Purpose
To describe outcomes after Boston Type 1 Keratoprosthesis (KPro) surgery in aniridic eyes.
Design
Retrospective, interventional case series.
Methods
setting : University-based tertiary care institution. patient population : Twenty-six aniridic eyes of 19 patients who underwent KPro implantation by a single experienced surgeon (M.H.-D.) between October 27, 2008 and January 16, 2012. main outcome measures : Preoperative and postoperative best-corrected visual acuity (BCVA), intraoperative and postoperative complications, and keratoprosthesis retention.
Results
Mean age was 56 years (range, 28–72); 10 patients were male. Seven patients had bilateral procedures. No intraoperative complications were encountered. Preoperatively, BCVA was 20/300 or worse in all eyes. After a mean follow-up time of 28.7 ± 13.5 months (range 4–50), the most recent BCVA was 20/200 or better in 14 eyes. Visual potential was limited by preexisting terminal glaucoma (n = 2), phthisis after retinal detachment (n = 4), and suprachoroidal hemorrhage (n = 2). Other postoperative complications included retroprosthetic membrane formation (n = 15), infectious keratitis (n = 1), extrusion (n = 2), and corneal melt (n = 4). Uncomplicated vitritis was reported in 6 eyes. No endophthalmitis occurred in this series. Most eyes have glaucoma and are on medical treatment. The overall retention rate of the initial prosthesis was 77%.
Conclusions
The prognosis in aniridic patients after KPro is variable. Meticulous follow-up and a subspecialty team approach are of utmost importance.
Congenital aniridia, resulting from mutations of the PAX6 gene, is a complex panocular disorder associated with multiple vision-impairing manifestations, including glaucoma, cataract formation, optic nerve hypoplasia, foveal hypoplasia, and corneal opacification. Aniridic keratopathy, characterized by limbal stem cell deficiency, presents as a progressive vascular pannus, corneal conjunctivalization, recurrent epithelial erosions, and subepithelial fibrosis, which eventually lead to an opaque cornea.
Medical management is initially instituted, but these patients eventually require surgical intervention. Penetrating keratoplasty is unsuccessful in the long term in the setting of significant limbal stem cell deficiency. A keratolimbal allograft technique, with or without subsequent keratoplasty, can be a viable alternative; however, systemic immunosuppression is necessary.
In recent years, the Boston Keratoprosthesis (KPro; Massachusetts Eye and Ear Infirmary, Boston, Massachusetts, USA) has been increasingly used to treat debilitating conditions that carry a poor prognosis with traditional corneal transplantation. The KPro can be performed as either a primary or secondary procedure. In this study, we evaluate outcomes of the Boston Type 1 KPro implantation in a subset of aniridic patients with significant keratopathy.
Patients and Methods
This retrospective interventional case series included a subgroup of 26 eyes (19 patients) with congenital aniridia, in whom penetrating keratoplasty was deemed highly unlikely to succeed. The institutional review board of Notre-Dame – Centre Hospitalier de l’Université de Montréal prospectively approved the study protocol. Written informed consent was obtained from each patient before surgery.
A single experienced cornea surgeon (M.H.-D.) implanted the new threadless KPro Type 1 in all studied eyes between October 27, 2008 and January 16, 2012 in our university-based tertiary care center, Notre-Dame Hospital – Centre Hospitalier de l’Université de Montréal. Details pertaining to the prosthetic device and surgical technique have been described previously. At the end of each surgery, a soft contact lens (Kontur Contact Lens Co, Hercules, California, USA) was applied. Postoperatively, patients were maintained on a topical regimen of prednisolone acetate 1% (Sandoz Canada Inc, Boucherville, Quebec, Canada) and moxifloxacin (Vigamox; Alcon Canada Inc, Mississauga, Ontario, Canada), each administered 4 times daily. No immunosuppression or oral steroids were administered.
Follow-up visits occurred on the first postoperative day, weekly for 4 weeks, and every 3 months thereafter. Visual acuity, detailed slit-lamp examination, digital intraocular pressure estimation, funduscopy, and postoperative complications were recorded at these intervals. When necessary, bandage contact lenses were adjusted, cleaned, and replaced.
After a chart review, the data were compiled in Microsoft Excel spreadsheets (Microsoft Inc, Redmond, Washington, USA). Outcome measures included preoperative and postoperative visual acuity, prosthesis retention rate, and significant complications. The Fisher exact test was used to compare the difference in outcomes and complications between primary and secondary keratoprosthesis groups. For each comparison, a 2-sided P value <.05 was considered statistically significant.
Results
Patient Demographics and Preoperative Variables
Twenty-six eyes (14 OD, 12 OS) of 19 aniridic patients were included in this single-center study. Ten patients (53%) were male and 9 (47%) were female. Seven patients underwent bilateral KPro implantation. In this series, the mean age of patients was 56 years (standard deviation [SD] 11 years; range 28–72 years). The mean follow-up time was 28.7 months (SD 13.5 months; range 4–50 months).
Seven eyes (27%) had previously undergone failed penetrating and lamellar keratoplasties and a keratolimbal allograft. Other prior anterior segment procedures included cataract extraction (15 eyes, 58%), and superficial keratectomy (2 eyes, 8%). Comorbid preoperative conditions included nystagmus, optic nerve hypoplasia, and foveal hypoplasia. Twenty-one eyes (81%) had a prior history of glaucoma, with 5/26 eyes (19%) having undergone glaucoma surgery before KPro implantation ( Table 1 ).
| Patient Number | Eye | Age | Sex | Prior Ocular Surgeries | Preoperative BCVA | Fellow Eye BCVA |
|---|---|---|---|---|---|---|
| 1 | OS | 72 | F | PK ×1, CE | HM | CF |
| OD | CE | CF | 20/400 | |||
| 2 | OD | 67 | M | PK ×1, CE + IOL (PC) | HM | CF |
| 3 | OS | 49 | M | CE | 20/300 | 20/200 |
| 4 | OS | 70 | M | PK ×1, CE, trab ×1 | 20/400 | 20/100 |
| 5 | OS | 39 | F | Lamellar graft ×1 | CF | 20/400 |
| OD | None | CF | 20/150 | |||
| 6 | OD | 54 | M | CE, trab ×1 | 20/300 | 20/150 |
| OS | None | 20/400 | 20/100 | |||
| 7 | OS | 72 | M | PK ×2, CE, trab ×1 | HM | CF |
| OD | PK ×1, CE | CF | 20/400 | |||
| 8 | OD | 54 | M | PK ×1, LSCT ×1, CE + IOL (PC) | CF | HM |
| 9 | OD | 55 | F | CE, TS ×1, trab ×1 | CF | CF |
| 10 | OS | 47 | M | Keratectomy ×1 | CF | HM |
| OD | None | HM | 20/70 | |||
| 11 | OD | 54 | F | None | CF | CF |
| OS | None | CF | 20/300 | |||
| 12 | OS | 53 | F | CE + IOL (PC) | CF | CF |
| OD | CE + IOL (PC) | CF | 20/200 | |||
| 13 | OD | 65 | M | Keratectomy ×2 | LP | LP |
| 14 | OD | 54 | F | None | CF | 20/300 |
| 15 | OS | 28 | F | None | CF | CF |
| 16 | OS | 57 | F | CE | CF | 20/300 |
| 17 | OD | 63 | F | G surgery a ×1 | HM | HM |
| 18 | OD | 56 | M | CE | HM | CF |
| 19 | OS | 56 | M | CE + IOL (PC) | CF | CF |
a G surgery = patient had glaucoma surgery (not otherwise specified).
Intraoperative Variables
Twenty-one eyes (81%) received a KPro in a fresh corneal donor button, while 5 eyes (19%) received a frozen corneal graft carrier. Concomitant surgeries included extracapsular cataract extraction (11 eyes, 42%), intraocular lens (IOL) explantation (3 eyes, 12%), and IOL repositioning (1 eye, 4%). After initial KPro assembly, 24 eyes (92%) were left aphakic while 2 eyes (8%) were left pseudophakic. No intraoperative complications were encountered.
Visual Acuity Outcomes
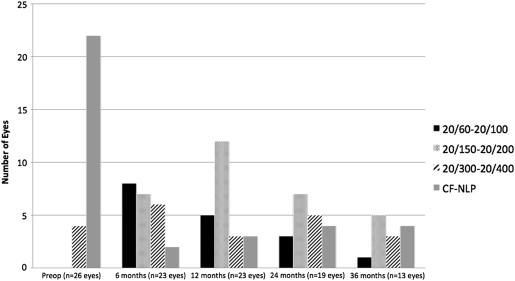
Preoperatively, best-corrected visual acuity (BCVA) was 20/300 or worse (range, light perception [LP] to 20/300). In the contralateral eye, preoperative BCVA was 20/70 or worse (range, LP-20/70). Postoperatively, most patients displayed an improvement in vision ( Figure ). At the last follow-up visit recorded, 14 eyes (54%) achieved BCVA of 20/200 or better (range 20/200–20/70). Final BCVA improved in 17 eyes (65%), while 9 eyes (35%) experienced worsened final BCVA. Visual potential was limited because of postoperative complications in 10 eyes (38%), of which 2 (8%; 2/26) displayed worsening glaucoma on the basis of progressive glaucomatous optic neuropathy, characteristic visual field loss, or elevated intraocular pressure despite maximal therapy. Preexisting comorbidities such as foveal hypoplasia and optic nerve hypoplasia may have also compromised visual rehabilitation in some patients, although this factor is somewhat difficult to quantify with precision.
Postoperative Complications and Management
Retroprosthetic membrane (RPM) formation was the most common complication, occurring in 15 eyes (58%), 9 of which required neodymium-doped–yttrium aluminum garnet (Nd:YAG) laser membranotomy (average 2.44 capsulotomies per eye). Two of the 26 eyes (8%) were refractory to Nd:YAG laser treatment and eventually required surgical membranectomy. Furthermore, 2 additional eyes (8%) necessitated surgical membrane removal without prior Nd:YAG membranotomy. Of the 7 patients that underwent bilateral KPro implantation, 3 patients developed bilateral RPM.
Glaucoma was diagnosed in 23 eyes (88%) after KPro surgery. Definite glaucoma progression was noted in 3 eyes, while 3 additional eyes required glaucoma drainage devices postoperatively to better control intraocular pressure.
In this series, the retention rate of the initial KPro was 77% (20/26), with 6 eyes requiring a keratoprosthesis replacement. Reasons for failure of the initial KPro included infectious keratitis (n = 1), interpseudophakos vascular membrane (n = 1), trans-prosthetic leakage (n = 1), corneal melt around a leaking prosthesis refractory to management with cyanoacrylate glue (n = 1), KPro device extrusion with impeding perforation (n = 1), and device extrusion secondary to RPM formation (n = 1). The latter-mentioned eye experienced slight corneal melting and early device extrusion in his second KPro, managed with a combination of cyanoacrylate glue and sutures. Peri-prosthetic corneal melting also developed bilaterally in 1 patient, who refused any additional interventions at the last follow-up visit. This patient’s visual prognosis was already poor, with an inoperable retinal detachment in a phthisical right eye and a combined retinal and choroidal detachment in the left eye that was also deemed inoperable.
Endophthalmitis was not encountered in this series. Other notable complications occurring in this series are summarized in Table 2 .
| Patient Number | Follow-up (mo) | Latest BCVA | Complications | Additional Interventions |
|---|---|---|---|---|
| 1 | 50 | LP | CD on hypotony; VH; RPM; inoperable CD/RD; corneal melt | PPV ×2 |
| 36 | NLP | SCH; inoperable total RD; RPM; phthisis bulbi; corneal melt | SCH drainage; PPV ×2; SB; epiretinal mb delamination | |
| 2 | 42 | LP | VH; interpseudophakos mb; inoperable RD; epiretinal mb; phthisis bulbi | Nd:YAG ×1; PPV ×3; mb delamination; SB; IOL removal; surgical RPM removal; KPro replacement |
| 3 | 40 | HM | Terminal glaucoma | PPV for floaters |
| 4 | 47 | 20/150 | RPM; glaucoma progression | Nd:YAG ×3; Ahmed valve |
| 5 | 38 | 20/150 | Vitritis; RPM | Nd:YAG ×1 |
| 26 | 20/400 | RPM | Nd:YAG ×3 | |
| 6 | 38 | 20/200 | None | None |
| 26 | 20/100 | Uveitis | None | |
| 7 | 44 | LP | Terminal glaucoma | None |
| 27 | NLP | RPM; CD; vitritis; terminal glaucoma; KPro leak with secondary hypotony; RD; corneal melt | Nd:YAG ×3; PPV ×2; Histoacryl glue ×2; KPro replacement | |
| 8 | 36 | 20/200 | RPM | None |
| 9 | 43 | HM | SCH ×2, CD, VH; hypotony on overfiltering tube; RPM; fibroplastic maculopathy; phthisis bulbi; total RD | SCH drainage ×2; PPV ×2; TS removal; Nd:YAG ×4; surgical RPM removal |
| 10 | 35 | 20/70 | Glaucoma progression | Ahmed valve |
| 7 | 20/150 | Glaucoma progression; CRVO | Ahmed valve | |
| 11 | 31 | 20/200 | Uveitis; RPM | Nd:YAG ×3 |
| 24 | 20/150 | Vitritis/uveitis; RPM; KPro extrusion/impeding perforation | Nd:YAG ×3; KPro replacement | |
| 12 | 35 | 20/200 | None | None |
| 23 | 20/400 | VH | None | |
| 13 | 33 | 20/400 | Uveitis/vitritis; hypotony; CD and RD; trans-KPro leakage; RPM; fibroplastic maculapathy; VH | PPV ×2; CD drainage; KPro replacement; Nd:YAG ×1 |
| 14 | 4 | 20/80 | None | None |
| 15 | 21 | LP | KPro extrusion due to RPM and leakage; RD; slight corneal melt and early extrusion on KPro#2; hypotony; CD; inoperable RD | KPro replacement; surgical RPM removal; PPV; Histoacryl glue and sutures |
| 16 | 10 | 20/80 | None | None |
| 17 | 12 | 20/200 | RPM | None |
| 18 | 10 | NLP | Infectious keratitis; CD; RPM; hypotony; inoperable RD; phthisis bulbi | KPro replacement |
| 19 | 8 | 20/150 | None | None |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


