Purpose
To describe the incidence and outcomes of reoperations for glaucoma in the Tube Versus Trabeculectomy (TVT) Study.
Design
Cohort study of patients in a multicenter randomized clinical trial.
Methods
The TVT Study enrolled 212 patients with medically uncontrolled glaucoma who had previous cataract and/or glaucoma surgery. Randomization assigned 107 patients to surgery with a tube shunt (350 mm 2 Baerveldt glaucoma implant) and 105 patients to trabeculectomy with mitomycin C (0.4 mg/mL for 4 minutes). Data were analyzed from patients who failed their assigned treatment and had additional glaucoma surgery. Outcome measures included intraocular pressure (IOP), use of glaucoma medications, visual acuity, surgical complications, and failure (IOP >21 mm Hg or not reduced by 20%, IOP ≤5 mm Hg, additional glaucoma surgery, or loss of light perception vision).
Results
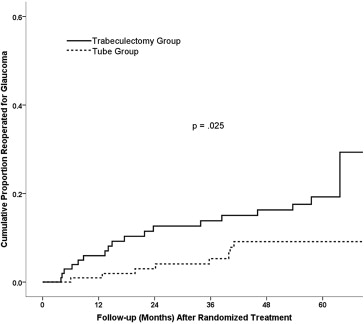
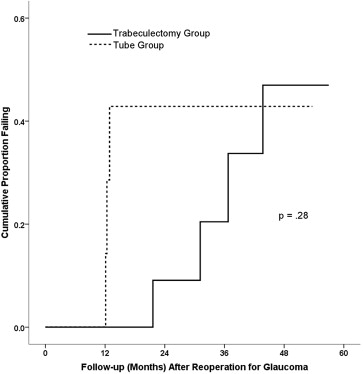
Additional glaucoma surgery was performed in 8 patients in the tube group and 18 patients in the trabeculectomy group in the TVT Study, and the 5-year cumulative reoperation rate was 9% in the tube group and 29% in the trabeculectomy group ( P = .025). Follow-up (mean ± SD) after additional glaucoma surgery was 28.0 ± 16.0 months in the tube group and 30.5 ± 20.4 months in the trabeculectomy group ( P = .76). At 2 years after a glaucoma reoperation, IOP (mean ± SD) was 15.0 ± 5.5 mm Hg in the tube group and 14.4 ± 6.6 mm Hg in the trabeculectomy group ( P = .84). The number of glaucoma medications (mean ± SD) after 2 years of follow-up was 1.1 ± 1.3 in the tube group and 1.4 ± 1.4 in the trabeculectomy group ( P = .71). The cumulative probability of failure at 1, 2, 3, and 4 years after additional glaucoma surgery was 0%, 43%, 43%, and 43%, respectively, in the tube group, and 0%, 9%, 20%, and 47% in the trabeculectomy group ( P = .28). Reoperations to manage complications were required in 1 patient in the tube group and 5 patients in the trabeculectomy group ( P = .63).
Conclusions
The rate of reoperation for glaucoma was higher following trabeculectomy with mitomycin C than tube shunt surgery in the TVT Study. Similar surgical outcomes were observed after additional glaucoma surgery, irrespective of initial randomized treatment in the study.
The Tube Versus Trabeculectomy (TVT) Study is a multicenter randomized clinical trial comparing the safety and efficacy of tube shunt surgery and trabeculectomy with mitomycin C (MMC) in eyes with previous ocular surgery. The study found similar intraocular pressure (IOP) and use of glaucoma medical therapy with both surgical procedures after 5 years of follow-up. Trabeculectomy with MMC had higher rates of surgical failure and reoperation for glaucoma compared with tube shunt surgery. No difference in the rate of vision loss was observed following the 2 procedures. Early postoperative complications were more frequent after trabeculectomy with MMC relative to tube shunt placement, but both procedures had similar rates of late postoperative complications and serious complications after 5 years.
In previous publications of TVT Study data, patients were censored from analysis of IOP, use of glaucoma medications, and complications after a glaucoma reoperation was performed. Therefore, the outcomes of patients who had additional glaucoma surgery in the study have not been previously described. The purpose of this study is to report the incidence and outcomes of reoperations for glaucoma in the TVT Study.
Methods
The design and methods of the TVT Study have been previously described in detail. The present investigation is a cohort study of patients in a multicenter randomized clinical trial. The study was approved by the Institutional Review Board at each Clinical Center. Written informed consent was obtained from all subjects for both the treatment and participation in the research. The study adhered to the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA). The TVT Study is registered in http://www.clinicaltrials.gov ( NCT00306852 ).
Enrolled patients were randomly assigned to treatment with a tube shunt or trabeculectomy with MMC. Patients in the tube group underwent placement of a 350 mm 2 Baerveldt glaucoma implant in the superotemporal quadrant with a complete restriction of flow at the time of implantation. Patients in the trabeculectomy group had a superior trabeculectomy with a standard dosage of MMC of 0.4 mg/mL for 4 minutes. Follow-up visits were scheduled 1 day, 1 week, 1 month, 3 months, 6 months, 1 year, 18 months, 2 years, 3 years, 4 years, and 5 years postoperatively. Each examination included measurement of Snellen visual acuity (VA), IOP, slit-lamp biomicroscopy, Seidel testing, and ophthalmoscopy. The examining clinician provided a reason for loss of 2 or more lines of Snellen VA at follow-up visits after 3 months.
Reoperations for glaucoma or complications were defined as additional procedures that required a return to the operating room. Cyclodestruction, whether performed in the clinic or operating room setting, was also counted as a reoperation for glaucoma. Interventions done at the slit lamp, such as needling procedures, were not considered glaucoma reoperations. The decision to perform additional glaucoma surgery was left to the discretion of the investigator. Patients were censored from several analyses at the time of reoperation for glaucoma in previous publications reporting TVT Study outcomes. However, data were still collected at scheduled follow-up visits after a reoperation. The IOP and number of glaucoma medications were determined immediately prior to repeat glaucoma surgery. The criteria used to define surgical failure after initial randomized treatment (IOP >21 mm Hg or not reduced by 20% below baseline on 2 consecutive follow-up visits after 3 months, IOP ≤5 mm Hg on 2 consecutive follow-up visits after 3 months, reoperation for glaucoma, or loss of light perception vision) were applied after reoperation for glaucoma in the present study.
Patients were grouped for data analysis based on their initial randomized treatment in the TVT Study. Univariate comparisons between treatment groups were performed using the 2-sided Student t test for continuous variables and the χ 2 test or Fisher exact test for categorical variables. Snellen VA measurements were converted to logMAR equivalents for the purpose of data analysis, as reported previously. The time to failure was defined either as the time from surgical treatment to reoperation for glaucoma, or as the time from surgical treatment to the first of 2 consecutive follow-up visits after 3 months in which the patient had persistent hypotony (IOP ≤5 mm Hg) or inadequately reduced IOP (IOP >21 mm Hg or not reduced by 20%). A P value of .05 or less was considered statistically significant in our analyses.
Results
Patient Characteristics
The TVT Study enrolled 212 patients, including 107 in the tube group and 105 in the trabeculectomy group. Figure 1 presents the results from Kaplan-Meier survival analysis comparing the rates of reoperation between the 2 treatment groups in the TVT Study after initial randomization. The 5-year cumulative reoperation rate was 9% in the tube group and 29% in the trabeculectomy group ( P = .025, log-rank test adjusted for stratum). Table 1 shows the patient characteristics at the time of glaucoma reoperation in the TVT Study. No significant differences in any of the demographic or ocular features were observed between the 2 treatment groups, although there was a tendency for patients in the tube group to have a lower IOP at the time of additional glaucoma surgery.
| Tube Group (n = 8) | Trabeculectomy Group (n = 18) | P Value | |
|---|---|---|---|
| Age (y) | .87 b | ||
| Mean ± SD | 69.3 ± 12.6 | 68.4 ± 11.9 | |
| Range | 48-83 | 33-88 | |
| Sex, n (%) | .22 c | ||
| Male | 6 (75) | 8 (44) | |
| Female | 2 (25) | 10 (56) | |
| Race, n (%) | 1.00 d | ||
| White | 3 (38) | 6 (33) | |
| Black | 5 (63) | 10 (56) | |
| Hispanic | 0 | 1 (6) | |
| Other | 0 | 1 (6) | |
| Diabetes mellitus, n (%) | 2 (25) | 9 (50) | .40 c |
| Hypertension, n (%) | 4 (50) | 9 (50) | 1.00 c |
| IOP (mm Hg), | .078 b | ||
| Mean ± SD | 21.3 ± 5.6 | 27.5 ± 8.6 | |
| Range | 14-33 | 18-47 | |
| Glaucoma medications, mean ± SD | 3.3 ± 1.2 | 2.9 ± 1.1 | .46 b |
| Diagnosis, n (%) | .24 d | ||
| POAG | 8 (100) | 12 (67) | |
| CACG | 0 | 2 (11) | |
| Other | 0 | 4 (22) | |
| Lens status, n (%) | .85 d | ||
| Phakic | 1 (13) | 2 (11) | |
| PCIOL | 7 (88) | 13 (72) | |
| ACIOL | 0 | 2 (11) | |
| Aphakic | 0 | 1 (6) | |
| Stratum a | .39 d | ||
| 1 | 2 (25) | 9 (50) | |
| 2 | 4 (50) | 4 (22) | |
| 3 | 0 | 2 (11) | |
| 4 | 2 (25) | 3 (17) | |
| Previous intraocular surgery | .70 b | ||
| Mean ± SD | 2.88 ± 0.99 | 2.72 ± 0.89 | |
| Range | 2-5 | 2-5 | |
| Time interval since randomized surgical treatment (mo) | .67 b | ||
| Mean ± SD | 27.4 ± 13.7 | 24.1 ± 19.8 | |
| Range | 6-41 | 4-64 | |
| Snellen VA | .31 b | ||
| LogMAR mean ± SD | 0.94 ± 0.89 | 0.60 ± 0.58 | |
| Median | 20/100 | 20/50 | |
| Range | 20/20-CF | 20/25-CF |
a Stratum 1 = previous cataract extraction; stratum 2 = previous trabeculectomy or combined procedure without an antifibrotic agent; stratum 3 = previous trabeculectomy with 5-fluorouracil or combined procedure with 5-fluorouracil or mitomycin C; stratum 4 = previous trabeculectomy with mitomycin C.
Types of Glaucoma Reoperations
Table 2 shows the reoperations that were performed for glaucoma in the TVT Study after 5 years of follow-up. A total of 18 patients in the trabeculectomy group underwent additional glaucoma surgery, which involved placement of a tube shunt in 15 patients, a bleb revision with tube shunt placement in 2 patients, and a trabeculectomy with 5-fluorouracil in 1 patient. One of these patients underwent a trans-scleral cyclophotocoagulation 31 months after tube shunt placement as a second reoperation for glaucoma in the study eye. In the tube group, 8 patients had glaucoma reoperations, including placement of a second tube shunt in 4 patients, trans-scleral cyclophotocoagulation in 3 patients, and endocyclophotocoagulation performed in conjunction with cataract surgery in 1 patient. Trans-scleral cyclophotocoagulation was performed as a second reoperation for glaucoma 13 months after combined cataract extraction and endocyclophotocoagulation in 1 patient, and 12 months after trans-scleral cyclophotocoagulation in another patient.
| Tube Group (n = 107) | Trabeculectomy Group (n = 105) | |
|---|---|---|
| Tube shunt | 4 | 15 |
| Trans-scleral cyclophotocoagulation | 3 | 0 |
| Endocyclophotocoagulation/cataract extraction | 1 | 0 |
| Bleb revision and tube shunt | 0 | 2 |
| Trabeculectomy with 5-FU | 0 | 1 |
| Total number of patients (cumulative percentage) with reoperation for glaucoma a | 8 b (9) | 18 c (29) |
a P = .025 for the difference in 5-year cumulative reoperation rates for glaucoma between treatment groups from Kaplan-Meier analysis (log-rank test adjusted for stratum).
b Two patients underwent trans-scleral cyclophotocoagulation as a second reoperation for glaucoma.
c One patient underwent trans scleral cyclophotocoagulation as a second reoperation for glaucoma.
Risk Factor Analysis for Glaucoma Reoperation
Baseline demographic and clinical characteristics of the overall TVT Study population were evaluated as possible predictors for reoperation for glaucoma after 5 years of follow-up, and the results are provided in Table 3 . Reoperations were pooled from both treatment groups for this risk factor analysis. Only assigned treatment was significantly associated with reoperation for glaucoma in univariate analysis ( P = .025, log-rank test). Stratum, age, sex, ethnicity, diabetes mellitus, hypertension, lens status, number of previous intraocular surgeries, glaucoma type, preoperative number of medications, preoperative IOP, preoperative Snellen VA, and clinical centers were not associated with additional glaucoma surgery either univariately or in a multivariate model adjusted for treatment.
| Risk Factor | Number (%) | Cumulative Probability of Reoperation for Glaucoma (%) b | P Value | |
|---|---|---|---|---|
| Univariate c | Multivariate d | |||
| Stratum a | .45 | .54 | ||
| 1 | 94 (44) | 14.1 | ||
| 2 | 49 (23) | 30.3 | ||
| 3 | 35 (17) | 7.6 | ||
| 4 | 34 (16) | 17.6 | ||
| Age (y) | .11 | .12 | ||
| <60 years | 31 (15) | 16.4 | ||
| 60-69 | 59 (28) | 47.4 | ||
| 70-79 | 79 (37) | 12.0 | ||
| ≥80 | 43 (20) | 6.2 | ||
| Sex | .40 | .43 | ||
| Male | 100 (47) | 16.5 | ||
| Female | 112 (53) | 20.7 | ||
| Race | .11 | .12 | ||
| White | 95 (45) | 10.7 | ||
| Black | 82 (39) | 31.6 | ||
| Hispanic | 30 (14) | 3.8 | ||
| Other | 5 (2) | 50.0 | ||
| Diabetes mellitus | .18 | .18 | ||
| Yes | 67 (32) | 20.5 | ||
| No | 145 (68) | 17.2 | ||
| Hypertension | .36 | .22 | ||
| Yes | 124 (59) | 19.9 | ||
| No | 88 (42) | 17.0 | ||
| Lens status | .34 | .35 | ||
| Phakic | 45 (21) | 14.5 | ||
| PCIOL | 160 (76) | 18.3 | ||
| ACIOL | 7 (3) | 31.4 | ||
| Previous intraocular surgery | .27 | .13 | ||
| 1 | 163 (77) | 18.3 | ||
| 2 | 41 (19) | 19.9 | ||
| 3 or 4 | 8 (4) | 27.1 | ||
| Time since last intraocular surgery (mo) | .76 | .89 | ||
| <6 months | 15 (7) | 14.4 | ||
| ≥6 months | 190 (93) | 18.6 | ||
| Glaucoma type | .31 | .14 | ||
| Primary | 190 (90) | 18.3 | ||
| Secondary | 22 (10) | 18.2 | ||
| Preoperative number of glaucoma medications | .86 | .58 | ||
| 0-1 | 21 (10) | 10.0 | ||
| 2-3 | 108 (51) | 21.1 | ||
| 4-6 | 83 (39) | 15.2 | ||
| Preoperative IOP (mm Hg) | .61 | .67 | ||
| <23 | 77 (36) | 21.7 | ||
| 23-26 | 66 (31) | 18.7 | ||
| >26 | 69 (33) | 13.9 | ||
| Preoperative Snellen VA | .27 | .58 | ||
| ≥20/30 | 106 (50) | 12.1 | ||
| 20/40-20/150 | 74 (35) | 20.0 | ||
| ≤20/200 | 32 (15) | 38.9 | ||
| Clinical centers | .38 | .40 | ||
| Enrolled ≥50% patients | 133 (63) | 19.0 | ||
| Enrolled <50% patients | 79 (37) | 15.9 | ||
| Treatment | .025 | – | ||
| Tube | 107 (50) | 9.1 | ||
| Trabeculectomy | 105 (50) | 29.3 | ||
a Stratum 1 = previous cataract extraction; stratum 2 = previous trabeculectomy or combined procedure without an antifibrotic agent; stratum 3 = previous trabeculectomy with 5-fluorouracil or combined procedure with 5-fluorouracil or mitomycin C; stratum 4 = previous trabeculectomy with mitomycin C.
b Kaplan-Meier survival analysis.
d Cox proportional hazard regression analysis, P value adjusted for treatment.
Evaluation for Reoperation Bias
Because the surgeon was not masked to the treatment assignment, a potential bias existed in the decision to reoperate for glaucoma. To evaluate for selection bias, the IOP levels were compared between the tube and trabeculectomy groups in patients who had inadequate IOP control after randomized treatment. The IOP (mean ± SD) was 21.1 ± 5.7 mm Hg for the 8 patients in the tube group and 27.0 ± 9.0 mm Hg for the 18 patients in the trabeculectomy group at the time of reoperation for glaucoma ( P = .11, Student t test). The IOP levels were also compared between the 12 patients in the tube group and 11 patients in the trabeculectomy group who failed because of inadequate IOP reduction (ie, IOP >21 mm Hg or not reduced by 20% from baseline) but did not undergo additional glaucoma surgery during 5 years of follow-up. In this patient subgroup, the IOP (mean ± SD) was 23.0 ± 5.1 mm Hg in the tube group and 20.1 ± 2.6 in the trabeculectomy group ( P = .11, Student t test). The mean IOP prior to reoperation for glaucoma was similar in the tube and trabeculectomy groups, and no significant difference was seen between treatment groups in mean IOP among patients who failed because of inadequate IOP reduction but did not undergo additional glaucoma surgery.
IOP and Glaucoma Medical Therapy
Table 4 provides data on IOP and use of glaucoma medical therapy after a glaucoma reoperation in the tube and trabeculectomy groups. No significant differences in mean IOP and use of medical therapy were seen between the 2 treatment groups at any time point.
| Tube Group | Trabeculectomy Group | P Value b | |
|---|---|---|---|
| Preoperative | |||
| IOP (mm Hg) | 21.3 ± 5.6 | 27.5 ± 8.6 | .078 |
| Glaucoma medications | 3.3 ± 1.2 | 2.9 ± 1.1 | .46 |
| N | 8 | 17 a | |
| 6 months | |||
| IOP (mm Hg) | 12.2 ± 5.6 | 17.4 ± 8.1 | .35 |
| Glaucoma medications | 0 (0) | .3 ± .8 | .52 |
| N | 3 | 6 | |
| 1 year | |||
| IOP (mm Hg) | 11.6 ± 3.9 | 15.5 ± 5.6 | .15 |
| Glaucoma medications | 1.8 ± 1.3 | 1.1 ± 1.4 | .29 |
| N | 6 | 13 | |
| 2 years | |||
| IOP (mm Hg) | 15.0 ± 5.5 | 14.4 ± 6.6 | .84 |
| Glaucoma medications | 1.1 ± 1.3 | 1.4 ± 1.4 | .71 |
| N | 7 | 10 | |
| 3 years | |||
| IOP (mm Hg) | 8.2 ± 3.2 | 14.1 ± 6.3 | .16 |
| Glaucoma medications | 1.7 ± 1.5 | 1.2 ± 1.0 | .56 |
| N | 3 | 9 | |
| 4 years | |||
| IOP (mm Hg) | 7.8 ± 4.6 | 16.4 ± 4.1 | .078 |
| Glaucoma medications | 1.0 ± 1.4 | 1.8 ± 1.7 | .63 |
| N | 2 | 4 | |
| 5 years | |||
| IOP (mm Hg) | – | 19.6 ± 1.1 | – |
| Glaucoma medications | – | .5 ± 1.0 | – |
| N | – | 4 | |
| Last follow-up | |||
| IOP (mm Hg) | 13.4 ± 6.6 | 16.4 ± 7.0 | .35 |
| Glaucoma medications | 1.7 ± 1.4 | .9 ± 1.3 | .21 |
| N | 7 | 16 |
a IOP was not available immediately prior to reoperation in 1 patient.
Surgical Success
Kaplan-Meier survival analysis was used to compare failure rates in patients who had glaucoma reoperations, and the results are shown in Figure 2 . The cumulative probability of failure at 1, 2, 3, and 4 years after additional glaucoma surgery was 0%, 43%, 43%, and 43%, respectively, in the tube group and 0%, 9%, 20%, and 47% in the trabeculectomy group ( P = .28, log-rank test). Earlier failure was observed in the tube group compared with the trabeculectomy group, although this difference was not statistically significant. Treatment failure occurred in 3 patients in the tube group, including 1 patient who had inadequate IOP reduction and 2 patients who underwent a cyclophotocoagulation as a second reoperation for glaucoma. There were 4 patients who failed in the trabeculectomy group, including 2 patients who had inadequate IOP reduction, 1 patient who had a cyclophotocoagulation as another glaucoma reoperation, and 1 patient who developed persistent hypotony.
Complications
Table 5 lists postoperative complications that developed after reoperation for glaucoma. A total of 5 complications were reported in 2 patients the tube group, and 15 complications were reported in 8 patients in the trabeculectomy group ( P = .42, Fisher exact test). Among patients who had additional glaucoma surgery, reoperations were required to manage complications in 1 patient in the tube group and 5 patients in the trabeculectomy group ( P = .63, Fisher exact test). A penetrating keratoplasty was performed in 1 patient in the tube group for persistent corneal edema, and this patient subsequently underwent removal of the intraocular lens, anterior vitrectomy, and tube repositioning for tube-cornea touch. There were 3 patients in the trabeculectomy group who had a penetrating keratoplasty for persistent corneal edema, and 1 of these patients subsequently underwent a repeat penetrating keratoplasty. A pars plana vitrectomy with injection of intravitreal antibiotics was performed in 1 patient in the trabeculectomy group for endophthalmitis. Another patient in the trabeculectomy group had a pars plana vitrectomy and scleral buckling procedure for a retinal detachment, and the tube shunt was later removed and a new shunt placed in a different quadrant for a tube erosion.



