Purpose
To determine the prevalence and risk factors of myopic maculopathy and specific optic disc and macular changes in highly myopic eyes of young Asian adults and their impact on visual acuity.
Design
Prospective cross-sectional study.
Methods
In total, 593 highly myopic (spherical equivalent refraction [SER] less than −6.00 diopters [D]) and 156 emmetropic (SER between −1.00 and +1.00 D) male participants from a population-based survey were included. All participants underwent standardized medical interviews, ophthalmic examination, and color fundus photographs. These photographs were graded systematically to determine the presence of optic disc and macular lesions. Myopic maculopathy was classified based on the International Classification of Myopic Maculopathy.
Results
The mean age was 21.1 ± 1.2 years. The mean SER for the highly myopic and emmetropic group was −8.87 ± 2.11 D and 0.40 ± 0.39 D, respectively ( P < .001). Compared to emmetropic eyes, highly myopic eyes were significantly more likely to have optic disc tilt, peripapillary atrophy (PPA), posterior staphyloma, chorioretinal atrophy, and myopic maculopathy (all P < .001). The main findings included PPA (98.3%), disc tilt (22.0%), posterior staphyloma (32.0%), and chorioretinal atrophy (8.3%). Myopic maculopathy was present in 8.3% of highly myopic eyes and was associated with older age (odds ratio [OR] 1.66; 95% CI: 1.22, 2.26), reduced choroidal thickness (OR 0.99; 95% CI: 0.98, 0.99), and increased axial length (AL) (OR 1.52; 95% CI: 1.06, 2.19). The presence of disc tilt, posterior staphyloma, and chorioretinal atrophy were associated with reduced visual acuity.
Conclusions
Our study showed that myopia-related changes of the optic disc and macula were common in highly myopic eyes even at a young age. The risk factors for myopic maculopathy include increased age, longer AL, and reduced choroidal thickness. Some of these changes were associated with reduced central visual function.
Myopia is a major cause of visual impairment in the world and the prevalence is especially high in East Asia. In Asia, the prevalence of myopia (spherical equivalent refraction [SER] less than −0.50 diopters [D]) and high myopia (SER less than −6.00 D) in young adults (age range 18–24 years) are 81.6%–96.5% and 6.8%–21.6%, respectively. In addition, a study in Singapore comparing similar cohorts of young Asian men (aged 16–25 years) between 1996–97 and 2009–10 showed that the prevalence of myopia and high myopia remained high in the latter group—81.6% and 14.7%, respectively. This group of young myopic adults could pose a significant public health problem in the future.
Complications associated with pathologic myopia can be irreversible and result in significant ocular morbidity. This includes myopic choroidal neovascularization, chorioretinal atrophy, and foveoschisis. These sight-threatening conditions result in reduced quality of life and increased socioeconomic burden, especially if they occur early in life. In the Singapore Cohort Study of Risk Factors for Myopia (SCORM) study (age range 12–16 years), the prevalence of optic disc tilt and peripapillary atrophy for children with SER less than −6.00 D (n = 89) was 67.5% and 92.2%, respectively. Interestingly, compared to older myopic adults (aged more than 40 years), the prevalence of these myopic maculopathies was much lower in these highly myopic children (only 1 case each of posterior staphyloma and lacquer cracks). Electrophysiology studies have also shown that the myopic retinas of adolescents and young adults have diminished amplitudes and delayed latency despite a normal-looking retina. This evidence suggested that myopia-related structural changes in the retina could be age- and time-dependent. On the other hand, in population-based studies, among adults older than 40 years with high myopia (SER less than −5.00 D), only a relatively small proportion (0.9%–3.29%) develop structural changes. It is possible that apart from axial length (AL) and SER, there are other contributing risk factors leading to pathologic myopic changes. To date, there is little literature on the visual impact of pathologic myopia and when these myopia-related changes affect highly myopic young adults. This is important in the assessment of visual potential because visual impairment at this young age group has significant impact on long-term visual prognosis and rehabilitation.
We aim to describe the prevalence of myopic maculopathy and related structural abnormalities, including specific myopia-related optic disc and macular changes in a group of highly myopic (SER less than −6.00 D) young Asian men and compare them with emmetropic eyes of the same age group. We will also examine the risk factors for these myopia-related changes and their impact on visual acuity.
Methods
Study Population
The current study was conducted between January 1, and December 31, 2012 and the methodology for subject recruitment was detailed elsewhere. Briefly, a total of 28 908 young male subjects aged 19–25 years underwent noncycloplegic autorefraction (Huvitz MRK-3100P, Republic of Korea) as part of a compulsory ophthalmic examination for pre-employment screening in Singapore. Out of 2584 persons identified to have high myopia (SER less than −6.00 D) based on noncycloplegic autorefraction, 719 subjects were selected based on refractive error–stratified random sampling strategy. They were invited to participate in the current study and underwent further examination and investigations at the Singapore Eye Research Institute as described below. For the control group, 168 emmetropic male subjects (SER between −1.00 and +1.00 D) were recruited and underwent the same standardized examination and investigations as the highly myopic group. We further excluded participants with any history of anterior segment ocular diseases, trauma, or systemic condition that affects their visual performance; any form of refractive surgery or ocular surgery that may alter the refractive status of the eye; and those who were unwilling or unable to take part in the study or unable to return for scheduled visits. Written informed consent were taken from the subjects and their parents/guardians (if they were below 21 years of age). The study was conducted in accordance with the tenets of the World Medical Association’s Declaration of Helsinki and had ethics approval from the Singhealth Centralized Institutional Review Board.
Interview, Visual Acuity Measurement, and Refraction
All the participants who fulfill the inclusion criteria and consented to the study underwent a standardized interview regarding their refraction status, including the age at which they started wearing glasses and the age at which their spherical refractive error first reached −6.00 D. Best-corrected visual acuity (BCVA) measurement and subjective cycloplegic refraction were conducted on the same day by a trained optometrist. The subjects’ monocular VA was measured using the logarithm of the minimal angle of resolution (logMAR) chart (Lighthouse International, New York, New York, USA) at 4 meters. If the largest number could not be identified at 4 meters, the chart was brought closer to the subject, then counting fingers, hand motion, or light perception vision was assessed. Cycloplegia was induced with 3 drops of cyclopentolate 1% 5 minutes apart. At least 30 minutes after the last drop, subjective cycloplegic refraction tests were performed by the same optometrist for all the participants. SER was calculated as the sum of the spherical power and half of the cylindrical power.
Ocular Examination and Imaging
Ocular biometry was performed using the IOL Master (Carl Zeiss Meditec AG, Jena, Germany), which included AL measurements. The mean of 3 AL measurements was taken as the final AL. All the subjects underwent a standardized and detailed examination of the anterior segment at the Singapore Eye Research Institute by a trained ophthalmologist. Slit-lamp examination included assessment of cornea and lenticular pathology and anterior chamber depth. Goldmann applanation tonometry was used to measure the intraocular pressure in mm Hg. Retinal photography was performed by a trained ophthalmic technician using the Canon CR-DGI (Canon Inc, Tokyo, Japan) nonmydriatic retinal camera after pupil dilation. Seven retinal photographs were taken to obtain the view of the optic disc (disc-centered and rotated at 30 degrees to the right and 30 degrees to the left), macular view, and right and left upper and lower arcade peripheral views from both eyes. Spectral-domain optical coherence tomography (SD OCT; Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany) of the macula was also performed after pupil dilation. The SD OCT scans were centered over the macula (scan diameter of 20 degrees) and used to evaluate the posterior pole for subtle posterior staphyloma and choroidal thickness. The details for choroidal thickness measurement were already described elsewhere and showed good reproducibility.
Fundus Photograph Grading
The color fundus photographs were graded similar to previously established grading techniques by a single trained grader (V.Y.) masked to the participant characteristics. Adjudication was performed by an experienced medical retina specialist (C.T.) from an accredited fundus photograph grading center.
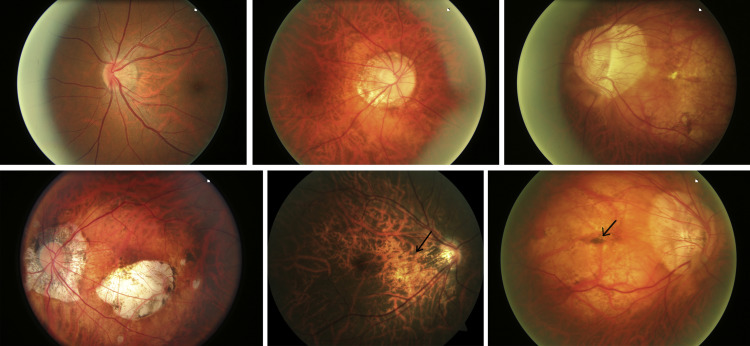
The main findings that were graded included (1) optic disc morphology (optic disc tilt and peripapillary atrophy) and (2) myopia-related macular pathology, including staphyloma, lacquer crack, and peripapillary atrophy (PPA) ( Figure 1 ). Optic disc tilt was diagnosed when 1 margin of the optic disc was subjectively raised above the opposite margin and the direction of optic disc tilt was determined. Presence of lacquer crack, its location, and number were evaluated. The Curtin and Karlin classification was used to determine the subtype and position of PPA. Staphyloma was determined by visualizing the border of the ectasia, then its location and type were documented based on the Curtin classification. Intergrader reliability in grading for the aforementioned features was assessed with additional grading of 100 randomly selected eyes by trained graders (V.Y. and V.K.), and reliability was found to be good (all intraclass correlation coefficients above 0.75). However, more subtle posterior staphyloma may be missed from fundus photographs. As such, after the initial screening for posterior staphyloma on fundus photographs, we further analyzed the remaining eyes using cross-sectional images from SD OCT to detect shallower posterior staphyloma. All the SD OCT images were graded by a medical retinal specialist (C.T.). The presence of posterior staphyloma was defined as curvature of the retinal pigment epithelium layer, with a foveal depth of ≥500 μm relative to the periphery of the OCT B-scan. This allowed posterior staphyloma with more gentle and subtle sloping edges to be detected.
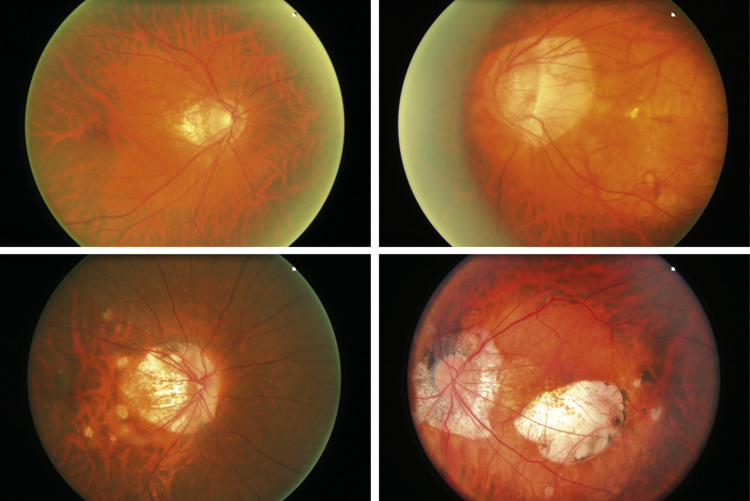
The presence of myopic maculopathy was defined and classified based on the International Photographic Classification and Grading System for Myopic Maculopathy. Briefly, pathologic myopia was classified in order of increasing severity ( Figure 2 ): category 0, no macular lesions; category 1, only tessellated fundus; category 2, diffuse chorioretinal atrophy; category 3, patchy chorioretinal atrophy; and category 4, macular atrophy. In addition, “plus” lesions included lacquer cracks, choroidal neovascularization, and Fuchs spot. Posterior staphyloma was classified as supplemental information. For this study, the presence of myopic maculopathy is defined as findings in the fundus photograph consistent with category 2 and above.
Statistical Analysis
Statistical analysis was performed using IBM SPSS version 22 (IBM Corporation, New York, USA). Only 1 eye per subject was included for analysis. By default, the right eye is selected unless the SER of the right eye is more than −6.00 D for the myopic group, then the left eye is selected for analysis. The χ 2 test or Fisher exact test was used for comparing categorical variables between highly myopic eyes and emmetropic eyes, and Student t test was performed for continuous variables. Logistic regression was performed to determine the association with myopic maculopathy and its trend across SER and AL categories. Linear regression models adjusted for age and ethnicity were performed to determine the effect of optic disc tilt, PPA, posterior staphyloma, chorioretinal atrophy, and myopic maculopathy on BCVA. Statistical significance was set at P < .05.
Results
Out of a total of 887 participants who were initially recruited for the study, we excluded 51 persons who did not meet the inclusion criteria and 87 persons whose final subjective cycloplegic refraction results did not fulfill either the high myopia (SER less than −6.00 D) or emmetropia (SER between −1.00 and +1.00 D) criteria. For our final analyses, we included 593 and 156 participants into the high myopia and emmetropic group, respectively. All the subjects were male and the mean age was 21.1 ± 1.2 (standard deviation [SD]) years for the myopic group and 21.5 ± 1.1 years (SD) for the emmetropic group ( P = .09). The mean SER for the myopic and emmetropic group was −8.87 ± 2.11 D and 0.40 ± 0.39 D, respectively ( P < .001). The corresponding AL was 27.45 ± 1.17 mm and 23.83 ± 1.01 mm, respectively ( P < .001).
Table 1 shows the common myopia-related optic disc and macular changes in highly myopic and emmetropic eyes and their relationship with SER. Compared to emmetropic eyes, the highly myopic eyes were significantly more likely to be affected by optic disc tilt, PPA, posterior staphyloma, and chorioretinal atrophy (all P < .001). For optic disc tilt, the most common direction of tilt was temporal (125/168; 74.4%) and for PPA, the most common location was temporal (434/655; 66.2%). Lacquer cracks were uncommon (6/593; 1.0%) and there was no significant difference in the presence of lacquer cracks between myopic eyes and emmetropic eyes ( P = .608). The lacquer cracks detected in all 6 myopic eyes were located in the macular region without involvement of the fovea. The most common type of staphyloma was peripapillary (103/155; 66.5%). For myopic eyes with chorioretinal atrophy, 72.5% (37/51 eyes) were smaller than 1 disc diameter in size. Most of the chorioretinal atrophy was also found in the peripapillary region (40/49; 81.6%). The prevalence of more visually adverse myopia-related changes such as macular hemorrhages, choroidal neovascularization, and Fuchs spots (2/593; 0.34%) were low in the myopic group. Myopic maculopathy was present in 8.3% (49/593) of the eyes in the myopic group.
| All Subjects (n = 749) | Optic Disc Tilt | Peripapillary Atrophy | Posterior Staphyloma | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | n (%) | P Value | N | n (%) | P Value | N | n (%) | P Value | |
| Emmetropic (−0.75D to +1.00 D) | 151 | 2 (1.3) | <.001 | 155 | 76 (49.0) | <.001 | 136 | 1 (0.66) | <.001 |
| With high myopia (−23.50 to −6.13 D) | 574 | 126 (22.0) | 589 | 579 (98.3) | 485 | 155 (32.0) | |||
| All Subjects (n = 749) | Chorioretinal Atrophy | Myopic Maculopathy Category (N = 749) | Presence of Myopic Maculopathy a (Yes vs No) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 0–1 | 2 | 3 | 4 | P Value | |||||||
| N | n (%) | P Value | n (%) | n (%) | n (%) | n (%) | N | n (%) | P Value | |||
| Emmetropic (−0.63 to +1.50 D) | 156 | 1 (0.6) | .001 | 156 | 155 (99.4) | 1 (0.6) | 0 (0.0) | 0 (0.0) | .01 | 156 | 1 (0.6) | <.001 |
| With high myopia (−23.50 to −6.13 D) | 590 | 49 (8.3) | 593 | 544 (91.7) | 31 (5.2) | 11 (1.9) | 7 (1.2) | 593 | 49 (8.3) | |||
a Presence of myopic maculopathy defined as findings in the fundus photograph consistent with category 2 and above based on the International Classification of Myopic Maculopathy.
Table 2 shows that with decreasing SER, there is a significantly increased frequency of myopia-related optic disc and macular changes in the eyes with high myopia (all P < .001) except peripapillary atrophy ( P = .06). Increased AL was also significantly associated with increased frequency of chorioretinal atrophy and posterior staphyloma, and similar trends for the other structural changes, although these did not reach statistical significance. The proportions of the more severe categories of myopic maculopathy (category 3 and 4) were significantly higher with decreased SER. Overall, the proportion of eyes with myopic maculopathy was significantly higher with decreased SER or increased AL.
| Optic Disc Tilt | Peripapillary Atrophy | Posterior Staphyloma | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | n (%) | P Value | N | n (%) | P Value | N | n (%) | P Value | |
| Spherical equivalent | |||||||||
| <−6.00 to −8.00 D | 238 | 35 (14.7) | <.001 | 246 | 239 (97.2) | .06 | 210 | 52 (24.8) | <.001 |
| <−8.00 to −10.00 D | 197 | 46 (23.4) | 202 | 202 (100.0) | 169 | 49 (29.0) | |||
| <−10.00 D | 139 | 45 (32.4) | 141 | 138 (97.9) | 106 | 54 (50.9) | |||
| Axial length | |||||||||
| All | 574 | 126 (22.0) | 589 | 579 (98.3) | 485 | 155 (32.0) | |||
| 1st quartile (24.07–25.72 mm) | 31 | 6 (19.4) | .45 | 33 | 31 (93.9) | .09 | 31 | 3 (9.7) | <.001 |
| 2nd quartile (25.74–26.85 mm) | 147 | 26 (17.7) | 152 | 148 (97.4) | 129 | 29 (22.5) | |||
| 3rd quartile (mm) (26.87–27.80 mm) | 194 | 44 (22.7) | 197 | 194 (98.5) | 162 | 47 (29.0) | |||
| 4th quartile (27.81–33.02 mm) | 202 | 50 (24.8) | 207 | 206 (99.5) | 163 | 76 (46.6) | |||
| Chorioretinal Atrophy | Myopic Maculopathy Category | Presence of Myopic Maculopathy (Yes vs No) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 0–1 | 2 | 3 | 4 | |||||||
| N | n (%) | P Value | n (%) | n (%) | n (%) | n (%) | N | n (%) | P Value | ||
| Spherical equivalent | |||||||||||
| <−6.00 to −8.00 D | 246 | 12 (4.9) | <.001 | 248 | 236 (95.2) | 12 (4.8) | 0 (0.0) | 0 (0.0) | 248 | 12 (4.8) | P < 0.001 |
| <−8.00 to −10.00 D | 203 | 11 (5.4) | 204 | 193 (94.6) | 7 (3.4) | 2 (1.0) | 2 (1.0) | 204 | 11 (5.4) | ||
| <−10.00 D | 141 | 26 (18.4) | 141 | 115 (81.6) | 12 (8.5) | 9 (6.4) | 5 (3.5) | 141 | 26 (18.4) | ||
| P value for myopic maculopathy category | Reference | P = .10 | P < .001 | P < .001 | |||||||
| Axial length | |||||||||||
| All | 590 | 49 (8.3) | 593 | 544 (91.7) | 31 (5.2) | 11 (1.9) | 7 (1.2) | 593 | 49 (8.3) | ||
| 1st quartile (24.07–25.72 mm) | 33 | 1 (3.0) | <.001 | 34 | 33 (97.1) | 1 (2.9) | 0 (0.0) | 0 (0.0) | 34 | 1 (2.9) | <.001 |
| 2nd quartile (25.74–26.85 mm) | 152 | 6 (3.9) | 153 | 147 (96.1) | 4 (2.6) | 1 (0.7) | 1 (0.7) | 153 | 6 (3.9) | ||
| 3rd quartile (26.87–27.80 mm) | 197 | 9 (4.6) | 198 | 189 (95.5) | 6 (3.0) | 2 (1.0) | 1 (0.5) | 198 | 9 (4.5) | ||
| 4th quartile (27.81–33.02 mm) | 208 | 33 (15.9) | 208 | 175 (84.1) | 20 (9.6) | 8 (3.8) | 5 (2.4) | 208 | 33 (15.9) | ||
| P value for myopic maculopathy category | Reference | P = .003 | P = .02 | P = .09 | |||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


