of parasitic infections affecting the cornea. Some of the most common parasitic ocular infections, such as toxoplasmosis and toxocariasis, are discussed in separate chapters. Millions of persons worldwide suffer from onchocerciasis, although far fewer are infected with dracunculiasis. The reader interested in rarer entities is referred to textbooks of parasitology (1,2). Parasitic ocular infections are discussed in groups according to the class of infecting organism.
INFECTIONS CAUSED BY PROTOZOA
The most frequently encountered parasitic ocular infections are caused by Protozoan species, including Acanthamoeba, Entamoeba, Microsporidia, the hemoflagellates Trypanosoma and Leishmania, Toxoplasma and Giardia.
Acanthamoeba
Acanthamoeba are small, free-living ubiquitous protozoans that have been isolated from fresh water, sea water, ocean sediment, arctic ice, swimming pool water (even frozen), bottled water, soil, vegetable matter, dialysis treatment units, contact lens cases, and even air (3). One study based on air sampling estimated that a human inhales, on average, two Acanthamoeba organisms per day (4). In contrast to many other protozoans, Acanthamoeba is not naturally parasitic and does not require a host. It feeds on bacteria, fungi, and other organisms and thrives where these microorganisms exist in large numbers, such as in biofilms on the walls of hot tubs. Contact with humans is largely accidental and infection is rare and opportunistic (5). Up to 100% of normal persons demonstrate serum immunoglobulin G (IgG) antibodies against Acanthamoeba species (6). Acanthamoeba has been recovered from human nasal cavities, throats, intestines, lung tissue, and cornea (3,7). Classification of the more than 50 known strains of Acanthamoeba species has been a subject of debate (8,9), but reports classify 22 species into three groups that differ in morphologic characteristics. Because these morphologic characteristics can vary with local environmental conditions, immunofluorescence, isoenzyme profiles, and restriction fragment length polymorphism (RFLP) patterns of whole-cell or ribosomal DNAs have been used in species identification (10, 11, 12, 13).
Acanthamoeba exist in two life forms, an active trophozoite and a dormant cyst. Trophozoites are the infectious form and measure from 15 to 45 μm in diameter. Encystment of trophozoites is the major factor accounting for the severity of Acanthamoeba infections. Encystment occurs as a result of pH changes or adverse changes in oxygen or food supply, but the exact stimulus that directs conversion between life forms in corneal tissue remains unknown (14). The cyst form is slightly smaller than the trophozoite (15 to 28 μm length), double walled, and can remain dormant but viable for years before resuming the trophozoite form (4). Cysts are resistant to wide extremes of temperature, desiccation, and many antimicrobial and disinfectant chemicals that have been shown effective against the trophozoites (15, 16, 17). Cysts may be impervious to inorganic chlorine up to 50 parts per million (ppm), whereas trophozoites are sensitive at 2 ppm, which is still in excess of levels found in public water supplies (<1 ppm) (18). Only some of the known strains of Acanthamoeba are pathologic in humans (A. castellanii, A. culbertsoni, A. hatchetti, A. lugdunensis, A. polyphaga, A. quina, A. rhysodes, A. griffini), possibly due to species differences in tissue adhesion or protease production (18, 19, 20, 21, 22). The earliest reported infections in humans involved the central nervous system (CNS) in immunocompromised patients (3,9), but keratitis due to Acanthamoeba was reported in immunocompetent patients in the early
1970s (23). Cutaneous infections may occur with or without CNS involvement (9).
1970s (23). Cutaneous infections may occur with or without CNS involvement (9).
The first published report of Acanthamoeba keratitis was in 1974 (24). Uncertainty remains about whether earlier cases had gone unrecognized or unreported, or whether this was a new disease. Five retrospective studies of histopathologic specimens identified evidence of only four cases of amebic infection (25, 26, 27, 28, 29). Isolated case reports followed until a relative “epidemic” of cases appeared worldwide, but especially in the United States and Great Britain in the early 1980s, with many of these cases occurring in contact lens-wearing patients (30). Hard, rigid gas-permeable, daily-wear soft, extended-wear soft, and disposable contact lenses have all been associated with Acanthamoeba keratitis, but most cases have involved daily-wear soft contact lenses (31). Often, patients had mixed their own saline solution using large jugs of water and salt tablets or had other nonhygienic lens care habits. Acanthamoeba adherence to contact lens surfaces and contact lens cases is a significant factor in pathogenicity (32). Most commercially available contact lens disinfectants are ineffective at killing Acanthamoeba, although thermal disinfection is reliable (33). As many as 85% of Acanthamoeba keratitis cases occur in contact lens-wearing patients (30), but other risk factors have been defined, including trauma, corneal transplantation, and exposure to infected lake water, sea water, or hot tubs (34, 35, 36). Cases in non-contact lens-wearing patients are most often associated with trauma, exposure to contaminated water or penetrating keratoplasty (37, 38, 39, 40). Many idiopathic cases have also been reported. The incidence of Acanthamoeba keratitis has been estimated between 1.2 and 3.0 cases per million (41).
Variability in presentation is one of the hallmarks of Acanthamoeba keratitis. Severe pain, frequently in excess of objective findings, is a common feature (42), as are symptoms of foreign-body sensation, photophobia, and tearing (42). The majority of cases are unilateral, but bilateral cases have been reported in 7.5% of cases (41).
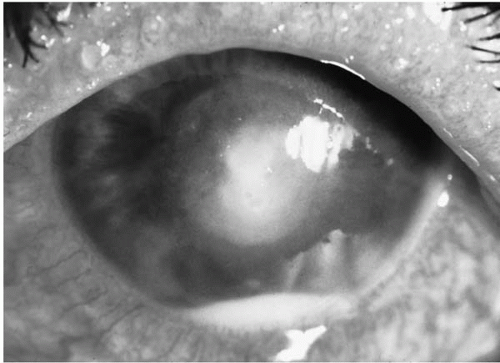 FIGURE 17-1. Acanthamoeba keratitis with hypopyon. |
Clinical signs vary with the stage of presentation, and disease progression is often slow. In very early corneal infection, only conjunctival hyperemia with superficial epithelial irregularities (microerosions, pseudodendrites, opacification, microcystic edema, or a diffuse granularity) may be seen (4,43). Despite corneal hypesthesia, severe pain thought to be secondary to keratoneuritis is common. In later stages, multifocal, nummular anterior stromal infiltrates develop, and may coalesce into annular or crescentic opacities (Fig. 17-1). Disciform keratitis may occur. A ring infiltrate, initially vague, with intact central epithelium, has been described by some as pathognomonic of Acanthamoeba keratitis (44). In later stages, the ring often appears more dense and discrete, and the central epithelium sloughs, facilitating stromal necrosis. Anterior chamber reaction is rare. The pathogenesis of the ring infiltrate is uncertain. Residual antigen may cause inflammation in the absence of active trophozoite infection. Cysts have been shown to induce corneal stromal inflammation as long as 31 months following antiamebic therapy (45). Focal stromal edema with intrastromal inflammatory infiltration is common and radially oriented perineural infiltration (keratoneuritis) has been described (43) (Fig. 17-2).
Later, continued inflammation and presumed release of proteases and collagenases lead to stromal lysis and sometimes to descemetocele formation or perforation. Less common sequelae may include secondary immune-mediated scleritis (46), iritis (47), and corneal neovascularization.
Chorioretinitis following keratitis (48) and a culture-positive anterior chamber paracentesis (49) have been reported. Herpetic keratitis is often the most commonly considered differential diagnosis, and may delay the diagnosis of Acanthamoeba infection (50). The appearance of satellite lesions in later stages can mimic fungal keratitis. In some studies, the mean delay to diagnosis was 42 to 48 days (51,52) and may be longer in non-contact lens-wearing patients (53). Clinical signs in Acanthamoeba keratitis are listed in Table 17-1.
Chorioretinitis following keratitis (48) and a culture-positive anterior chamber paracentesis (49) have been reported. Herpetic keratitis is often the most commonly considered differential diagnosis, and may delay the diagnosis of Acanthamoeba infection (50). The appearance of satellite lesions in later stages can mimic fungal keratitis. In some studies, the mean delay to diagnosis was 42 to 48 days (51,52) and may be longer in non-contact lens-wearing patients (53). Clinical signs in Acanthamoeba keratitis are listed in Table 17-1.
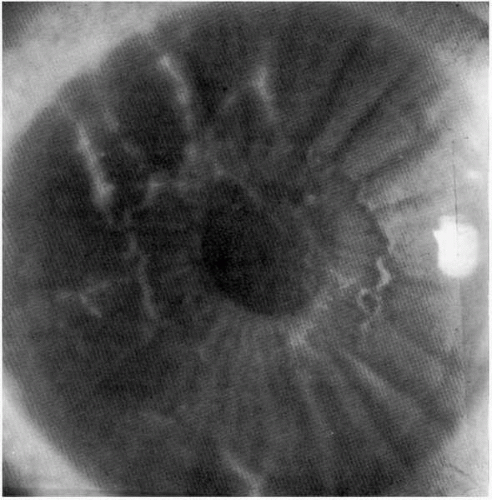 FIGURE 17-2. Perineural infiltrates during early stage of Acanthamoeba keratitis. |
TABLE 17-1. REPORTED FREQUENCIES OF CLINICAL SIGNS IN ACANTHAMOEBA KERATITIS | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Diagnosis
Accurate diagnosis of Acanthamoeba infection requires microbiologic confirmation and should not be made wholly on clinical grounds. All available sources for culture should be exploited, including contact lens solutions and cases, well water, or hot tub water samples. Diagnosis is most often confirmed by direct inoculation of corneal scrapings onto appropriate culture media or submission of scrapings from the base of ulcers for histopathologic examination. Sometimes, direct incision into the stroma to reach deeper infiltrates or excisional corneal biopsy is necessary to obtain adequate tissue samples. Corneal buttons obtained at the time of keratoplasty should always be submitted for both histopathologic examination and culture. Recently, confocal microscopy has been reported as a tool to identify cysts or trophozoites in vivo (54,55), but debate about the validity of these findings has tempered early enthusiasm about this technology as a noninvasive diagnostic tool.
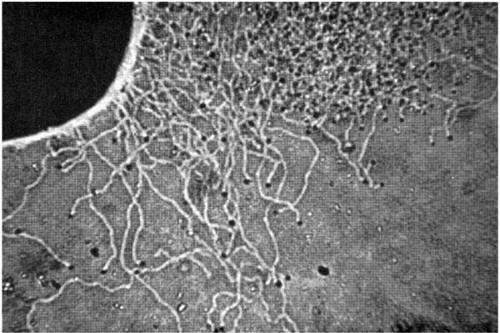 FIGURE 17-3. Migration of Acanthamoeba organisms on a culture plate. |
Culture specimens should be directly inoculated onto culture media at the slit lamp or in the operating room. Acanthamoeba organisms grow poorly on media typically used for bacterial keratitis sampling (blood agar, chocolate agar, Sabouraud agar). Early reports recommended culture on nonnutrient agar seeded with an overlay of bacteria, usually gram-negative rods (e.g., Escherichia coli, Enterobacter aerogenes, Klebsiella pneumoniae, or Xanthomonas maltophilia). Examination of culture plates reveals “trails” that motile trophozoites leave on the agar surface as they ingest bacteria (Fig. 17-3). Acanthamoeba will grow on commercially available buffered charcoal yeast extract (BCYE) (56) and tryptic soy agar with horse or rabbit blood (57). In one review of 106 cases, 43.4% of cases were culture positive (52).
Histopathologic studies have demonstrated both trophozoites and cysts using methenamine-silver, periodic acid-Schiff (PAS), Masson trichrome, and iron-hematoxylin-and-eosin stains (58,59). Fluorescent microscopy can be done using calcofluor white, fluorescein-conjugated lectins such as
concanavalin A and wheat-germ agglutinin, and immunofluorescent stains, and immunoperoxidase staining is available (3,60, 61, 62). A reculture technique has been proposed as a laboratory standard for in vitro sensitivity testing (63), but is not widely performed (64). Both trophozoiticidal and cysticidal concentrations can be measured, but correlation with clinical efficacy has not been demonstrated.
concanavalin A and wheat-germ agglutinin, and immunofluorescent stains, and immunoperoxidase staining is available (3,60, 61, 62). A reculture technique has been proposed as a laboratory standard for in vitro sensitivity testing (63), but is not widely performed (64). Both trophozoiticidal and cysticidal concentrations can be measured, but correlation with clinical efficacy has not been demonstrated.
Treatment
Early reports of Acanthamoeba keratitis treatment were characterized by failures of medical treatment, recurrence following surgical intervention, and frequent loss of vision. Some medical cures were reported with combinations of amebicidal drugs (65, 66, 67, 68, 69), but treatment failures were common and prolonged duration of therapy was required (50,70,71). Better results were achieved when treatment was begun early in the course of disease (70,72).
Medical therapy has employed aminoglycosides, polymeric biguanides, diamidines, and imidazoles, usually in combinations (43,69). Most of these medications are prescribed to be instilled initially every hour and then slowly tapered. To date, no report has recommended standardization of the therapeutic regimen (73). Among the aminoglycosides, neomycin, commercially available as an 8-mg/mL solution or fortified to 20 mg/mL, has been demonstrated to have antiamebic efficacy. Paromycin 10 mg/mL has also been used. Polymeric biguanides, commercially available as environmental biocides (Baquacil, a swimming pool disinfectant), have been used with success in the treatment of Acanthamoeba keratitis (43,69). Diluted to a 0.02% concentration, progressive ocular surface toxicity often forces discontinuation of therapy. The mechanism of action of this agent is believed to be interference with cytoplasmic membrane integrity and inhibition of essential respiratory enzymes (69). Chlorhexidine 0.02% to 0.1% is another cationic antiseptic agent that has shown good efficacy at eradicating Acanthamoeba, and it also acts by disrupting membrane function (63,74). Because of the lower surface toxicity as compared with polyhexylmethylbiguanide (PHMB), chlorhexidine has emerged as a favored treatment, whether alone or in combination with other agents (43). Aromatic diamidines such as Brolene (propamidine isethionate 0.1% solution), pentamidine isethionate, and dibromopropamidine ointment are available in eyedrop or ointment preparations. These agents act by inhibition of S-adenosylmethionine decarboxylase or by direct interaction with amebic nucleic acids (63). Limited bioavailability, induction of encystment, and acquired resistance have all been suggested as causes of treatment failures with Brolene. Imidazoles, which also act by affecting membrane permeability, have been used both as topical preparations and systemically administered (75). Oral therapy with itraconazole or ketoconazole may have an important role in adjunctive therapy. Miconazole 1% to 2% and clotrimazole 1% to 2% have been used in therapy with success, but ocular surface toxicity is common and these drugs are amebistatic rather than amebicidal (76).
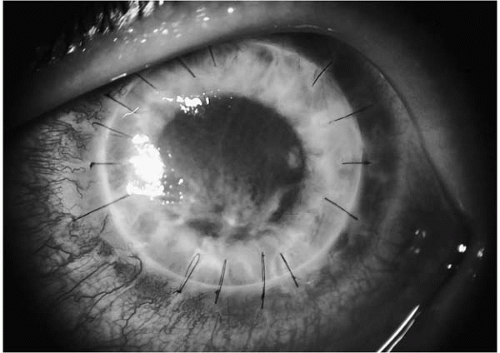 FIGURE 17-4. Recurrent Acanthamoeba keratitis following second keratoplasty in a 29-year-old contact lens wearer. |
As is true in other infectious scenarios, the role of topical corticosteroids is controversial. Controlling the severe stromal and scleral inflammatory process is important, but inhibition of host defense mechanisms may prolong the course of disease or even significantly worsen outcomes (77,78). Some reports have indicated worse outcomes in cases of early steroid use, and have recommended delaying steroids until after effective antiamebic therapy is confirmed. Steroids have been shown to promote conversion of cysts to trophozoites (79).
Surgical intervention should be delayed until there is clear evidence of control of amebic replication, and should not be employed as a strategy to debulk the cornea of amebic load (80). Penetrating keratoplasty is occasionally required to maintain the structural integrity of the globe (81), but vigorous attempts should be made to forestall surgical intervention as long as possible (9,82). Recurrence of disease following penetrating keratoplasty has been frequently reported (43,82), often as a crescentic infiltrate near the graft—host junction, and results in reduced likelihood of vision preservation (Fig. 17-4). As in cases of fungal keratitis, postoperative treatment with topical cyclosporine is recommended for prophylaxis against rejection rather than topical steroids. Penetrating keratoplasty is best reserved for optical rehabilitation in quiescent, medically cured eyes (82).
Entamoeba histolytica Infections
Entamoeba species are endemic worldwide, but thrive in contaminated water supplies in areas of poor sanitation. Entamoeba species exist in three life forms: a trophozoite (12-60 μm), precyst, and cyst (10-20 μm). The most common route of infection is fecal to oral transmission.
Infection follows ingestion of even small numbers of cysts. Excystment occurs in the small intestine, but trophozoite maturation and encystment occur in the large intestine. Gastrointestinal infection is the most common clinical presentation of infection, but extragastrointestinal spread occurs. Entamoeba histolytica has been reported to infect the external tissues of the eye, presumably following fecal-ocular transmission (83).
Infection follows ingestion of even small numbers of cysts. Excystment occurs in the small intestine, but trophozoite maturation and encystment occur in the large intestine. Gastrointestinal infection is the most common clinical presentation of infection, but extragastrointestinal spread occurs. Entamoeba histolytica has been reported to infect the external tissues of the eye, presumably following fecal-ocular transmission (83).
Diagnosis is made on the basis of direct visualization of trophozoites in infected material, usually stool specimens. Trichrome, iron-hematoxylin, PAS, and immunofluorescence techniques have all been used to enhance detection of entamoebic trophozoites. Serologic tests are available, but their usefulness in the diagnosis of ocular entamoebiasis is unknown.
Microsporidiosis
Microsporidia are ubiquitous, obligate intracellular spore-forming protozoan parasites, prevalent in numerous wild and domesticated animal hosts (84). Microsporidia organisms exist in three developmental stages within infected cells: infective, proliferative (binary or multiple fission), and sporogony. Sporogony results in spore production, ranging from 1 to 20 μm, with the coiled polar filament or tubule characteristic of Microsporidia. Classification of over 100 species into 144 genera is made by morphologic features such as the number of coils, number of nuclei, or presence of vacuoles (85,86).
Only five genera of Microsporidia are known to cause human disease (Nosema, Encephalitozoon, Enterocytozoon, Pleistophora, and Septada) (87). Most cases have involved immunocompromised hosts, especially AIDS patients (88, 89, 90), though sporadic cases have occurred in immunocompetent patients (91). Microsporidia infections are usually transmitted by fecal-oral, transplacental, or transovarial routes; ocular infection more often occurs by direct inoculation. Enteritis is the most common manifestation of human Microsporidia infection, occurring in as many as 30% of AIDS patients (86), but disseminated infections may produce peritonitis, sinusitis, pulmonary, renal, cardiac, hepatic, or CNS disease (86,90,92).
Microsporidia keratitis was first reported in 1990, although there were prior case reports of ocular infection (93). Ocular disease is most common in AIDS patients or following trauma (94, 95, 96, 97, 98). Ocular findings of microsporidial infection include conjunctival injection, mixed follicular-papillary tarsal conjunctival reaction, and punctate epithelial keratopathy. Most cases present as a coarse, granular epithelial keratitis with small foci of anterior stromal infiltration (Fig. 17-5). Hyphema and necrotizing keratitis have been reported (85).
Two clinical presentations of Microsporidia keratitis have been described. Immunocompromised or AIDS patients usually present with bilateral conjunctival inflammation and coarse epitheliopathy usually related to Encephalitozoon spp. (96,99,100), thought to reach the cornea through systemic dissemination. The characteristic coarse or punctuate epitheliopathy may extend to the limbus, but significant stromal involvement, bacterial superinfection, or iritis is rare. Healthy immunocompetent patients may present with unilateral conjunctival inflammation with focal stromal keratitis, usually related to exogenous infection with Nosema spp. (94,95). Stromal involvement may extend to deeper layers, taking on a disciform appearance similar to herpetic keratitis.
 FIGURE 17-5. Microsporidial keratoconjunctivitis presenting as punctate epithelial keratopathy. (From Lowder CY, et al. Microsporidia infection of the cornea in a man seropositive for human immunodeficiency virus. Am J Ophthalmol 1990;109:242. Published with permission from the American Journal of Ophthalmology. Copyright by the Ophthalmic Publishing Company.) |
Diagnosis requires demonstration of oval Microsporidia spores in specimens obtained during superficial corneal scraping, or more rarely from biopsy. Spores stain gram positive and may show a PAS-positive body at one end of the oval spore, but staining is variable with routine methods such as Giemsa, Gomori silver, or acid-fast staining. Calcofluor white staining is better for light microscopic diagnosis, but electron microscopy is preferred for revealing the characteristic coiled tubules within the spore coat of Microsporidia. Without electron microscopy, spores may be confused with Toxoplasma gondii, Histoplasma capsulatum, or Leishmania (101). Polymerase chain reaction (PCR) is available as a diagnostic research tool only. Serologic testing and culture are unreliable (86,94,102,103).
Reports of medical treatment of Microsporidia keratitis have demonstrated poor results with topical antibiotics, metronidazole, or thiabendazole, but better results with topical propamidine isethionate 0.1% (Brolene) (99) or
topical fumagillin (91,101,104,105). Benzimidazoles such as albendazole have a long history of use against numerous helminthic infections, but have resulted in inconsistent clearing of Microsporidia infections (86). Fumagillin is an antiamebic compound isolated from Aspergillus fumigatus in 1949. The mechanism of action of fumagillin is not well understood (86). In AIDS patients, best results have been reported with topical fumagillin or systemic albendazole (106), but successful reports of treatment with metronidazole and oral itraconazole have been published (86,100). There is no validated model for in vitro sensitivity testing. Surgical treatment for significant stromal involvement involving penetrating keratoplasty with cryotherapy has been reported (90,107,108).
topical fumagillin (91,101,104,105). Benzimidazoles such as albendazole have a long history of use against numerous helminthic infections, but have resulted in inconsistent clearing of Microsporidia infections (86). Fumagillin is an antiamebic compound isolated from Aspergillus fumigatus in 1949. The mechanism of action of fumagillin is not well understood (86). In AIDS patients, best results have been reported with topical fumagillin or systemic albendazole (106), but successful reports of treatment with metronidazole and oral itraconazole have been published (86,100). There is no validated model for in vitro sensitivity testing. Surgical treatment for significant stromal involvement involving penetrating keratoplasty with cryotherapy has been reported (90,107,108).
Hemoflagellate Infections
The hemoflagellates include the Trypanosoma and Leishmania species as well as Toxoplasma and Giardia. Different life forms present within each species.
Trypanosomes
Two distinctive diseases caused by Trypanosoma species have been well described. Over 10 million people in Latin America are thought to be infected with Chagas’ disease or trypanosomiasis, caused by Trypanosoma cruzi. The organism lives within the gastrointestinal system of the reduvid bug and is passed into the feces. During feeding, the bug defecates and organisms gain entry into fresh bite wounds. Transmission of infection has also been reported transplacentally, via consumption of contaminated foods, blood transfusions, breast-feeding, and laboratory accidents. Clinical disease is usually cutaneous, characterized by the chagoma or hard cutaneous nodule. Once the parasite enters the bloodstream, generalized lymphadenopathy, splenomegaly, hepatomegaly, myocarditis, or meningoencephalitis may result. Most patients recover within months, but fatal cases have been reported. Ocular involvement is usually eyelid swelling or chagoma of the lid or lacrimal gland (109). Conjunctival edema and erythema or dacryoadenitis may be associated with generalized lymphadenopathy.
African trypanosomiasis, or African sleeping sickness, is caused by Trypanosoma brucei gambiense and Trypanosoma brucei rhodesiense. Transmission is via the bite of the tsetse fly in sub-Saharan Africa. Systemic disease may present in various ways, including meningoencephalitis, myocarditis, hepatosplenomegaly or cutaneous nodules. Central nervous system involvement may follow lymphatic spread of trypanosomes. Ocular involvement is usually eyelid edema (110). Interstitial keratitis and anterior uveitis have been described (110,111).
Laboratory diagnostic methods include examination of wet mounts of whole blood or Giemsa staining of blood smears, buffy coat, or cerebrospinal fluid samples to identify extracellular trypanosomes. If involved, lymph node aspirates or biopsies, bone marrow biopsies, or biopsy of cutaneous lesions may yield organisms. Trypanosomes can be cultured on Novy-MacNeal-Nicolle agar or in tissue culture (112), but standardized techniques remain in development. Serologic testing is available but infrequently used. Enzyme-linked immunosorbent assay (ELISA), indirect immunofluorescence, radial immunodiffusion, immunoprecipitation, and indirect agglutination are useful epidemiologic tools, although they are not presently standardized (113).
Systemic treatment with oral nifurtimox or benzimidazole is effective in early stages of American trypanosomiasis. For African trypanosomiasis, early-stage parenteral therapy includes suramin or pentamidine. Systemic treatment can limit corneal scarring and neovascularization if stromal keratitis is present. Intravenous medication is used for central nervous system involvement.
Leishmaniasis
Leishmaniasis is considered by the World Health Organization (WHO) as one of the six major tropical diseases. There are estimated to be 10 million to 12 million infected persons worldwide, with about 2 million new cases recognized annually and nearly 400 million people at risk for infection (114). Leishmaniasis is classified into Old and New World cutaneous leishmaniasis, mucocutaneous, and visceral leishmaniasis (kala-azar), each caused by various Leishmania species with unique animal reservoirs and insect vectors. Despite attempts at controlling the disease, new endemic areas have developed due to immigration (115) between developing countries. There are endemic areas on every continent except Australia (116), but especially in India and Afghanistan, the rural Middle East, Northern and Eastern Africa, and South America. Cases of a variant of visceral leishmaniasis were reported among American military personnel after Operation Desert Storm (117). Leishmaniasis is transmitted through the bite of Phlebotomus or Lutzomyia species sandflies.
Leishmania spp. exist in two forms, the promastigote or infective stage, and the amastigote stage, which undergoes intracellular binary fission after phagocytosis by circulating macrophages. Local replication of organisms results in papular lesions that may granulate or ulcerate. Transport of infected macrophages via the lymphatic system may lead to distant subcutaneous nodules or lymphangiitis. Systemic dissemination (visceral leishmaniasis) via the reticuloendothelial system leads to hepatosplenomegaly, hypersplenism, and secondary pancytopenia.
Leishmaniasis of the eye is extremely rare (118, 119, 120, 121, 122, 123). Visceral leishmaniasis has been associated with retinal hemorrhages and anterior uveitis, whereas cutaneous and mucocutaneous infections have been mostly associated with eyelid manifestations (116). Cutaneous leishmaniasis
may involve any area of exposed skin, but involves the eyelid only rarely, thought likely due to lid movement during blinking (120,124,125). Solitary or multiple lesions on the face or extremities are typical (120,121,126). Cicatricial entropion or ectropion may result from prolonged lid inflammation. Eyelid lesions may progress to conjunctival involvement, with granuloma formation or chronic conjunctivitis with scarring (109,120,127,128). Progressive disease can involve the lacrimal drainage structures and can produce cicatricial entropion or ectropion. The cornea may be involved via hematogenous spread of organisms or via contiguous spread of disease from the eyelids, beginning with punctate epithelial keratitis and progressing to limbal keratitis or generalized stromal keratitis with neovascularization and scarring (128,129). Necrosis may develop leading to ulceration and perforation, necessitating enucleation (130). Three additional cases have been reported leading to blindness (131).
may involve any area of exposed skin, but involves the eyelid only rarely, thought likely due to lid movement during blinking (120,124,125). Solitary or multiple lesions on the face or extremities are typical (120,121,126). Cicatricial entropion or ectropion may result from prolonged lid inflammation. Eyelid lesions may progress to conjunctival involvement, with granuloma formation or chronic conjunctivitis with scarring (109,120,127,128). Progressive disease can involve the lacrimal drainage structures and can produce cicatricial entropion or ectropion. The cornea may be involved via hematogenous spread of organisms or via contiguous spread of disease from the eyelids, beginning with punctate epithelial keratitis and progressing to limbal keratitis or generalized stromal keratitis with neovascularization and scarring (128,129). Necrosis may develop leading to ulceration and perforation, necessitating enucleation (130). Three additional cases have been reported leading to blindness (131).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


