Key points
- •
Uvulopalatoplasty is used to treat patients with obstructive sleep apnea (OSA) who have narrowing of the retro-palatal area of the pharynx.
- •
There have been many descriptions of procedures for the palate to decrease its length and move it anteriorly to increase the anterior posterior dimensions of the inferior margin of the palate.
- •
New techniques using radio frequency, laser, and implants have been used for snoring and OSA; but results have been similar to more surgically oriented techniques.
The procedure uvulopalatopharyngoplasty (UPPP) was first described for the treatment of snoring by Ikematsu in 1964. Much later, in 1981, UPPP was described by Fujita and colleagues as “a new surgical approach” to treat obstructive sleep apnea. Until then, permanent tracheostomy had been the only consistently effective surgical treatment in adult sleep apnea but resulted in psychosocial issues that were unacceptable to many patients. Fujita and colleagues described 12 predominantly male (11 of 12) patients with a history of excessive daytime sleepiness and loud habitual snoring. The velopharyngeal space was identified as the area of functional collapse of the pharynx during apneas. Clinically, the patients had a shallow oropharyngeal space with a relatively large uvula and redundant mucosa of the surrounding tissue.
Fujita and colleagues subsequently described a series of 66 patients (63 men) treated for obstructive sleep apnea with UPPP. The mean apnea index (AI) preoperatively was 59. Significant improvements occurred after UPPP, although great variability was noted in individual patient response. Two subgroups were identified: responders (33 of 66) showed a significant decrease in AI of 84% (58.3–9.5), whereas nonresponders had little improvement (60.3–55.4). Despite recognizing the clear variability in response, they were unable to identify a sleep or respiratory parameter that differentiated the response to UPPP.
Some explored whether patients with mild sleep apnea might be more likely to benefit from surgical treatment. In an evaluation of 37 unselected patients with mild obstructive sleep apnea who underwent UPPP, Senior and colleagues found that only 40% had at least a 50% postoperative reduction in the respiratory event index (REI). Other patients had an increase in average REI from 161.6 ±5.0 to 26.7 ±18.4. Subjective assessment of sleepiness similarly was not improved. Again, the issue of responders and nonresponders arose.
In a review of the literature, Sher and colleagues noted that reports of case series and few controlled trials tend to limit the ability to advocate for change in surgical practice across the specialty. Their review found that UPPP was effective, at best, in less than 50% of patients with obstructive sleep apnea.
The variability in results of UPPP and the inability to predict which patients would respond to surgery became frustrating to otolaryngologists as many sleep medicine physicians refrained from referring patients for surgical interventions. Because of a success rate that was quoted as a 50:50 chance of improvement, many otolaryngologists attempted to improve surgical success results and to decrease the postoperative period in patients with obstructive sleep apnea with modifications of the traditional UPPP.
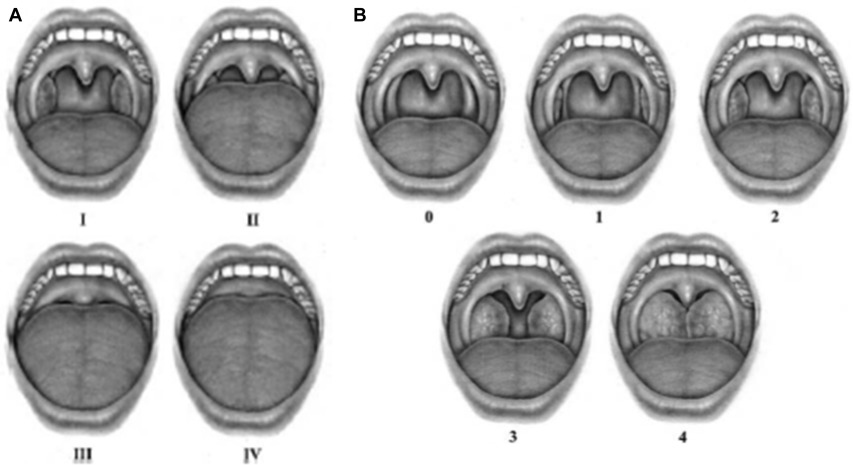
A breakthrough began when Friedman and colleagues classified patients with obstructive sleep apnea with a staging system based on body mass index (BMI), tonsil size, and palate position. Stage I was defined as a palate position 1 or 2 combined with tonsil size 3 or 4. Stage II was defined as palate position 3 or 4 and tonsil size 3 or 4. Stage III patients had palate position 3 or 4 and tonsil size 0, 1, or 2. Any patient with a BMI greater than 40 was stage III. In a retrospective analysis, UPPP alone had an 80% success rate in stage I patients, 37.9% success in stage II, and 8.1% success in stage III ( Fig. 1 , Table 1 ).
| Friedman Tongue Position | Tonsil Size | BMI | |
|---|---|---|---|
| Stage I | 1 | 3, 4 | <40 |
| 2 | 3, 4 | <40 | |
| Stage II | 1, 2 | 0, 1, 2 | <40 |
| 3, 4 | 3, 4 | <40 | |
| Stage III | 3, 4 | 0, 1, 2 | <40 |
| Any | Any | >40 |
Multiple palatal procedures were developed to improve surgical success. An attempt to review all published procedures would be difficult because most are single series by individual surgeons and did not include large enough numbers or the technique was not adopted by others to reach significance within the specialty. Some of the procedures included new technology that was developed or applied in a novel way.
Uvulopalatopharyngoplasty
Fujita described the UPPP as a procedure to remove redundant mucosa and preserve the muscular layer to enlarge the oropharyngeal space. The procedure required general anesthesia, and patients were admitted to the hospital. The UPPP was performed by making an incision through the mucosa of the soft palate lateral to the glossopalatal arch from the inferior pole of the tonsillar fossa toward the uvula ending at its tip. The incision was extended on the pharyngeal side of the uvula and the pharyngopalatal arch toward the inferior pole of the tonsil. The mucosa of the soft palate, tonsillar fossa, and the lateral aspect of the uvula were undermined with sharp dissection and excised. The mucosal edges between the anterior and postural palatal arches were reapproximated with interrupted sutures. This maneuver brought the palatal arch forward or anteriorly with an increase in the anterior posterior dimension of the oropharyngeal space. If the uvula was elongated with the maneuver, then it was shortened or removed. If redundant tissue was in the posterior pharyngeal wall, an additional excision of the posterior pharyngeal mucosa could be done. The posterior pharyngeal mucosa was elevated and stretched laterally and sutured ( Fig. 2 ).
Uvulopalatopharyngoplasty
Fujita described the UPPP as a procedure to remove redundant mucosa and preserve the muscular layer to enlarge the oropharyngeal space. The procedure required general anesthesia, and patients were admitted to the hospital. The UPPP was performed by making an incision through the mucosa of the soft palate lateral to the glossopalatal arch from the inferior pole of the tonsillar fossa toward the uvula ending at its tip. The incision was extended on the pharyngeal side of the uvula and the pharyngopalatal arch toward the inferior pole of the tonsil. The mucosa of the soft palate, tonsillar fossa, and the lateral aspect of the uvula were undermined with sharp dissection and excised. The mucosal edges between the anterior and postural palatal arches were reapproximated with interrupted sutures. This maneuver brought the palatal arch forward or anteriorly with an increase in the anterior posterior dimension of the oropharyngeal space. If the uvula was elongated with the maneuver, then it was shortened or removed. If redundant tissue was in the posterior pharyngeal wall, an additional excision of the posterior pharyngeal mucosa could be done. The posterior pharyngeal mucosa was elevated and stretched laterally and sutured ( Fig. 2 ).
The uvulopalatal flap
The uvulopalatal flap (UPF) was reported by Powell and colleagues who used a technique to advance the uvula and distal palate by creating a flap of tissue that was reversed on itself and sutured close to the hard palate. The advancement flap started with the ventral surface of the soft palate, and the uvula had the mucosa removed and was sutured in place. An incision was made that also released the lateral aspects of the palate. Huntley’s drawings described the steps of the procedure very well (see Fig. 2 ). Initially, local anesthetic with a vasoconstrictor was injected in the ventral surface of the soft palate and uvula to assist with separating a plane between the muscular layer and the mucosa, which also helped with pain control and hemostasis. The soft palate and uvula were retracted toward the hard palate to allow an outline to be drawn for the incision. The ventral mucosa was removed, and relaxing incisions were made at the lateral aspect to provide greater anterior release of the UPF and increase the retro-palatal area. The palate was then folded on itself, and the mucosa of the dorsal palate and uvula was sutured into position.
The procedure can be done as an outpatient or under general anesthesia. An advantage was that the procedure was potentially reversible if velopharyngeal insufficiency occurred. Because muscular tissue was not removed, the normal physiologic mobility of the palate was maintained and the likelihood of scar contracture and subsequent nasopharyngeal stenosis would be decreased. An important additional benefit was a decrease in postoperative pain because there was no disruption of muscle tissue or presence of denuded surfaces.
An extended UPF (EUPF) described by Li and colleagues included the previous procedure but used dissection and removal of submucosal adipose tissue of the soft palate and supratonsillar area ( Fig. 3 ). The EUPF was done in conjunction with tonsillectomy. The EUPF was done under general anesthesia, and in their series there was one occurrence of bleeding from the tonsillar fossa during the postoperative period and 3% of patients had occasional nasal regurgitation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


