Purpose
To evaluate the outcomes of a new technique for deep anterior lamellar keratoplasty (DALK) employing the injection of air up to 2 mm inside a deep trephination (intended within 100 μm from the endothelial surface) obtained with a guarded trephine set by means of anterior segment optical coherence tomography (AS OCT).
Design
Retrospective, noncomparative, interventional case series.
Methods
The success rate and learning curve of pneumatic dissection in one clinical practice were analyzed in nonscarred keratoconic eyes undergoing a standardized DALK including 9-mm trephination intended to a depth within 100 μm from the endothelial surface, based on the thinnest AS OCT measurement at this site; and injection of air through a cannula advanced 1–2 mm centripetally from the bottom of the trephination. Surgical parameters, success rate of pneumatic dissection, and complications were recorded.
Results
Eighty-eight eyes of 88 patients were included in the study. Pneumatic dissection succeeded in 75 of 88 eyes (85%). No significant correlation could be found between number of cases performed and success rate for this surgeon. Complications included loss of suction during trephination (n = 2, 2.3%) and perforation (n = 4, 4.6%). Conversion to penetrating keratoplasty was necessary in 1 case (1.1%).
Conclusion
Setting an adjustable trephine to a depth within 100 μm from the endothelial surface eliminates the need for reaching the central cornea for successful pneumatic dissection and substantially flattens the learning curve of DALK, while achieving a constant success rate above 80% and minimizing complications.
Since its introduction in 2002, pneumatic dissection leading to the formation of the so-called “big bubble” has emerged as the most popular surgical technique employed for deep anterior lamellar keratoplasty (DALK). However, as shown by the 2014 annual report of the American Eye Bank Association, to date this procedure is performed only in a small percentage of those eyes for which it is indicated. Until now, most techniques have involved a trephination within the anterior two thirds of the stroma; the centripetal advancement of a needle/cannula into the center of the cornea, trying to reach the deep stroma; and finally the injection of air. Surgeons have done so under the assumption that, in order to maximize the success rate of pneumatic dissection, before injecting air the needle/cannula should reach the central cornea as close as possible to the posterior corneal surface. Recently, it has been confirmed that the rate of big bubble formation exceeds 90% when the needle/cannula reaches a depth within 100 μm from the internal corneal surface.
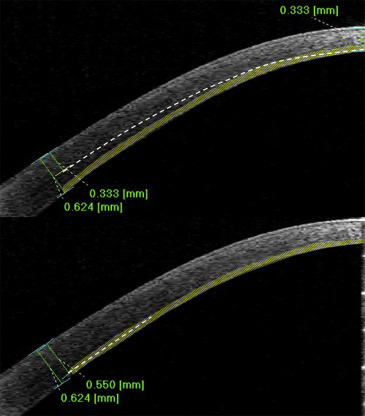
The challenge with this approach is to reach the central cornea at the proper depth with a safe and reproducible technique. Even the use of pachymetric values as reference to guide the surgical procedure has not added substantial advantages. As shown in Figure 1 (Top), setting the trephine/blade to target the thinnest central measurement still obliges the surgeons to advance the needle/cannula from a relatively superficial peripheral level all the way into the thinner central cornea, still following the surgeon’s intraoperative judgment.
To truly standardize DALK, we combined anterior segment optical coherence tomography (AS OCT) technology with the use of a trephine with predeterminable and measurable blade advancement for the development of a new surgical approach. The technique is based on the assumption that it is also possible to achieve a big bubble by injection of air into the deep stroma in the peripheral cornea. If this is proven true, there would be no need for the cannula/needle to reach the center of the cornea, thus eliminating the subjectively guided part of the procedure. The technique consists of 3 main steps: exact measurement of corneal thickness at the site of trephination; calibration of the trephine to stop the blade advancement within 100 μm from the thinnest pachymetric value obtained at the site of trephination; and injection of air after minimal (1–2 mm) centripetal introduction of a dedicated cannula into the stroma. We report herein the success rate of pneumatic dissection using this technique, the complication rate, and the learning curve observed for 1 surgeon with this technique in a series of consecutive nonscarred keratoconic eyes.
Methods
We reviewed the charts of all patients with nonscarred keratoconus who had undergone pneumatic dissection for DALK from the initial use of this procedure from September 1, 2013 to July 31, 2015. Eyes with scarred keratoconus were excluded in an attempt at eliminating factors possibly affecting the success of pneumatic dissection, as well as optimizing the homogeneity of the study population. All eyes had been operated on by the same surgeon (M.B.) at Villa Igea Hospital in Forlì (Italy). The study followed the tenets of the 1964 Declaration of Helsinki and was approved by the local ethics committee (Comitato Etico Ospedali Privati Forlì); a detailed informed consent had been provided by all patients.
Data collected included preoperative corneal thickness measured by AS OCT (Casia; Tomey, Tokyo, Japan) over the entire cornea, surgical parameters (depth of trephination, cannula advancement, amount of air injected), success or failure of pneumatic dissection, and all complications.
Data were analyzed with the Minitab, version 16 (Minitab Inc, State College, Pennslyvania, USA). Pearson correlation was used to analyze the relationship between the number of surgeries performed and the overall success rate. A P value of <.05 was considered statistically significant.
Surgical Procedure
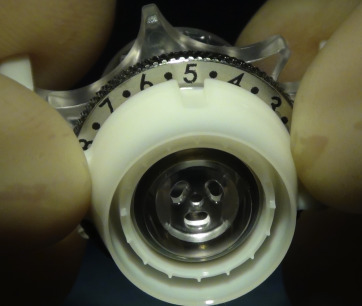
In all patients anesthesia and akinesia were obtained with a peribulbar injection of 8–10 cc of ropivacaine (0.75% solution). To reach the intended depth, a suction trephine (Moria, Antony, France) with a predeterminable block of the measurable blade advancement ( Figure 2 ) was centered on the geometric center of the cornea. The measurable blade advancement can be regulated precisely only in 50-μm steps, so the trephine was set to a depth between 0 and 50 μm from the thinnest AS OCT measurement at the site of trephination (9 mm in diameter).
A temporal paracentesis was performed to soften the eye and a small air bubble was injected into the anterior chamber. Then, a blunt Fogla probe (Bausch & Lomb Storz Ophthalmics, Irvine, USA) was inserted at the base of the trephination ( Figure 3 , Top left) and advanced up to 1 mm into the stroma, tangentially to the corneal posterior surface, with the purpose of maintaining the depth reached with the trephination ( Figure 3 , Top right).
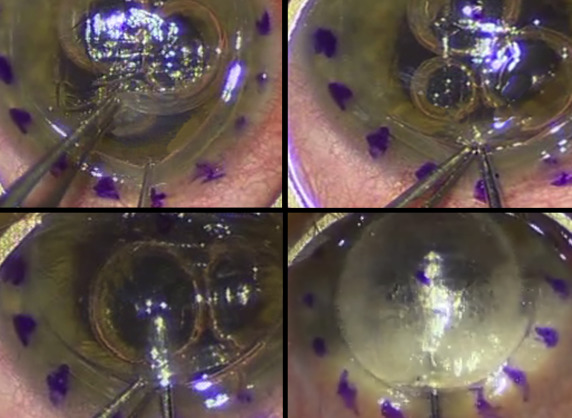
The probe was then exchanged for a 27 gauge Fogla cannula (Bausch & Lomb Storz Ophthalmics), which was slowly advanced, following the track obtained with the probe, up to 1 additional millimeter into the cornea ( Figure 3 , Bottom left) and air was gently and progressively forced into the stroma until a bubble was obtained ( Figure 3 , Bottom right).
DALK was then completed in all eyes according to a technique presented as a video in 2013 at the Annual Meeting of the American Academy of Ophthalmology, including baring the bubble floor only in the central 6 mm of the cornea and transplanting an anterior lamella cut by microkeratome-assisted dissection. When pneumatic dissection failed, including in the 2 cases of incomplete trephination due to loss of suction, the procedure was completed in the same way, but baring of the central 6 mm was obtained by manual dissection.
When trephination (n = 2) or cannula advancement (n = 1) caused a perforation, pneumatic dissection was attempted at a site about 3 mm away from the perforation, succeeding in creating a big bubble and allowing uneventful completion of the procedure. In the remaining case, after a macroperforation occurred during hand dissection, the procedure was converted into a 2-piece mushroom keratoplasty according to the technique described in the past.
Results
Eighty-eight eyes of 88 patients were identified. The mean age at the time of surgery was 32.3 ± 10.4 years. There were 50 male and 38 female patients.
The average peripheral corneal thickness was 602.3 ± 46.7 μm. The intended depth of trephination (setting of the trephine block) was 500 μm in 52 eyes and 550 μm in 36 eyes (ie, 520.4 ± 24.7 μm on average). The total advancement of the cannula centripetally never exceeded 2 mm. The amount of air injected varied between 1 and 5 cc.
Intraoperative complications occurred in 6 eyes (6.8%) and included loss of suction during trephination in 2 eyes (2.3%); perforation during trephination in 2 eyes (2.3%); perforation during cannula advancement in 1 eye (1.1%); and perforation during hand dissection after failed pneumatic dissection in 1 eye (1.1%). Two of these cases could be continued as planned with successful bubble formation; in the 4 remaining cases the procedure was completed by hand dissection (n = 3, 3.4%) or converted into a mushroom keratoplasty (n = 1, 1.1%).
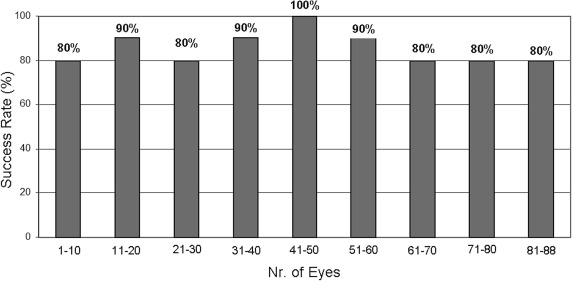
The overall success rate of pneumatic dissection was 85.2% (75 of 88 eyes). In all cases of successful pneumatic dissection, the bubble obtained was clinically classified as type 1, according to Dua and associates’ description. If eyes with complications related to trephination (n = 4) are excluded, pneumatic dissection was achieved in 88.0% (74 of 84 eyes). As shown in Figure 4 , the success rate for the initial 10 cases was 80% and did not differ substantially in the following cases. An insignificant and inverse correlation was found between the number of cases and the overall success rate (r = −0.67, P = .22).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


