Purpose
To evaluate the outcomes and complications associated with the repair of rhegmatogenous retinal detachment (RRD) using 25-gauge pars plana vitrectomy (PPV) with selective sclerotomy suturing.
Design
Retrospective case series.
Methods
Analysis of consecutive 25-gauge pars plana vitrectomy cases performed for treating RRD was conducted. Reviewed parameters included demographics, ophthalmic history, results of ocular examinations, and intraoperative as well as postoperative complications. Analysis of the surgery digital video disc recordings revealed complications such as iatrogenic retinal breaks and retinal or subretinal tugging by the soft-tip cannula.
Results
Forty-two eyes with RRD were evaluated with a follow-up of at least 3 months. The preoperative best-corrected visual acuity (BCVA) of 20 eyes with macula-on RRD ranged between 20/20 and 20/40 (mean, 20/30). Twenty-two eyes with macula-off RRD had preoperative BCVA ranging between 20/70 and hand movements (mean, 20/400). The single-surgery success rate was 97.4%. The final BCVA of the macula-on eyes ranged between 20/20 and 20/40 (mean, 20/30). In the eyes with macula-off RRD, the postoperative BCVA ranged between 20/30 and 20/400 (mean, 20/73). Sutures were placed on at least 1 scleral wound because of intraoperative gas leakage in 36.4% of the eyes. On the first postoperative day, all the eyes receiving gas tamponade had a 100% fill. None of the eyes in the study had postoperative hypotony, ciliochoroidal effusion, or choroidal hemorrhage. No cases of postoperative subconjunctival gas or oil leakage were noted.
Conclusions
Modification of the standard 25-gauge sutureless technique with selective scleral wound suturing may contribute to preventing wound leakage and possible postoperative complications of hypotony or partial tamponade.
Transconjunctival 25-gauge pars plana vitrectomy (PPV) has emerged as an important surgical system in vitreoretinal surgery. Advantages of 25-gauge vitrectomy include less traumatic intraocular access with faster patient recovery. Reduced flow with gentler fluidics in high-speed 25-gauge PPV also may help to reduce iatrogenic traction on detached retina during vitrectomy. Success has been reported using 25-gauge sutureless technique in eyes with various vitreoretinal disorders. Recent studies on the use of 25-gauge instrumentation for the repair of rhegmatogenous retinal detachment (RRD) have shown variable results, with single-surgery success rates ranging between 74% and 95.5%.
In this study, we evaluated the outcomes as well as intraoperative and postoperative complications associated with primary repair of RRD with 25-gauge PPV. Specific consideration was given for selective oblique sclerotomy suturing in avoiding postoperative hypotony and complications associated with partial tamponade. In addition, we report the single-surgery anatomic success rate and visual acuity results.
Methods
A retrospective analysis of 42 eyes of 42 patients was conducted after reviewing retinal surgical cases from August 26, 2007, through March 13, 2009. Consecutive patients who underwent 25-gauge PPV for RRD repair were identified. All cases but one were patients with primary RRD without history of prior retinal detachment surgery or vitrectomy. The exception was a patient for whom a radial sponge failed. There were no other exclusion criteria, but in the same time frame, we used scleral buckling surgery in most phakic RRD cases, as well as 20-gauge vitrectomy in traumatic or complicated RRD with advanced proliferative vitreoretinopathy.
The patients’ medical records were reviewed, and age, gender, ophthalmic history, preoperative and postoperative Snellen best-corrected visual acuity (BCVA), results of anterior and posterior segment examinations, and postoperative complications were obtained. The operation reports were reviewed for intraoperative complications as well as scleral wound leakage and subsequent intraoperative suturing of sclerotomies. Complications such as iatrogenic retinal breaks during vitrectomy and retinal or subretinal tugging by the soft-tip cannula during fluid–air exchange were noted from analysis of the surgery digital video disc recordings, which were available for 22 cases. All the patients included in the study had a minimum follow-up of 3 months.
Surgical Technique
All patients received local retrobulbar anesthetics, and the eye was prepared and draped in the standard ophthalmic fashion. Simultaneous clear corneal cataract surgery was performed by the vitreoretinal surgeon (D.H.B.) using standard phacoemulsification technique in 4 cases. A 4- to 5-mm diameter round capsulorrhexis was made to obtain a stable in-the-bag intraocular lens during the vitrectomy procedure, and a 10-0 nylon suture was placed on the corneal incision at the conclusion of cataract surgery to stabilize the wound during subsequent scleral depression. All the 25-gauge PPVs were performed with the Millennium vitreoretinal surgical system (Bausch & Lomb, St Louis, Missouri, USA) and a xenon light source (Alcon Laboratories, Fort Worth, Texas, USA).
The surgical approach consisted of displacing the conjunctiva over the sclerotomy with a swab, which then was created with oblique insertion using a 25-gauge trocar and cannula system (Bausch & Lomb). Cannulas were placed 3 mm posterior to the limbus for pseudophakic eyes and 4 mm posterior to the limbus for phakic eyes. Wide-angle fundus visualization was achieved using the BIOM noncontact wide-field imaging system (Oculus, Munich, Germany).
The PPV began with a core vitrectomy followed by peripheral vitreous dissection with relief of traction at the sites of retinal breaks and along detached retina. Perfluorocarbon liquid (PFCL) was injected thorough a soft-tip cannula (Alcon Laboratories) to fill the eye partially to stabilize the posterior retina and to elevate the vitreous before performing a 360-degree indented anterior vitreous shave. After retinal reattachment under PFCL, an extendable endolaser probe (Synergetics, O’Fallon, Missouri, USA) was used to demarcate the retinal breaks and areas of holes in lattice degeneration with assisted scleral depression. Active fluid–air exchange with a soft-tip extrusion canula (Alcon Laboratories) was used to drain the PFCL up to the level of the most anterior tear. Drainage of loculated anterior subretinal fluid through the preexisting retinal break, followed by intraocular drainage of the floating fluid and remaining PFCL, then was performed. After initial fluid–air exchange, sequestered intraocular fluid was removed from the posterior pole after a wait of 1 minute. In some of the cases, a second round of endolaser was performed under air to treat anterior retinal tears left partially untreated because of partial view.
Choice of tamponading agent varied depending on the location and extent of the retinal breaks. We used 1300 centistokes silicone oil (Arciolane, Toulouse, France), 16% or 14% mixture of perfluoropropane (C 3 F 8 ), or 20% sulfur hexafluoride (SF 6 ). The eyes were flushed with 35 ml gas before initiation of trocar removal.
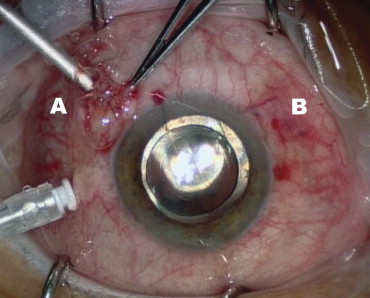
When silicone oil was used, a conjunctival flap over the 3 trocar insertion sites was opened and 7-0 Vicryl sutures (Johnson and Johnson company, St-Stevens-Woluwe, Belgium) were used to close the sclerotomy and conjunctiva in 2 layers. In cases with gas tamponade, suturing of sclerotomies was performed only in leaking trocar insertion sites based on the presence of subconjunctival gas bubbles associated with intraoperative hypotony during sequential trocar extraction ( Figure 1 ). After scleral suturing, additional nonexpansible gas mixture was injected into the vitreous cavity through the maintainer port, or through the sclera with a 30-gauge needle when leakage was evident from the last removed trocar entry wound. Subconjunctival injection of antibiotic (cefuroxime [Zinacef]; Panpharma, Fougères, France) was applied over each sclerotomy site. Antibiotic ointment and dexamethasone 0.1% were placed on the surface of the eye, followed by a patch and shield. In cases with gas tamponade, patients were instructed to position one side down for 10 days.
Results
The study included 42 consecutive patients (42 eyes) who underwent 25-gauge PPV for RRD repair. The mean follow-up was 9 months (range, 3 to 18 months). On presentation, 33 eyes were pseudophakic and 9 eyes were phakic. Four eyes in the phakic group had a +3 cortical cataract, a +2 to +3 posterior subcapsular cataract, or both, and had combined phacoemulsification and intraocular lens plus 25-gauge PPV. Five eyes remained phakic, of which 1 eye had a history of an upper nasal radial sponge placement 10 days earlier for a macula-on RRD. It redetached because of development of a new superior tear.
There were 14 women and 28 men with an average age of 65.8 years (range, 47 to 83 years; standard deviation, 10.2 years) The preoperative BCVA of the 20 eyes (47.6%) with macula-on RRD ranged between 20/20 and 20/40 (mean, 20/30). Twenty-two eyes (52.4%) with macula-off RRD had a preoperative BCVA ranging between 20/70 and hand movements (mean, 20/400).
In 40 eyes (95.4%), retinopexy was applied only around areas of retinal breaks. Two eyes (4.6%) with extensive pigmented lattice and atrophic peripheral changes had additional 360-degree laser barrage. One eye had cryoretinopexy around a lower nasal break. In the phakic group, tamponade choice for all the eyes was 20% SF 6 (all had superior tears between 9 and 3 o’clock). In the 37 pseudophakic cases, 24 eyes (64.9%) received tamponade with 20% SF 6 , 9 eyes (24.3%) received silicone oil, and 3 eyes (8.1%) and 1 eye (2.7%) received tamponade with 14% and 16% C 3 F 8 , respectively. In eyes with at least 1 superior break associated with at an additional break below 4 to 8 o’clock, silicone oil was used. A mixture of 16% C 3 F 8 was chosen in a case with a single break at 5 o’clock. A 14% mixture of C 3 F 8 was used in an eye with a superior break spanning 1.5 hours below 1 o’clock and in 2 eyes with single breaks at 3 to 4 and 8 to 9 o’clock. A nonexpansile mixture of 20% SF 6 was used in all other cases with breaks between 9 and 3 o’clock.
Twelve (36.4%) of the 33 eyes receiving gas tamponade had suture placement on at least 1 leaky sclerotomy. All the eyes filled with silicone oil had scleral suture placement on all 3 sclerotomies. On the first postoperative day, all the eyes receiving gas tamponade had a 100% fill. None of the eyes in the study had postoperative hypotony, ciliochoroidal effusion, or choroidal hemorrhage. No cases of postoperative subconjunctival gas or oil leakage were noted.
The 5 phakic eyes had a +1 to +2 nuclear sclerosis cataract on presentation. On the first postoperative day, 4 of the 5 eyes had gas-induced posterior feathering of the lens with poor view of the fundus. During follow-up, the lens returned to its baseline clarity within 2 to 4 weeks. None of these eyes had progression of the cataract during the follow-up.
Two of the 9 eyes that had silicone oil tamponade displayed mild anterior chamber flare lasting more than 1 month after surgery. In all cases, the silicone oil was removed after 3 months from the initial RRD repair. None of these cases displayed hypotony after oil removal or signs of uveitis.
The single operation success rate was 41 (97.6%) of 42. One pseudophakic eye redetached on postoperative day 5 because of progression of inferior proliferative vitreoretinopathy. In 3 pseudophakic eyes, visually significant postoperative epiretinal membrane (ERM) developed that was diagnosed at 4 to 12 weeks after the RRD surgery. All 3 underwent a subsequent 25-gauge ERM peel. The final BCVA of the 20 eyes with macula-on RRD ranged between 20/20 and 20/40 (mean, 20/30). In the 22 eyes with macula-off RRD, the postoperative BCVA ranged between 20/30 and 20/400 (mean, 20/73).
Analysis of available digital video disc recordings of 22 cases for events of iatrogenic retinal breaks caused by the vitreous cutter revealed 2 occurrences of a single iatrogenic round hole in an area of detached retina. Enlargement of a preexisting retinal break during air–fluid exchange by the soft-tip cannula requiring additional laser was observed in 2 cases. Two cases also displayed mild temporary hemorrhage at the edge of the tear after tugging by the active soft-tip extrusion cannula during air–fluid exchange.
In 1 phakic case, a pigmented subconjunctival scar was noted by the patient at the upper-nasal sclerotomy insertion site ( Figure 2 ). The pigmentation slowly disappeared within a few months.



