The emergence and refinement of flexible endoscopes during the second half of the twentieth century has facilitated flexible bronchoscopy’s rise as the standard for evaluation of and often intervention in the tracheobronchial tree. Many of these procedures require only topical anesthesia and may be conducted in office settings without sedation. The relocation of procedures previously reserved for the operating room or endoscopy suite confers cost savings, improves provider flexibility, and maintains patient safety while increasing satisfaction and limiting convalescence.
Key points
- •
Numerous diagnostic and therapeutic airway procedures may be performed on awake patients in the otolaryngologist’s office.
- •
With careful patient selection and pre-procedural counseling, acceptance and tolerance of unsedated airway procedures are high.
- •
Published outcomes demonstrate efficacy and safety comparable to their sedated or operating room counterparts and are accompanied by lower costs and more expeditious patient recovery.
Overview
Airway compromise results from numerous causes presenting with a relatively limited symptom profile, including dyspnea, stridor, hoarseness, and hemoptysis. Pathology of the upper airway can be categorized as
- •
Idiopathic
- •
Inflammatory (granulomatous diseases, polychondritis)
- •
Neoplastic (benign, malignant, metastatic)
- •
Acquired stenosis or vocal fold paralysis (trauma, postintubation, tracheotomy, postsurgical)
- •
Congenital
The use of mechanical ventilator support, endotracheal intubation, and tracheotomy expanded significantly during the mid-twentieth century amidst the polio epidemic and continues to be a major constituent in the care of hospitalized patients who are surviving complex injuries and disease. Subglottic and tracheal stenosis resulting from these measures account for a large percentage of patients with symptomatic airway obstruction. Rates of postintubation subglottic stenosis are estimated at 0.9% to 8.3%. Recognized factors increasing a ventilated patient’s risk of airway stenosis include duration of intubation and size of endotracheal tube.
Airway narrowing may exist for a generous period of time before the obstruction becomes apparent, and this is particularly true in less-active patients who lead sedentary lives. Typically, narrowing of the airway must reach 30% before symptoms appear at rest. The workup of such patients might include imaging and pulmonary function testing, but of paramount importance is endoscopic assessment, necessary for locating, characterizing, and often treating airway obstruction. Treatment options for laryngotracheal stenosis include observation, endoscopic dilation with or without laser assistance, stent placement, open airway surgery, and tracheotomy.
Overview
Airway compromise results from numerous causes presenting with a relatively limited symptom profile, including dyspnea, stridor, hoarseness, and hemoptysis. Pathology of the upper airway can be categorized as
- •
Idiopathic
- •
Inflammatory (granulomatous diseases, polychondritis)
- •
Neoplastic (benign, malignant, metastatic)
- •
Acquired stenosis or vocal fold paralysis (trauma, postintubation, tracheotomy, postsurgical)
- •
Congenital
The use of mechanical ventilator support, endotracheal intubation, and tracheotomy expanded significantly during the mid-twentieth century amidst the polio epidemic and continues to be a major constituent in the care of hospitalized patients who are surviving complex injuries and disease. Subglottic and tracheal stenosis resulting from these measures account for a large percentage of patients with symptomatic airway obstruction. Rates of postintubation subglottic stenosis are estimated at 0.9% to 8.3%. Recognized factors increasing a ventilated patient’s risk of airway stenosis include duration of intubation and size of endotracheal tube.
Airway narrowing may exist for a generous period of time before the obstruction becomes apparent, and this is particularly true in less-active patients who lead sedentary lives. Typically, narrowing of the airway must reach 30% before symptoms appear at rest. The workup of such patients might include imaging and pulmonary function testing, but of paramount importance is endoscopic assessment, necessary for locating, characterizing, and often treating airway obstruction. Treatment options for laryngotracheal stenosis include observation, endoscopic dilation with or without laser assistance, stent placement, open airway surgery, and tracheotomy.
Indications
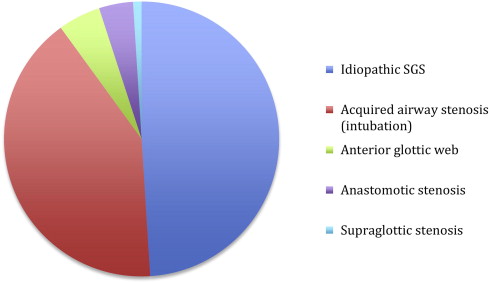
The primary indication for office-based airway surgery is the treatment of stenosis, the most common cause being idiopathic subglottic stenosis. Acquired tracheal or more distal stenosis and glottic webs are the second and third most common indications for in-office airway procedures. Fig. 1 displays the most common reasons that bring patients to our center for office-based airway surgery.
Other indications for office-based airway intervention include biopsy of suspicious lesions, secondary tracheoesophageal puncture, foreign body retrieval, and treatment of recurrent respiratory papillomatosis. Furthermore, office-based airway procedures are ideal for those in whom sedated or operative procedures are difficult or impossible because of significant comorbidity, cervical spine disease, morbid obesity, maxillofacial challenges, or extensive laryngotracheal papillomas.
Preoperative planning
Before office-based airway surgery, patients should be counseled and prepared on what to expect. If undue anxiety is encountered, the procedure should be performed under intravenous sedation or general anesthesia. It is helpful to reassure patients that “they are in control” and that they may terminate the procedure at any time should they experience significant discomfort. Maintaining communication with the patient during the procedure, placing a hand on the patient’s shoulder, and making intermittent eye contact when possible helps ensure patient comfort and a successful outcome. A nurse opposite the endoscopist holding the patient’s hand or explaining the steps of the procedure into the patient’s ear is also beneficial in maximizing patient comfort and reducing anxiety.
Office-based tracheobronchoscopy, laser airway surgery, and balloon tracheoplasty may induce hemodynamic changes and exacerbate reactive airway disease. Mean arterial pressure, heart rate, cardiac index, and pulmonary arteriolar occlusion pressure have all been shown to significantly increase during bronchoscopy. Surgery on the glottis and trachea can stimulate a reflex sympathetic discharge and result in ST segment alterations as well as significant decreases in forced expiratory volume in one second, forced vital capacity, and peak inspiratory and expiratory flow. Caution must be exercised when considering office-based airway surgery on patients with cardiopulmonary disease, and the possibility of hemodynamic changes associated with awake procedures must be weighed against the risks of intravenous sedation or general anesthesia.
Preparation and patient positioning
In addition to patient counseling and informed consent, adequate preparation for an office-based airway procedure requires assembling appropriate equipment and staff as well as achieving sufficient topical anesthesia. Any of a variety of endoscopes may be selected for the procedure; preferred are ultrathin distal chip bronchoscopes or esophagoscopes. The patient is comfortably seated upright in a standard examination chair positioned in front of a viewing screen linked to a recording system. When an intervention is anticipated, appropriate equipment, such as biopsy forceps, brushes, guide wires, laser fibers, and hydrostatic balloons, should be available. For patient safety and comfort, at least one, and ideally two assistants are required for office-based airway surgery.
Our technique of patient preparation is aimed at maximizing comfort which is essential for a successful procedure.
- •
First, topical anesthesia of 6 mL of 4% lidocaine is delivered via nebulizer, which is well tolerated and takes approximately 10 minutes to dispense ( Fig. 2 ).
Fig. 2
Administration of 6 mL of 4% lidocaine via nebulizer before the procedure.
- •
Then, the patient’s more patent nasal cavity is topically anesthetized and decongested with a combination of 1:1 oxymetazoline hydrochloride (0.05%) and lidocaine hydrochloride topical solution (4%).
- •
Patients are instructed on what to expect throughout the duration of the procedure and informed that should they experience any undue discomfort to raise their hand to suspend the procedure.
- •
The ultrathin endoscope with a 2-mm working channel (Pentax VE-1530 transnasal esophagoscope, Pentax Precision Medical Co, KayPentax, Lincoln Park, NJ) is placed and positioned above the glottis.
- •
The endoscope is repeatedly lubricated with 2% viscous lidocaine throughout the procedure to maximize nasal comfort.
- •
An additional 2 mL of 2% lidocaine is sprayed via the working channel into the trachea, and 1 mL is sprayed onto the vocal folds while the patient performs a “laryngeal gargle” by producing a sustained vowel during administration of the anesthetic. This, in our experience, provides patients with adequate anesthesia for the procedure.
Other anesthetic techniques have been described for office-based airway procedures, including topical application through Abraham cannulas, transnasal red rubber catheters, or transcervical puncture, as well as bilateral superior laryngeal nerve blocks, which are reserved for anticipated long dilation times. Excessive anesthesia may lead to coughing caused by aspiration of saliva and total administration of lidocaine must not exceed the patient’s maximum allowable dose of 5 mg/kg.
Procedural approach
Tracheoscopy and Bronchoscopy
The simplest and least invasive of in-office airway procedures are diagnostic evaluations of the upper airways. They require no additional equipment or personnel beyond an endoscope and the endoscopist.
- •
Tracheoscopy may be performed without additional topical anesthesia beyond what is used for traditional flexible laryngoscopy, whereby the endoscope is passed through abducted vocal folds during quick nasal inhalation for 2 seconds while the image is captured on video, which can be played at a later time.
- •
Coughing is expected during the procedure, and the patient should be counseled of this beforehand.
- •
Additional anesthesia as described above affords a more extensive examination of the airways beyond the carina.
- •
Proximal third-order bronchi may be reached with a traditional flexible laryngoscope passed transorally.
Balloon Tracheoplasty
- •
For treating tracheal stenosis, the patient is anesthetized as previously described, and the endoscope is passed through the more patent naris to the larynx then advanced gently into the trachea.
- •
After localization of the area in need of dilation, a flexible guide wire (Hydra Jagwire Guidewire, Boston Scientific, Natick, MA) is passed through the working channel of the endoscope and advanced past the area of stenosis ( Fig. 3 ).



