Purpose
To characterize the optical coherence tomography (OCT) angiography, en face OCT, and microperimetry features of paracentral acute middle maculopathy in both the acute phase and after resolution, and to propose a classification of distinct subtypes of this entity.
Design
Retrospective observational case series.
Methods
Clinical histories, high-resolution digital color imaging, spectral-domain OCT images, fluorescein angiography, OCT angiography images, and en face OCT images of 16 patients with paracentral acute middle maculopathy were evaluated. Microperimetry was available in 6 patients.
Results
The most common referring diagnoses were isolated branch retinal arterial occlusion (5/16), combined central retinal vein and cilioretinal artery occlusion (4/16), and isolated central retinal vein occlusion (4/16). All patients demonstrated hyperreflective plaque-like lesions at the level of the inner nuclear layer on spectral-domain OCT, with no fluorescein angiographic correlate. OCT angiography demonstrated variable areas of capillary dropout within the superficial and deep retinal capillary plexi in these areas. En face OCT highlighted confluent areas of middle retina hyperreflectivity corresponding to these lesions. Three distinct en face OCT patterns were observed: arteriolar, fern-like, and globular. Microperimetry demonstrated relative scotomas mapping to the area of middle retinal hyperreflectivity seen on en face OCT.
Conclusions
Paracentral acute middle maculopathy may be best evaluated with the use of en face OCT imaging, which corresponds to subjective and objective visual field defects. En face OCT appearance may be used to classify paracentral acute maculopathy into distinct subtypes.
Paracentral acute middle maculopathy is a recently characterized presentation of deep retinal capillary ischemia, manifesting as hyperreflective bands within the middle retina on spectral-domain optical coherence tomography (OCT) imaging. While the initial description detailed lesions occurring in isolation, subsequent reports have observed this finding in conjunction with other retinovascular conditions, including branch (BRAO) and central (CRAO) retinal arterial occlusion, central retinal vein occlusion (CRVO), diabetic retinopathy, sickle cell retinopathy, and Purtscher retinopathy. Most recently, Christenbury and associates described the first case of paracentral acute middle maculopathy imaged with OCT angiography, demonstrating attenuation of the deep capillary plexus in the area of involvement. Taken together, these observations further support a vaso-occlusive origin for these lesions.
The purpose of the current study was to describe the natural evolution of paracentral acute middle maculopathy in 16 additional cases evaluated with OCT angiography, and to better elucidate the involvement of the adjacent retinal capillary plexuses, which to date have been unable to be adequately assessed with traditional fluorescein angiography. Furthermore, these findings were correlated to en face OCT imaging, which has not been previously reported for this condition, and microperimetry, when available. A new classification of distinct subtypes of paracentral acute middle maculopathy is then proposed based on en face OCT appearances.
Methods
Institutional review board approval was obtained through the Wills Eye Hospital, Philadelphia, Pennsylvania, for a retrospective observational case series. Research adhered to the tenets of the Declaration of Helsinki and was conducted in accordance with regulations set forth by the Health Insurance Portability and Accountability Act (HIPAA).
Clinical records and imaging were reviewed to identify all cases with spectral-domain OCT imaging showing paracentral acute middle maculopathy lesions at a single academic private-practice office location from January 1, 2015 to July 30, 2015. Available en face OCT and OCT angiogaphy imaging cases were identified. OCT angiography and en face OCT was performed using the Avanti RTVue XR (Optovue, Fremont, California, USA), which obtains volumetric data from horizontal and vertical acquisitions that can be automatically segmented to specific depths. Using these data, side-by-side OCT angiography and en face OCT images can be generated at the levels of the superficial capillary plexus, the deep capillary plexus, the normally avascular outer retina, and the choriocapillaris. Baseline and follow-up demographic, clinical, laboratory, and imaging data were extracted from patient charts. High-resolution digital color photography, fluorescein angiography, and red-free photography were included in review, when available, for each patient. Microperimetric examination using the Macular Integrity Assessment (MAIA; CenterVue, Padova, Italy) was available and reviewed for 6 patients.
Results
The patient demographic, ocular examination, imaging, and microperimetry findings (when available) are summarized in Table 1 . The mean age at presentation was 53 years, and 9 of the 16 patients (56%) were male. Ten individuals (63%) presented with acute-onset nonspecific visual loss, 3 (19%) reported a paracentral scotoma, and 3 (19%) described an altitudinal field cut. Of the 10 patients with sudden vision loss, 2 (20%) experienced a partial resolution of symptoms within 30 minutes of onset.
| Patient | Age (Years) | Sex | Eye | Symptom | Referring Diagnosis | Associated Condition | VA Presentation | Deep Capillary Plexus OCT-A Findings | Middle Retina En Face OCT Pattern | Microperimetry Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 41 | M | OS | Vision loss | CRVO/CR | Beta thalassemia | 20/20 | Normal flow | Arteriolar | N/A |
| 2 | 56 | F | OD | Vision loss | CRAO | HSV uveitis | CF | Capillary dropout | Arteriolar | N/A |
| 3 | 82 | M | OD | Field cut | BRAO | HTN | 20/25 | Normal flow | Arteriolar | N/A |
| 4 | 65 | M | OS | Vision loss | BRAO | HTN, chiropractic procedure | 20/25 | Normal flow | Arteriolar | N/A |
| 5 | 17 | M | OD | Vision loss | BRAO | Prepapillary vascular loop, trauma | 20/40 | Capillary dropout | Arteriolar | N/A |
| 6 | 73 | M | OS | Field cut | BRAO | HTN, carotid occlusion | 20/40 | Capillary dropout | Arteriolar | Altitudinal field cut |
| 7 | 52 | F | OS | Vision loss | CRVO/CR | Transcontinental flight/dehydration | 20/60 | Normal flow | Arteriolar | Altitudinal field cut |
| 8 | 75 | M | OD | Paracentral scotoma | BRAO | HTN, post-cardiac catheterization | 20/25 | Normal flow | Arteriolar | N/A |
| 9 | 60 | F | OS | Paracentral scotoma | BRAO | HTN, DM | 20/40 | Capillary dropout | Arteriolar | Paracentral scotoma |
| 10 | 76 | M | OD | Vision loss | CRVO/CR | HTN | 20/40 | Normal flow | Arteriolar | N/A |
| 11 | 93 | M | OD | Vision loss | CRVO/CR | HTN | 20/40 | Normal flow | Arteriolar/fern-like | N/A |
| 12 | 52 | M | OD | Vision loss | CRVO | Amyloidosis | 20/25 | Normal flow | Fern-like | Paracentral scotoma |
| 13 | 21 | F | OU | Vision loss | BRAO OU | Sickle cell disease, dehydration on cruise ship | 20/25 OD 20/200 OS | Capillary dropout OU | Multifocal globular | N/A |
| 14 | 34 | F | OS | Vision loss | BRAO | Cosmetic facial filler injection | HM a | Capillary dropout | Focal globular | N/A |
| 15 | 26 | F | OS | Paracentral scotoma | BRAO | Mechanical heart valve on anticoagulation | 20/30 | Normal flow | Focal globular | Paracentral scotoma |
| 16 | 21 | F | OU | Vision loss | BRAO | Post-viral illness, Purtscher-like | CF OU | Normal flow OU | Multifocal globular | Paracentral scotoma |
The most common referring diagnoses were isolated BRAO (5/16, 31%), combined CRVO with cilioretinal artery occlusion (4/16, 25%), and isolated CRVO (4/16, 25%). Seven patients had known histories of hypertension; 1 of these patients also had diabetes mellitus, 1 patient presented after cardiac catheterization, and another lost vision 1 hour after a chiropractic procedure. Associated conditions in the remaining 9 patients included recent cosmetic facial filler injection, post-viral illness, amyloidosis, beta thalassemia, presumed herpes simplex uveitis, prepapillary vascular loop with trauma, sickle cell anemia with dehydration on a cruise ship, mechanical heart valve on anticoagulation, and transcontinental flight with dehydration.
Snellen best-corrected visual acuity (BCVA) on presentation ranged from 20/20 to hand motions. Two individuals (13%) had bilateral vision loss; vision in these cases was finger count OU and 20/25 OD and 20/200 OS, respectively. The patient with hand motions visual acuity had concurrent ischemic optic neuropathy.
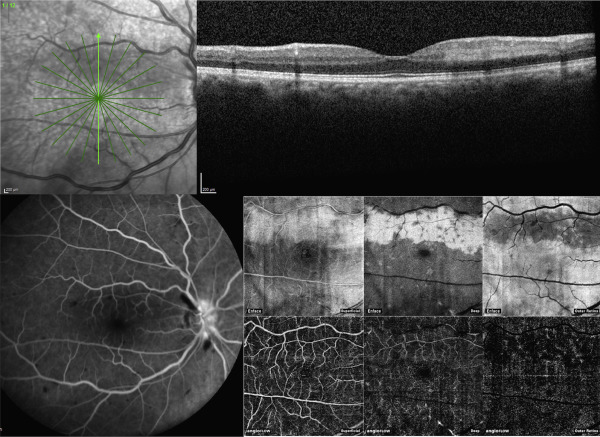
All patients demonstrated hyperreflective plaque-like lesions at the level of the inner nuclear layer on spectral-domain OCT, consistent with paracentral acute middle maculopathy ( Figure 1 top ). Fluorescein angiography did not consistently reveal any correlate to these lesions ( Figure 1 bottom left). En face OCT highlighted confluent areas of middle retina hyperreflectivity corresponding to the lesions ( Figure 1 bottom right). OCT angiography demonstrated variable areas of capillary dropout within the superficial and deep retinal capillary plexi in the area corresponding to the paracentral acute middle maculopathy lesions ( Figure 1 , bottom right, bottom row). Microperimetry disclosed relative scotomas mapping to the area of middle retinal hyperreflectivity as seen on en face OCT ( Figure 2 ).
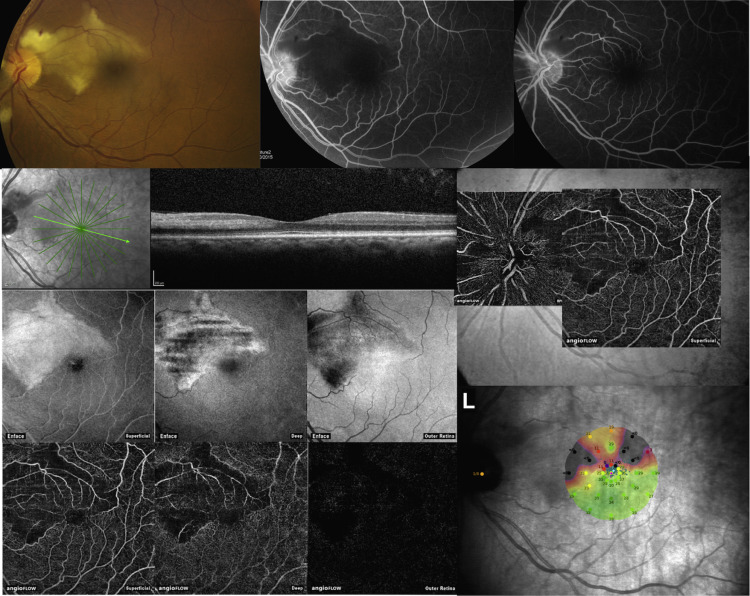
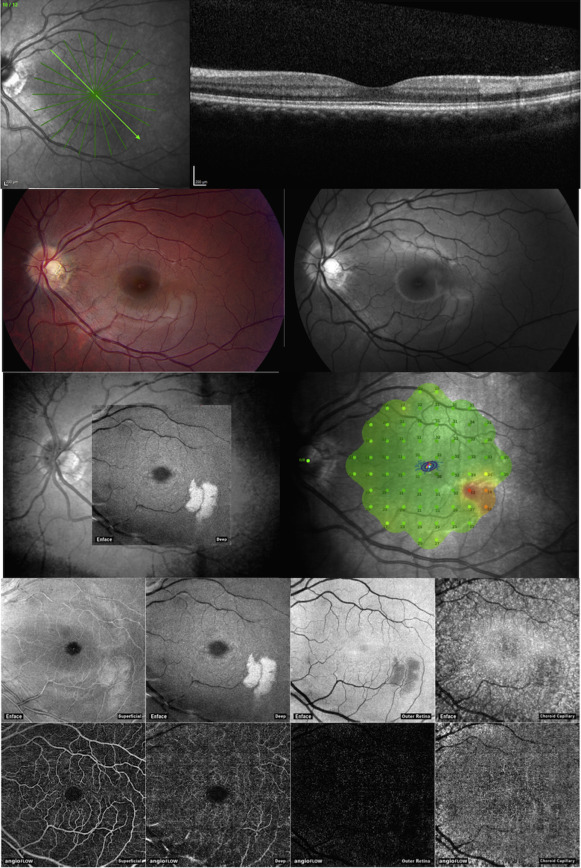
Three distinct patterns of these areas on en face OCT were observed: arteriolar, globular, and fern-like ( Table 2 ). The arteriolar pattern was seen in 11 patients (63%) and showed a characteristic band-like middle retina hyperreflectivity mirroring the distribution of a large retinal arteriole ( Figure 2 ). The globular pattern was noted in 4 patients (25%) with either a focal ovoid patch or multifocal ovoid patches of middle retina hyperreflectivity ( Figure 3 ). The fern-like pattern was observed in 2 patients (13%) in the setting of CRVO with multilobulated parafoveal middle retina hyperreflectivity ( Figure 4 ). Of note, 1 patient with a combined CRVO and cilioretinal artery occlusion had both the arteriolar and fern-like pattern.
| Pattern | Appearance | Presumed Mechanism |
|---|---|---|
| Arteriolar | Band-like areas in distribution of major arteriole | Transient or true arterial occlusion |
| Fern-like | Multilobulated central area tracking along veins | Perivenular capillary ischemia |
| Globular | Ovoid focal or multifocal areas | Distal precapillary or capillary ischemia |
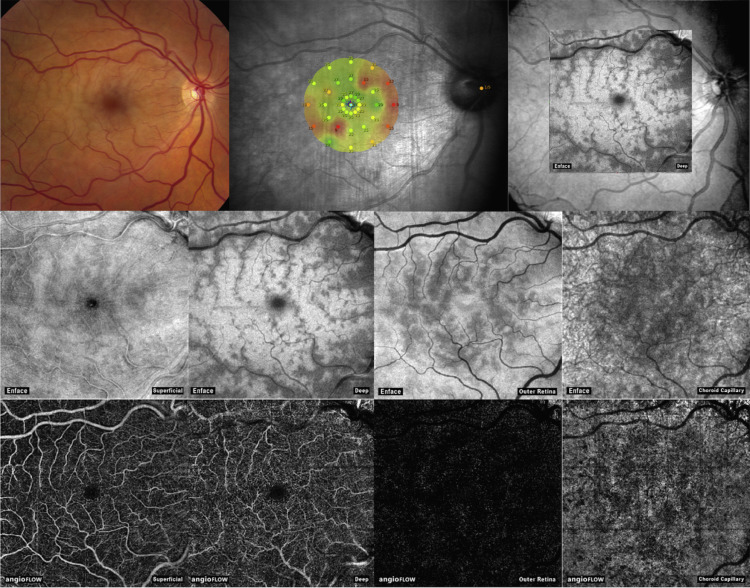
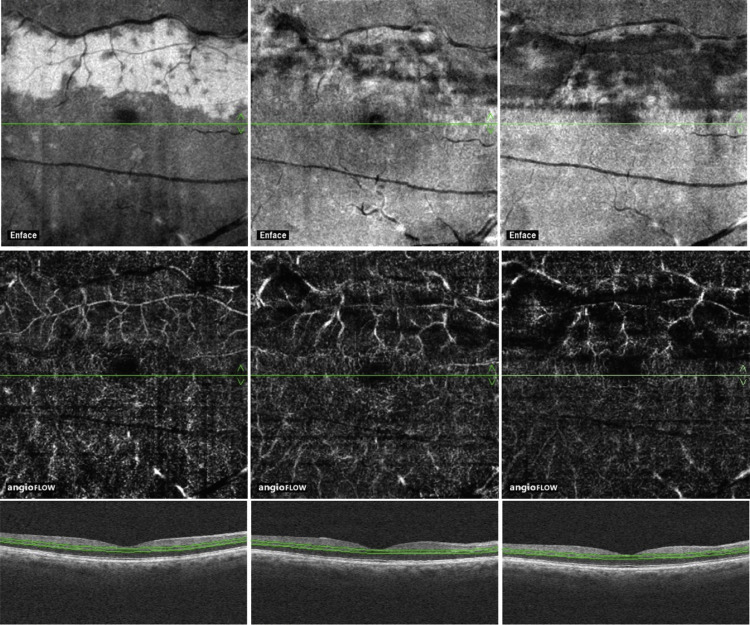
On follow-up en face OCT, areas of middle retina hyperreflectivity showed resolution, with variable areas of hyporeflectivity representing middle retinal atrophy ( Figure 5 ). OCT angiography of the deep capillary plexus showed capillary dropout in the same areas.
Results
The patient demographic, ocular examination, imaging, and microperimetry findings (when available) are summarized in Table 1 . The mean age at presentation was 53 years, and 9 of the 16 patients (56%) were male. Ten individuals (63%) presented with acute-onset nonspecific visual loss, 3 (19%) reported a paracentral scotoma, and 3 (19%) described an altitudinal field cut. Of the 10 patients with sudden vision loss, 2 (20%) experienced a partial resolution of symptoms within 30 minutes of onset.
| Patient | Age (Years) | Sex | Eye | Symptom | Referring Diagnosis | Associated Condition | VA Presentation | Deep Capillary Plexus OCT-A Findings | Middle Retina En Face OCT Pattern | Microperimetry Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 41 | M | OS | Vision loss | CRVO/CR | Beta thalassemia | 20/20 | Normal flow | Arteriolar | N/A |
| 2 | 56 | F | OD | Vision loss | CRAO | HSV uveitis | CF | Capillary dropout | Arteriolar | N/A |
| 3 | 82 | M | OD | Field cut | BRAO | HTN | 20/25 | Normal flow | Arteriolar | N/A |
| 4 | 65 | M | OS | Vision loss | BRAO | HTN, chiropractic procedure | 20/25 | Normal flow | Arteriolar | N/A |
| 5 | 17 | M | OD | Vision loss | BRAO | Prepapillary vascular loop, trauma | 20/40 | Capillary dropout | Arteriolar | N/A |
| 6 | 73 | M | OS | Field cut | BRAO | HTN, carotid occlusion | 20/40 | Capillary dropout | Arteriolar | Altitudinal field cut |
| 7 | 52 | F | OS | Vision loss | CRVO/CR | Transcontinental flight/dehydration | 20/60 | Normal flow | Arteriolar | Altitudinal field cut |
| 8 | 75 | M | OD | Paracentral scotoma | BRAO | HTN, post-cardiac catheterization | 20/25 | Normal flow | Arteriolar | N/A |
| 9 | 60 | F | OS | Paracentral scotoma | BRAO | HTN, DM | 20/40 | Capillary dropout | Arteriolar | Paracentral scotoma |
| 10 | 76 | M | OD | Vision loss | CRVO/CR | HTN | 20/40 | Normal flow | Arteriolar | N/A |
| 11 | 93 | M | OD | Vision loss | CRVO/CR | HTN | 20/40 | Normal flow | Arteriolar/fern-like | N/A |
| 12 | 52 | M | OD | Vision loss | CRVO | Amyloidosis | 20/25 | Normal flow | Fern-like | Paracentral scotoma |
| 13 | 21 | F | OU | Vision loss | BRAO OU | Sickle cell disease, dehydration on cruise ship | 20/25 OD 20/200 OS | Capillary dropout OU | Multifocal globular | N/A |
| 14 | 34 | F | OS | Vision loss | BRAO | Cosmetic facial filler injection | HM a | Capillary dropout | Focal globular | N/A |
| 15 | 26 | F | OS | Paracentral scotoma | BRAO | Mechanical heart valve on anticoagulation | 20/30 | Normal flow | Focal globular | Paracentral scotoma |
| 16 | 21 | F | OU | Vision loss | BRAO | Post-viral illness, Purtscher-like | CF OU | Normal flow OU | Multifocal globular | Paracentral scotoma |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


