Purpose
To develop and evaluate a new implantable collamer lens (ICL) sizing method that uses high-frequency ultrasound biomicroscopy (UBM).
Design
Interventional case series.
Methods
ICL were implanted in 47 eyes of 25 patients (8 male, 17 female, mean age 34.7 ± 6.8 years). At 3 months after ICL surgery, the vault (distance between ICL and crystalline lens) was measured using anterior optical coherence tomography (OCT). Stepwise multiple regression analysis was performed in order to determine the optimal ICL size that will be expected to achieve a 0.5-mm vault, and the regression equation was calculated. Mean keratometric power, axial length, anterior chamber depth, sulcus-to-sulcus (STS) diameter, and distance between STS plane and crystalline lens were applied as candidates for explanatory variables. Subsequently, the equation was applied to a new group of patients (81 eyes of 43 patients, 20 male and 23 female, mean age 35.6 ± 7.2 years) in order to decide the ICL size. Postoperative vault was evaluated at 3 months after surgery. Main outcome measures were mean postoperative vault and percentages of eyes that achieved moderate vault.
Results
The regression equation was determined using 3 explanatory variables: anterior chamber depth (ACD), STS diameter, and distance between STS plane and anterior crystalline lens surface (STSL). The mean vault error (postoperative vault – predicted vault) was −0.06 ± 0.29 mm. Of the total number of eyes, 88.9% had a vault between 0.15 and 1.0 mm. None of the eyes had a low vault (<0.15 mm). Nine eyes (11.1%) had a high vault (>1.0 mm).
Conclusion
A novel ICL sizing equation was developed and shown to be an effective method for calculation of the optimal ICL size in order to achieve an appropriate vault.
An implantable collamer lens (ICL; STAAR Surgical, Monrovia, California, USA) is a posterior chamber–type phakic intraocular lens that is designed to be implanted in the ciliary sulcus. Determination of ICL size is crucial in order to achieve a successful result. A too-large ICL will result in shallowness of the anterior chamber and an increased risk of angle-closure or pupillary block glaucoma. On the other hand, a too-small ICL will result in a decreased distance between the ICL and crystalline lens and in an increasing risk of cataract formation. Conventionally, ICL size has been determined based on the horizontal corneal diameter (white-to-white, WTW) and anterior chamber depth (ACD). However, accumulated reports have revealed that there is a poor correlation between ciliary sulcus-to-sulcus (STS) diameter and WTW measurement. Choi and associates determined ICL size using conventional 50-MHz ultrasound biomicroscopy (UBM). Even though only a small number of cases were evaluated, the UBM method was superior to conventional methods for achieving a moderate vault. The emergence of high-frequency UBM with a wide scanning field has enabled direct measurement of STS diameter.
Vault changes according to the difference between ICL size and STS diameter. Gonvers and associates reported that there was no contact between the ICL and crystalline lens in cases with the central vaulting equal to or greater than 0.15 mm. They concluded that 0.15 mm of central vaulting should be the minimum target for ICL implantation. Therefore, in the present report, the lower limit of vaulting was set at 0.15 mm.
Recently, Dougherty and associates conducted a multicenter study that reported a regression equation to calculate optimal ICL size. They used STS and ICL power as explanatory variables. Since the distance between the fixed position of the ICL and crystalline lenses can affect ICL vault, a new parameter was created in the present study: the distance between STS plane and anterior crystalline lens surface (STSL).
The purpose of this study was to develop an equation using stepwise multiple regression analysis for determination of appropriate ICL size, and then to validate the efficacy of the equation by investigating postoperative vault.
Methods
Subjects in the Implantable Collamer Lens Sizing Equation Study
A total of 45 eyes of 24 consecutive patients (12 male, 12 female, mean age 34.3 ± 6.6 years) who underwent ICL surgery at Nagoya Eye Clinic were enrolled in the study. Patient demographics are shown in Table 1 . Patients were excluded if they had other ocular diseases except for refractive error. The mean manifest refractive sphere and cylinder of these subjects were −9.22 ± 3.08 diopters (D; range −3.75 to −24.0 D) and −0.95 ± 0.78 D (range 0 to −2.75 D), respectively. The ICL size was determined with a conventional STAAR sizing nomogram that calculated the size from the 2 parameters of WTW and anterior chamber depth.
| Mean ± Standard Deviation (Range) | |
|---|---|
| Number of patients (eyes) | 24 (45) |
| Age (years) | 34.3 ± 6.6 (22 to 45) |
| Sex (female, male) | 12, 12 |
| Manifest refractive sphere (D) | −9.22 ± 3.08 (−3.75 to −15.5) |
| Manifest refractive cylinder (D) | −0.95 ± 0.78 (0 to -2.75) |
| Axial length (mm) | 27.9 ± 1.3 (25.8 to 31.3) |
| Anterior chamber depth (mm) | 3.25 ± 0.27 (2.77 to 3.81) |
| Ciliary sulcus-to-sulcus diameter (mm) | 11.79 ± 0.44 (11.17 to 12.95) |
| STS to anterior lens surface distance (STSL) (mm) | 0.31 ± 0.18 (-0.04 to 0.69) |
| Implanted ICL power (D) | −14.17 ± 3.77 (-6.0 to -22.5) |
Regression Equation Validation Study Subjects
A total of 81 eyes of 43 patients (21 male, 22 female, mean age 35.6 ± 7.2 years) who underwent ICL implantation surgery were enrolled in the study. Patient demographics are shown in Table 2 . The mean manifest refractive sphere and cylinder of these subjects were −9.21 ± 3.34 D (range −3.25 to −24.0 D) and −1.12 ± 0.95 D (range 0 to −3.75 D), respectively.
| Mean ± Standard Deviation (Range) | |
|---|---|
| Number of patients (eyes) | 43 (81) |
| Age (years) | 35.6 ± 7.2 (25 to 48) |
| Sex (female, male) | 23, 20 |
| Manifest refractive sphere (D) | −9.21 ± 3.34 (-3.25 to -24.0) |
| Manifest refractive cylinder (D) | −1.12 ± 0.95 (0 to -3.75) |
| Anterior chamber depth (mm) | 3.08 ± 0.26 (2.63 to 3.61) |
| Ciliary sulcus-to-sulcus diameter (mm) | 11.74 ± 0.57 (11.17 to 12.95) |
| STS to anterior lens surface distance (mm) | 0.35 ± 0.20 (0 to 0.82) |
| Implanted ICL size | 12.7 ± 0.37 (12.1 to 13.2) |
Multiple Regression Analysis
Before ICL implantation surgery, mean keratometric value (ARK-530A; Nidek, Gamagori, Japan), axial length (IOL Master; Carl Zeiss Meditec, Jena, Germany), anterior chamber depth (IOL Master; Carl Zeiss Meditec), and STS (VumaxII; SONOMED Inc, Lake Success, New York, USA) and STSL (VumaxII) were measured. At 3 months after surgery, vault was measured using anterior OCT (Visante; Carl Zeiss Meditec). From the observation that ICL vault increases 1.1 times higher along the compression length in a balanced salt solution (BSS) (STAAR proprietary data), optimal ICL size to achieve 0.5-mm vault was estimated with the following equation:
Optimal ICL size = Implanted ICL size + ( 0.5 − Postoperative vault ) / 1.1.
Then, stepwise multiple regression analysis was performed in order to evaluate the correlation between optimal ICL size and other ocular parameters. The dependent variable was optimal ICL size. The candidates of an explanatory variable included mean keratometric value, axial length, STS, STSL, and ICL spherical power. In the regression analysis, a variance inflation factor was calculated and the amount of multicollinearity was assessed.
Ultrasound Biomicroscopy Scanning System
A high-frequency B-scan diagnostic ultrasound biomicroscopy imaging system (VumaxII) was employed in the present study. The system has a scanning field depth of 18.5 × 14 mm, and can capture the entire anterior segment in a single scan. The sampling rate was 22 frames/s. A headpiece with a 35-MHz transducer was used for STS and STSL measurement. The axial and lateral resolution in the anterior segment with a 12-mm height were 0.022 mm and 0.38 mm, respectively. The repeatability of STS measurements has been previously evaluated, and the coefficient of variation was 0.62%. A single, experienced examiner carried out all UBM measurements.
Measurements of Ciliary Sulcus-to-Sulcus Diameter and Distance Between Ciliary Sulcus-to-Sulcus Plane and Anterior Crystalline Lens Surface Using High-frequency Ultrasound Biomicroscopy
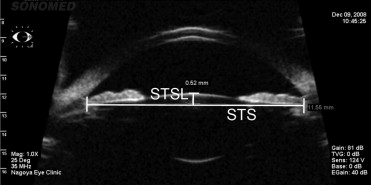
Topical anesthesia consisting of oxybuprocaine hydrochloride 0.4% (Benoxil ophthalmic solution; Santen, Osaka, Japan) was administered, and an appropriately sized eyecup (18.0, 20.0, 22.0, or 24.0 mm diameter) was used depending on interpalpebral size. The eyecup was filled with sterile normal saline, and the subject was asked to fixate a target on the ceiling with the fellow eye in order to maintain fixation. The probe was immersed to the water surface vertically, and sectional images were taken on the horizontal meridian. The probe was moved horizontally along the superior-inferior axis and images were recorded as a movie. The examiner captured the images according to the following 3 conditions. First, corneal, posterior, and anterior lens capsule references were in 1 image, and these structures were located at a position symmetrical to a central vertical line in the scanned area. Second, the ciliary sulcus was kept at a depth of 12 mm in order to achieve the best resolution. Third, the examiner kept the largest pupil size during consecutive scans. After 6 still images were chosen from recording video frames in which the STS was captured clearly, the end of the high reflective line on the back surface of the iris was defined as the ciliary sulcus. Subsequently, STS was measured manually using a digital caliper. After excluding maximum and minimum values of 6 measurements, the mean STS value was calculated. Similarly, the distance between the STS line and the anterior surface of the crystalline lens was measured. STS and STSL in the representative UBM image are shown in Figure 1 . When the STS plane was posterior to the anterior crystalline lens surface, STSL was defined as a positive value.
Implantable Collamer Lens Implantation Surgery
Two weeks before ICL implantation, 2 peripheral laser iridotomies using neodymium:YAG and an argon laser were performed at the 10:30 and 1:30 clock-hour positions. Details of the ICL implantation procedure have been described previously. Briefly, topical anesthesia was administered. Paracentesis was then performed with the aqueous humor replaced by a viscoelastic material (Opegan; Santen Pharmaceuticals, Osaka, Japan). Subsequently, an injector cartridge (STAAR Surgical) was used to insert the ICL through a sutureless 2.9-mm temporal clear corneal incision. After initially placing the ICL on the iris, a specially designed manipulator was used to place 4 haptics behind the iris. Once correct ICL positioning in the center of the pupillary zone was confirmed, an intraocular mitotic was applied, followed by irrigation of the anterior chamber with a balanced salt solution. Postoperatively, 250 mg acetazolamide was taken orally in order to decrease intraocular pressure. Intraocular pressure was measured 2 hours after surgery. Topical moxifloxacin was administered locally 4 times daily for 4 weeks.
Calculation of Predicted Vault
Since ICL was manufactured with 0.5-mm length increments, ICL with exact length as calculated from the equation cannot be implanted. Therefore, predicted vault was calculated as follows to validate the equation:
Predicted vault = ( Postoperative vault in the present study ) + 1.1 ( ICL size calculated from the each equation / nomogram − implanted ICL size )
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


