Purpose
To describe the clinical implications of outer foveolar defects on optical coherence tomography (OCT) in eyes treated surgically for macular hole (MH).
Design
Retrospective observational case series.
Methods
Ninety-six eyes of 93 subjects who had undergone surgery for the treatment of idiopathic MH were included. Clinical data, including OCT prior to and at follow-up visits ranging from 3 to 32 months after surgery, were analyzed. Incidence, risk factors, and clinical outcomes of outer foveolar defect were evaluated.
Results
Outer foveolar defects were noted on postoperative OCT in 44 of the 96 eyes (45.8%). The mean preoperative diameter of MH in the eyes (333.5 ± 126.3 μm) evidencing outer foveolar defects was significantly smaller than those that did not (504.2 ± 155.6 μm) ( P < .0001). The mean disappearance time of the defect was estimated to be 182 days after surgery. The mean postoperative visual acuity (logMAR) improved to 0.40 ± 0.26 from 0.58 ± 0.23 after the disappearance of outer foveolar defects.
Conclusions
Outer foveolar defects were detected predominantly after surgery for small MHs. The defect decreases gradually in size and eventually disappears completely approximately 6 months after surgery.
Macular hole (MH) is characterized by a central, full-thickness retinal defect, which induces central visual loss. Idiopathic MH has received a great deal of attention in recent years, owing primarily to improved ability to achieve closure and restoration of visual function via surgery. Optical coherence tomography (OCT) has significantly broadened our understanding of the pathogenesis, management, and prognosis of this disorder. Multiple foveal abnormalities observed by OCT have been described after MH surgery. Among them, the postoperative OCT features of outer foveolar defects have been referred to variously as “tissues of bridge,” “foveolar lucencies,” “foveolar cysts,” “foveolar detachments,” or “outer retinal defects” in previous studies. Although the occurrence of this phenomenon is common, its clinical significance, including its prognostic value, risk factors of its development, and implications on the MH sealing process, has yet to be clearly elucidated.
The principal objective of this study was to evaluate the incidence, risk factors, and clinical outcomes of outer foveolar defects after surgery for the treatment of idiopathic MH.
Methods
This was a retrospective study of a consecutive series of patients undergoing surgeries for idiopathic MH between January 2005 and July 2007 at the Samsung Medical Center. For inclusion in the study, the follow-up period had to be at least 3 months after the surgery. The preoperative data included complete medical histories; ophthalmologic examination including the measurement of intraocular pressure, refraction, and best-corrected Snellen visual acuity (BCVA); and biomicroscopic examination of the lens status, vitreous, and fovea.
Surgical procedures were conducted in all cases by a single surgeon (S.W.K.) and involved standard pars plana vitrectomy, the induction of a posterior vitreous detachment with posterior vitreous detachment (if not already present), the removal of the posterior cortical vitreous, the peeling of the internal limiting membrane around the MH, and a complete fluid-gas exchange. Selection of the gas for intraocular tamponade depended principally on the size of the MH. For MHs smaller than 400 μm in diameter, 25% SF 6 gas was usually injected. For larger holes, 14% C 3 F 8 gas was usually employed. Silicone oil was injected in 1 case, because the patient was unable to maintain a face-down position because of a systemic condition. All patients except the aforementioned were instructed to maintain a face-down position for at least 7 days postoperatively. Follow-up examinations were conducted at 1- to 3-week intervals in the first 2 months after the operation, and at intervals of 2 or 3 months thereafter. In cases in which lens opacification impaired the visualization of fundus detail, phacoemulsification and intraocular lens implantation was jointly conducted (14 eyes). During the follow-up period, patients who developed visually significant cataracts underwent cataract surgery (59 eyes).
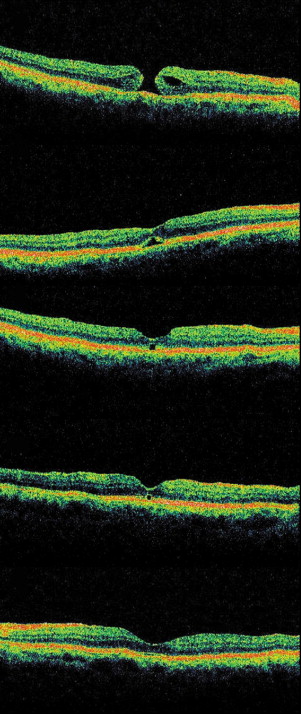
The OCT (Model 3000; Carl Zeiss Meditec, Dublin, California, USA) examination was conducted at each follow-up and included the measurement of 3 MH parameters: minimum diameter of the MH (MH diameter), diameter of the MH at the level of the retinal pigment epithelium (RPE) (hole base diameter), and distance from the RPE to the innermost aspect of the MH (MH height). We calculated 1) the MH index, the ratio of the MH height to the hole base diameter, as described by Kusuhara and associates, 2) diameter hole index (the ratio of the MH diameter to the hole base diameter), and 3) the ratio of the minimum diameter to the hole base diameter, as previously described by Ruiz-Moreno and associates. The central foveolar thickness was defined as the distance between the innermost foveolar surface and the outermost foveolar surface, and was measured via a manually assisted technique outlined by the OCT system software. The sealed MHs were subdivided into 3 types, according to the OCT classifications described in a previous report: the U-shaped closure, which describes a normal foveal contour; the V-shaped closure for a steep foveal contour; and the flat-open closure, in which a foveal defect of the neurosensory retina persists postoperatively, although the whole rim of the MH is attached to the underlying RPE with flattening of the cuff. All cases were assessed by 1 masked observer (J.W.L.). The outer foveolar defect was defined as lucencies of the outer foveal layer on postoperative OCT, in the eyes with sealed MH. The representative case is shown in Figure 1 .
SPSS software version 12.0 for Windows (SPSS, Inc, Chicago, Illinois, USA) was used for statistical analysis. Snellen visual acuity was converted to a logarithm of the minimal angle of resolution (logMAR) for statistical analysis. Categorical analysis was conducted using the 2-tailed t test, χ 2 test, Mann-Whitney U test, or Fisher exact test, as appropriate. Data were analyzed via repeated-measures analysis of variance with Bonferroni correction. Correlation analyses were conducted via Spearman correlation. The Kruskal-Wallis test is used to compare data among 3 or more independent groups. Multivariate logistic regression analysis was performed for identification of factors related to the presence of outer foveolar defect. The presence of outer foveolar defect after surgery was the dependent variable, and the independent variables included gender, age, baseline visual acuity, type of intraocular tamponade, MH diameter, hole base diameter, MH height, MH index, diameter hole index, the period for obtaining initial OCT scan after surgery, and lens status. The results were considered significant at P values of less than .05. The disappearance time of the phenomenon was evaluated by Kaplan-Meier survival analysis.
Results
All 110 eyes were subjected to surgery for MH during the study period. Among the 110 eyes, 3 eyes were excluded because of the short follow-up period of less than 3 months and 2 eyes were excluded because of nonperformance of postoperative OCT. Nine cases undergoing further treatment for unsealed MH were also excluded. Thus, 96 eyes of 93 subjects were ultimately included in this study. None of the patients in our series experienced recurrence after MH closure was achieved. The mean (± SD) age of the patients was 61.9 ± 12.0 years (range, 22 to 79 years). The study group included 33 men and 60 women. The mean follow-up period was 14.4 ± 9.0 months (range, 3 to 32 months). The postoperative OCT classification of MH sealing revealed a U-shaped closure in 69 eyes (71.8%), a V-shaped closure in 26 eyes (27.0%), and a flat-open closure in 1 eye (1%).
Outer foveolar defects were identified on the initial OCT after surgery for MH in 44 of the 96 eyes (45.8%). Eyes were categorized into the with-defect group (44 eyes, 41 subjects) and the without-defect group (52 eyes, 52 subjects). The baseline characteristics and a comparison of the 2 groups are provided in Table 1 . Demographic data regarding age, gender, laterality, preoperative lens status, lens status at the last visit, frequency of cataract surgery during follow-up, and follow-up period revealed no significant differences between the 2 groups.
| Variable | With-Defect Group (44 Eyes of 41 Patients) | Without-Defect Group (52 Eyes of 52 Patients) | P Value |
|---|---|---|---|
| Follow-up period, months (mean ± SD) | 14.0 ± 6.0 | 14.3 ± 9.5 | .687 a |
| Gender, female:male | 27:14 | 30:22 | .521 b |
| Age, years (mean ± SD) | 60.4 ± 10.2 | 62.3 ± 11.9 | .562 a |
| Intraocular tamponade, air: SF 6 : C 3 F 8 :silicone oil | 4:17:23:0 | 0:8:45:1 | .005 c |
| Period obtaining initial OCT scan after surgery, days (mean ± SD) | 8.3 ± 3.6 | 19.5 ± 13.9 | .020 d |
| VA at baseline (logMAR; mean ± SD) | 0.76 ± 0.32 | 0.88 ± 0.24 | .044 a |
| VA at last follow-up (logMAR; mean ± SD) | 0.36 ± 0.32 | 0.60 ± 0.34 | <.0001 a |
| MH diameter at baseline, μm (mean ± SD) | 333.5 ± 126.3 | 504.2 ± 155.6 | <.0001 d |
| Hole base diameter at baseline, μm (mean ± SD) | 611.0 ± 240.7 | 887.2 ± 342.6 | <.0001 d |
| MH height at baseline, μm (mean ± SD) | 367.0 ± 75.7 | 390.2 ± 91.9 | .178 a |
| MH index (height/base diameter) (mean ± SD) | 0.66 ± 0.24 | 0.51 ± 0.21 | .000 a |
| Diameter hole index (MH diameter/base diameter) (mean ± SD) | 0.61 ± 0.17 | 0.60 ± 0.23 | .157 a |
| MH closure type, U-type:V-type:flat-open | 36:8:0 | 33:18:1 | .159 c |
| Lens status | |||
| Preoperative, pseudophakia:phakia | 1:43 | 4:48 | .320 c |
| At last follow-up, pseudophakia:phakia | 38:6 | 40:12 | .272 c |
| Combined cataract surgery:cataract surgery during follow-up | 6:31 | 8:28 | .718 c |
The mean preoperative MH diameter in the with-defect group was 333.5 ± 126.3 μm (range, 110 to 568 μm), smaller than that of the without-defect group, which was 504.2 ± 155.6 μm (range, 240 to 848 μm) ( P < .0001). The eyes in the with-defect group exhibited smaller preoperative hole base diameter ( P = .0003, t test), more frequent utilization of short-acting gas ( P < .0001, Fisher exact test), and a shorter period between surgery and initial postoperative OCT ( P = .020, t test). Additionally, no differences in the central foveolar thickness between the 2 groups at the last visit were noted (150.7 ± 63.0 μm vs 147.0 ± 36.5 μm; P = .438). The distributions of the OCT types of MH sealing did not differ between the 2 groups; U-type, V-type closure, and flat-open sealing types were identified in 36, 8, and 0 eyes, respectively, in the with-defect group and 33, 18, and 1 eyes, respectively, in the without-defect group ( P = .159). Using multivariate logistic regression analysis, we sought to identify possible factors that might have influenced the presence of the outer foveolar defect. MH diameter and baseline visual acuity were related to the presence of outer foveolar defect ( P = .013, P = .015, respectively).
The size of the outer foveolar defect gradually diminished over the follow-up period. Additionally, the complete disappearance of outer foveolar defects was noted in 37 eyes during the 4 weeks to 18 months after surgery. In the remaining 7 eyes, the outer foveolar defect persisted until patients were transferred to local clinics. For those 7 eyes, the mean follow-up period after surgery in our hospital was 3.0 ± 0.8 months. Including all the eyes evidencing outer foveolar defects on postoperative OCT, we determined the mean disappearance time of the defect via statistics utilizing Kaplan-Meier survival analysis. The mean disappearance time was estimated as 182 days. The mean height of the outer foveolar defect upon initial identification was 72.8 ± 25.0 μm. Additionally, the central foveolar thickness including the outer foveolar defect at that time was 175.8 ± 45.2 μm. After the disappearance of outer foveloar defects, the mean central foveolar thickness was reduced to 148.8 ± 35.6 μm ( P = .002). Resolution time of the outer foveolar defect was not correlated with final visual acuity ( P = .248, r = .039).
Preoperative logMAR BCVA ranged between 0.2 and 1.3. The mean preoperative logMAR BCVA was better in the with-defect group than in the without-defect group (0.76 ± 0.32 vs 0.88 ± 0.24; P = .044). Postoperative BCVA at the final visit ranged between 0 and 0.7. The mean postoperative BCVA was better in the with-defect group than in the without-defect group (0.36 ± 0.32 vs 0.60 ± 0.34; P < .0001). The mean logMAR BCVA of 37 eyes, in all of which the complete disappearance of the outer foveolar defect was confirmed, was 0.58 ± 0.23 at the time of initial detection of the defect. The mean BCVA in those eyes at the time of complete disappearance of the defect improved significantly, to 0.40 ± 0.26 ( P < .0001).
We determined that BCVA after surgery for idiopathic MH generally continued to improve gradually over the follow-up period. In order to assess the effects of the outer foveolar defect on postoperative visual outcomes, we compared changes in visual acuity during the 12-month follow-up between the 45 eyes in the without-defect group and the 35 eyes in the with-defect group. BCVA was better in the with-defect group than in the without-defect group, both prior to and after surgery. Because MH diameter was positively correlated with baseline visual acuity ( P = .002, r = 0.304), we eliminated the confounding effect of MH diameter using the Spearman partial correlation analysis. After adjusting for macular hole diameter, we detected no significant differences in BCVA between the 2 groups. A comparison of changes in visual acuity between the 2 groups is provided in Table 2 .



