Purpose
To identify clinical outcomes and treatment patterns of intravitreal dexamethasone implant (Ozurdex; Allergan, Inc) in noninfectious uveitis in the clinical setting.
Design
Multicenter retrospective cohort study.
Methods
Eighty-two eyes (63 patients) receiving 142 implant injections over 35 months were included. Treatment indication, uveitis diagnosis, visual acuity, intraocular pressure, vitreous haze score, central retinal thickness by optical coherence tomography, phakic status, number of injections, time to reinjection, systemic treatments, and complications data were collected. Time to visual acuity and vitreous haze score improvement as per the Standardization of Uveitis Nomenclature guidelines were also determined.
Results
The probability of visual acuity improvement (≥0.3 logarithm of the minimal angle of resolution units improvement) was 39% at 1 month, 49% at 3 months, 52% at 6 months, and 58% at 12 months. Eyes with baseline vitritis (vitreous haze score ≥+0.5, n = 45) had a probability of vitreous haze score improvement (2-step decrease or change from +0.5 to 0) at 2 weeks of 41%, at 1 month 63%, at 3 months 73%, at 6 months 79%, and at 12 months 88%. In eyes that completed 12-month follow-up (n = 54), 40.7% underwent 2 injections (mean time to second injection of 6.6 ± 1.9 months) and 11.2% required ≥3 injections (mean time to third injection of 11 ± 1.5 months).
Conclusions
Dexamethasone implant use in uveitis provides favorable visual acuity and vitreous haze score outcomes but requires repeated injections, an important consideration when choosing intraocular treatment as a route to controlling uveitis.
As uncontrolled intraocular inflammation results in cumulative damage to the retina, there is consensus that long-term maintained control of uveitis is critical for preserving vision. Sustained-release intraocular implants have been developed in recent years to provide maintained delivery of different types of steroids to the posterior segment. Whereas some of the first steroid implants required a major surgical procedure for their placement in the vitreous cavity, the technological advances in pharmacotherapy have made possible the development of new injectable devices that can be easily administered in an office-based setting. Currently commercially available devices are classified into 2 types: inert shells, which slowly release drug; and bioerodible polymers. Among the latter is included the dexamethasone implant (Ozurdex; Allergan, Inc, Irvine, California, USA), which is a bioerodible device composed of a mix of polylactic acid and polyglycolic acid polymers that releases 0.7 mg of preservative-free dexamethasone for up to 6 months. Its safety and efficacy has been confirmed in clinical trials for the management of a variety of retinal diseases, such as macular edema related to retinal vein occlusions or diabetes.
The use of the dexamethasone implant for uveitis was evaluated in the HURON (cHronic Uveitis evaluation of the intRavitreal dexamethasONe implant) trial. This study demonstrated that a single injection led to adequate control of intraocular inflammation and good visual outcomes for up to 6 months in noninfectious intermediate and posterior uveitis. However, given the strict entry criteria under trial conditions, it is unclear whether these outcomes reflect the routine use of this implant in uveitis units in real-world situations, in which treatment is driven by wider indications, for longer follow-up periods, when repeat injections are required. The criteria for determining intraocular steroid treatment in uveitis have yet to reach consensus on where it sits in the pathway of care outside the clinical trial setting; therefore, larger study cohort outcomes have the opportunity to inform this consensus over and above the short single-center series currently reported.
With this in mind, we established a collaborative project between 4 specialized uveitis units in the United Kingdom and Spain to ascertain the clinical characteristics, demographics, and clinical outcomes, as well as complications and reinjection frequency, of intravitreal dexamethasone implant in noninfectious uveitis in routine clinical practice.
Methods
Clinical data were retrospectively collected from 4 specialized uveitis clinics, 2 in the United Kingdom (Bristol Eye Hospital, University Hospitals Bristol National Health Service Foundation Trust, Bristol; and Gloucestershire Hospitals National Health Service Foundation Trust, Cheltenham) and 2 in Spain (Hospital Universitario de Cruces, Bilbao; and Institut Clínic d′Oftalmología [ICOF] at Hospital Clinic, Barcelona). A comprehensive data spreadsheet was provided to each study center and was completed within the predetermined timeframe by the end of August 2013, collecting data from injections performed between October 26, 2010 and July 4, 2013. Patient identifiers were removed to make data anonymous, and on this basis an ethics committee at Gloucestershire Hospitals National Health Service Foundation Trust determined that formal ethics approval was not required. Data from individual centers were collated and merged to a centralized database for analysis purposes. This study was conducted in accordance with the tenets of the Declaration of Helsinki. Analysis was restricted to eyes undergoing intravitreal dexamethasone implant injection for noninfectious uveitis, with clinical indications of vitritis or uveitic cystoid macular edema (CME) or both.
Clinical Data
Data collected included age; sex; laterality; indication; uveitis anatomic classification; phenotypic diagnosis; previous local treatments; previous and current systemic treatments; surgical details; number of injections; complications; and visual acuity (VA), intraocular pressure (IOP), central retinal thickness assessed by optical coherence tomography (OCT), and vitreous haze score at baseline and at 1, 3, 6, and 12 months post injection of the first intravitreal dexamethasone implant.
Data Sources/Measurements
As data were gathered from routine clinical settings, visual acuity was determined as the best VA with habitual correction or pinhole rather than best-corrected refracted VA at all time points. Analysis for eyes with low VA was undertaken by substituting counting fingers and hand movement with 2.0 and 2.3 logarithm of the minimal angle of resolution (logMAR), respectively. Vitreous haze score was measured using a standardized scale in conformance with Standardization of Uveitis Nomenclature guidelines. Central retinal thickness was determined by OCT imaging, using 1 of 2 different devices depending on the study center (Cirrus HD OCT; Carl Zeiss Meditec, Dublin, California, USA and Spectralis OCT; Heidelberg Engineering, Heidelberg, Germany). In patients for whom data were not available for a particular visit or who had been lost to follow-up, no missing value substitutions were performed.
Statistical Methods
Probabilities of events occurring after intravitreal dexamethasone implant injection are presented as survival curves using the Kaplan-Meier method. Snellen VA was converted to logMAR equivalents for the purposes of statistical analysis. Improvement in VA and vitreous haze score was defined as per the Standardization of Uveitis Nomenclature guidelines as halving of the visual angle (≥0.3 logMAR unit change) and 2-step decrease or change from +0.5 to 0 in vitreous haze score, respectively. Subgroup analysis was performed in eyes with vitritis and eyes with CME. Descriptive frequency statistics and the χ 2 test were used to assess qualitative variables. Normality of quantitative variables was examined using histograms. The paired t test was used to compare pre- and posttreatment mean changes when variables were normally distributed, and the Wilcoxon test was used in cases where nonparametric tests were required. A P value of less than .05 was considered statistically significant. All statistical analysis was performed using Excel and SPSS 15.0 software (SPSS Inc, Chicago, Illinois, USA). Kaplan-Meier survival analysis curves were constructed using MedCalc 13.3 software (MedCalc Software, Ostend, Belgium).
Results
Demographics, Indications, and Uveitis Type of Study Eyes
Data were received for 146 intravitreal dexamethasone implant injections performed in 85 eyes over a 35-month period (October 2010–August 2013) ( Supplemental Figure 1 , available at AJO.com ). Three of these eyes were excluded from analysis owing to different indications than noninfectious uveitis (1 eye had hypotonous maculopathy, 1 had CME following a previously treated toxoplasma chorioretinitis, 1 had CME following penetrating eye injury). A total of 142 intravitreal dexamethasone implant injections performed in 82 eyes of 63 patients with noninfectious uveitis were analyzed, with 30.1% of patients receiving bilateral injections (19/63). Patient demographics, indications, uveitis anatomic classification, phenotypic diagnosis, and current and previous treatments of study eyes are detailed in Table 1 . The most common indication for treatment was CME (60.9%, 50/82), followed by vitritis (25.6%, 23/82), then combined CME and vitritis (10.9%, 9/82). The most frequent anatomic locations were intermediate uveitis (37.8%, 31/82), posterior uveitis (23.1%, 19/82), and panuveitis (21.9%, 18/82), and most frequent phenotypic diagnoses were nondifferentiated (54.8%, 45/82), birdshot chorioretinopathy (14.6%, 12/82), sarcoidosis (7.3%, 6/82), and multiple sclerosis (7.3%, 6/82). The mean time from diagnosis to the first injection was 67.8 ± 65.2 months (median = 48 months, interquartile range 49). Excluding patients with juvenile idiopathic arthritis (as they are commonly diagnosed in childhood with prolonged follow-up), the mean time from diagnosis to first injection was 58.4 ± 51.6 months (median = 48, IQR = 51.5).
| Total | Bristol Eye Hospital, Bristol, UK | Gloucestershire NHS Trust, Cheltenham, UK | Hospital de Cruces, Bilbao, Spain | Hospital Clinic, Barcelona, Spain | |
|---|---|---|---|---|---|
| Age, mean ± SD (median, IQR) | 47.4 ± 17.2 (50.5, IQR 26) | 51.2 ± 15.7 (53, IQR 22) | 40 ± 16.9 (37, IQR 28) | 47.9 ± 21.6 (52, IQR 29.5) | 48.2 ± 16.1 (48, IQR 24.5) |
| Sex, % female (female:male) | 74.1% (2.8:1) | 60% (1.5:1) | 100% (9:0) | 75% (3:1) | 71.8% (2.5:1) |
| N eyes (patients) | 82 (63) | 15 (10) | 10 (9) | 15 (12) | 42 (32) |
| Indications (%) | 1. CME (61%) 2. Vitritis (28%) 3. CME + vitritis (11%) | 1. CME (66.7%) 2. Vitritis (20%) 3. CME + vitritis (13.3%) | 1. Vitritis (40%) 2. CME + vitritis (40%) 3. CME (20%) | 1. CME (80%) 2. CME + vitritis (13.4%) 3. Vitritis (6.6%) | 1. CME (61.9%) 2. Vitritis (35.7%) 3. CME + vitritis (2.4%) |
| Uveitis anatomic classification (%) | 1. Intermediate uveitis (37.8%) 2. Posterior uveitis (23.1%) 3. Panuveitis (21.9%) 4. Anterior chronic uveitis (13.4%) 5. Acute anterior uveitis (2.4%) 6. Retinal vasculitis (1.2%) | 1. Intermediate uveitis (46.6%) 2. Posterior uveitis (40%) 3. Panuveitis (13.3%) | 1. Intermediate uveitis (70%) 2. Panuveitis (30%) | 1. Anterior chronic uveitis (46.7%) 2. Panuveitis (13.3%) 3. Intermediate uveitis (20%) 4. Intermediate uveitis (20%) | 1. Intermediate uveitis (33.3%) 2. Panuveitis (26.2%) 3. Posterior uveitis (23.8%) 4. Anterior chronic uveitis (9.5%) 5. Acute anterior uveitis (4.7%) 6. Retinal vasculitis (2.3%) |
| Phenotypic diagnosis (%) | 1. Nondifferentiated (54.8%) 2. Birdshot (14.6%) 3. Sarcoidosis (7.3%) 4. Multiple sclerosis (7.3%) 5. Juvenile arthritis (6.1%) 6. Ankylosing spondylitis (2.4%) 7. HLA-B27 uveitis (2.4%) 8. IRVAN (2.4%) 9. Sympathetic ophthalmia (1.2%) 10. Behçet disease (1.2%) | 1. Nondifferentiated (60.0%) 2. Birdshot (26.6%) 3. HLA-B27 uveitis (13.3%) | 1. Nondifferentiated (90%) 2. Juvenile arthritis (10%) | 1. Nondifferentiated (66.6%) 2. Sarcoidosis (20%) 3. Juvenile arthritis (6.7%) 4. Birdshot (6.7%) | 1. Nondifferentiated (40.4%) 2. Birdshot (16.6%) 3. Multiple sclerosis (14.3%) 4. Sarcoidosis (7.1%) 5. Juvenile arthritis (7.1%) 6. Ankylosing spondylitis (4.7%) 7. IRVAN (4.7%) 8. Sympathetic ophthalmia (2.3%) 9. Behçet disease (2.3%) |
| Systemic therapies ( % ) | 53.9% (34/63) | 50% | 44.4% | 58.3% | 56.2% |
| -Prednisolone | 14.3% | 20% | 22.2% | 8.3% | 12.5% |
| -1 second-line agent | 9.5% | 0% | 0% | 8.3% | 15.6% |
| -2 double therapy a | 20.6% | 20% | 22.2% | 41.7% | 18.7% |
| -3 Triple therapy b | 9.5% | 10% | 0% | 0% | 9.4% |
| Immunomodulatory therapy (%) | 1. MTX (31%) 2. Adalimumab (20.6%) 3.Mycophenolate (20.6%) 4. Cyclosporine (6.9%) 5. Tacrolimus (6.9%) 6. Azathioprine (3.4%) 7. Beta-interferon (3.4%) 8. Abatacept (3.4%) 9. Golimumab (3.4%) | 1.Mycophenolate (50%) 2. Adalimumab (25%) 3. Tacrolimus (25%) | 1.Mycophenolate (100%) | 1. MTX (71.4%) 2. Adalimumab (28.6%) | 1. Adalimumab (29.4%) 2. MTX (23.5%) 3.Mycophenolate (11.7%) 4. Cyclosporine (11.7%) 5. Azathioprine (5.8%) 6. Beta-interferon (5.8%) 7. Abatacept (5.8%) 8. Golimumab (5.8%) |
| Previous local therapies ( % ) | 63.4% (52/82) | 60% (9/15) | 90% (9/10) | 60% (9/15) | 59.5% (25/42) |
| -Periocular steroids | 37.8% (31/82) | 6.6% (1/15) | 50% (5/10) | 40% (6/15) | 45.2% (19/42) |
| -Intravitreal steroids | 56% (46/82) | 60% (9/15) | 70% (7/10) | 26.6% (4/15) | 61.9% (26/42) |
| -Anti-VEGF | 19.5% (16/82) | 13.3% (2/15) | 0% (0/10) | 20% (3/15) | 26.1% (11/42) |
a Double therapy: steroids + second-line agent.
Current Systemic Treatment, Previous Local Treatments, and Phakic Status
At the time of the first injection, 53.9% of patients (34/63) were on systemic treatment, which included 14.3% (9/63) on prednisolone, 9.5% (6/63) on 1 second-line immunomodulatory therapy, and 30.1% (19/63) on a combined regimen of prednisolone and immunomodulatory therapy as dual therapy in 20.6% (13/63) and as triple therapy in 9.5% (6/63) ( Table 1 ). Previous local treatments with periocular and intravitreal therapies were used in 63.4% of eyes (52/82), with 37.8% treated with prior periocular steroids (31/82), 56.0% with intravitreal triamcinolone (46/82), and 19.5% with intravitreal anti–vascular endothelial growth factor (VEGF) drugs (16/82). Regarding the phakic status, 51.2% of the eyes were pseudophakic (42/82), 42.6% were phakic (35/82), and 6.1% were aphakic (5/82). Previous pars plana vitrectomy had been undertaken in 32.9% of included eyes (27/82) to facilitate uveitis control.
Visual Acuity, Vitreous Haze, and Central Retinal Thickness Outcomes
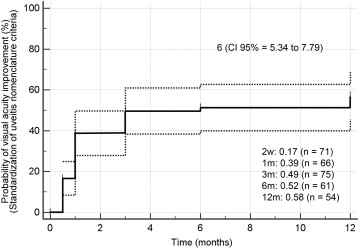
VA (mean ± standard deviation [SD]) was 0.68 ± 0.4 (median = 0.5) logMAR at baseline, 0.59 ± 0.4 (0.5) 2 weeks post injection, 0.49 ± 0.4 (0.4) at 1 month, 0.49 ± 0.5 (0.4) at 3 months, 0.60 ± 0.5 (0.4) at 6 months, and 0.52 ± 0.5 (0.4) at 12 months ( P < .01 at all time points) ( Table 2 ). The probability of visual acuity improvement as per the Standardization of Uveitis Nomenclature guidelines (improvement ≥0.3 logMAR units) was 17% at 2 weeks, 39% at 1 month, 49% at 3 months, and 52% at 6 months, which was maintained at 12 months (58%) ( Figure 1 ). The median time to visual acuity improvement was 6 months (95% confidence interval [CI] = 5.34–7.79).
| All Study Eyes | Baseline | 2 Weeks | 1 Month | 3 Months | 6 Months | 12 Months |
|---|---|---|---|---|---|---|
| VA, logMAR | ||||||
| Mean ± SD (median, IQR) | 0.68 ± 0.47 (0.5, IQR 0.4) | 0.59 ± 0.49 (0.5, IQR 0.6) | 0.49 ± 0.47 (0.4, IQR 0.4) | 0.49 ± 0.50 (0.4, IQR 0.6) | 0.60 ± 0.5 (0.4, IQR 0.4) | 0.52 ± 0.53 (0.4, IQR 0.575) |
| IOP, mm Hg | ||||||
| Mean ± SD (median, IQR) | 14.1 ± 4.0 (14, IQR 5) | 18.0 ± 8.1 (17, IQR 5.75) | 18.0 ± 7.6 (17, IQR 7.25) | 15.9 ± 5.4 (16, IQR 5) | 14.3 ± 4.2 (14, IQR 5.5) | 14.6 ± 4.2 (15, IQR 6) |
| VHS | ||||||
| 0 | 37 (48.6%) a | 47 (68.1%) | 55 (85.9%) | 52 (74.2%) | 43 (72.8%) | 42 (79.2%) |
| +0.5 | 9 (11.8%) | 10 (14.4%) | 5 (7.8%) | 9 (12.8%) | 8 (13.5%) | 5 (9.4%) |
| +1 | 18 (23.6%) | 9 (13%) | 3 (4.6%) | 5 (7.1%) | 4 (6.7%) | 5 (9.4%) |
| +2 | 9 (11.8%) | 3 (4.3%) | 1 (1.5%) | 3 (4.2%) | 3 (5%) | 0 (0%) |
| +3 | 2 (2.6%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| +4 | 1 (1.3%) | 0 (0%) | 0 (0%) | 1 (1.4%) | 1 (1.6%) | 1 (1.8%) |
| CRT, μm | ||||||
| Mean ± SD (median, IQR) | 462 ± 190 (436, IQR 245) | 327 ± 97 (312, IQR 124) | 274 ± 89 (260, IQR 76) | 324 ± 150 (278, IQR 87) | 366 ± 158 (311, IQR 173) | 335 ± 153 (277, IQR 145) |
| (Total n = 82) | (n = 80) | (n = 71) | (n = 66) | (n = 75) | (n = 61) | (n = 54) |
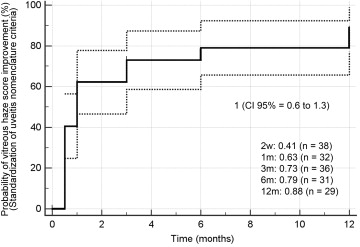
Restricting the analysis to include only eyes with vitritis at baseline (vitreous haze score ≥+0.5, n = 39 eyes), the probability of achieving vitreous haze score improvement as per the Standardization of Uveitis Nomenclature guidelines (2-step improvement or change from +0.5 to 0) was 41% at 2 weeks, 63% at 1 month, 73% at 3 months, 79% at 6 months, and 88% at 12 months ( Figure 2 ). The median time to vitreous haze score improvement was 1 month (95% CI = 0.6–1.3).
In the cohort of eyes with CME (n = 59 eyes), the mean central retinal thickness was 469 ± 193 μm (mean ± SD) at baseline, improving to 326 ± 81 at 2 weeks, 267 ± 74 at 1 month, 318 ± 149 at 3 months, 366 ± 140 at 6 months, and 355 ± 160 at 12 months ( P < .001 at all time points) ( Supplemental Table 1 , available at AJO.com ). These results, together with corresponding visual acuity measures at each time point, are shown in Supplemental Figure 2 (available at AJO.com ).
Intraocular Pressure Outcomes
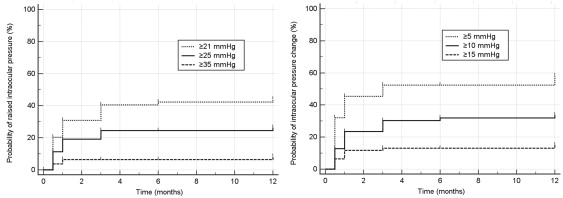
Mean IOP at baseline was 14.1 ± 4 mm Hg (mean ± SD) and increased to 18.0 ± 8 mm Hg at 2 weeks ( P < .001), 18.0 ± 7 mm Hg at 1 month ( P < .001), 15.9 ± 5 mm Hg at 3 months ( P = .01), 14.4 ± 4 mm Hg at 6 months ( P = .62), and 14.6 ± 4 mm Hg at 12 months ( P = .43) ( Table 2 ). At 1 month, the probability of having an IOP ≥21 mm Hg was 32%, ≥25 mm Hg was 19%, and ≥35 mm Hg was 7%, and at 3 months these probabilities were 41%, 23%, and 7%, respectively ( Figure 3 , Left). Regarding changes in IOP from baseline, at 1 month the probability of IOP increase ≥5 mm Hg was 46%, ≥10 mm Hg was 23%, and ≥15 mm Hg was 12%. These probabilities increased to 53%, 30%, and 13% at 3 months, respectively ( Figure 3 , Right).
Reinjection Frequency and Number of Injections
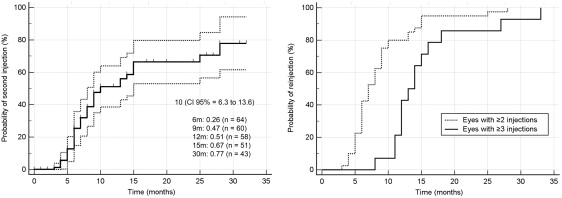
The overall mean number of injections was 1.7 ± 0.8 (mean ± SD) with a median of 1 injection over a mean follow-up of 15.4 ± 9 months (median = 13). A single injection was performed in 52.4% (43/82) of eyes, 29.3% (24/82) required 2 injections, and 18.2% (15/82) required ≥3 injections. The probability of having a second injection at 6 months was 26%, increasing to 47% at 9 months and 51% at 12 months, with a median time to second injection of 10 months (95% CI = 6.3–13.6) ( Figure 4 , Left). Among eyes that were injected twice, the probability of having the second injection by 6 months was 43%, and among those with ≥3 injections the probability of having the third injection by 12 months was 43% ( Figure 4 , Right).
Restricting the analysis to eyes that completed 12 months of follow-up (54/82 eyes, 65.9%; 28 eyes [34.1%] did not complete 12 months of follow-up), the mean number of injections was 1.64 ± 0.7 (median = 2) ( Supplemental Table 2 , available at AJO.com ). In this subgroup, 40.7% (22/54) of eyes required a second injection, which was performed on average 6.6 ± 1.9 months after the first injection (median = 6); and in the 9.3% (5/54) of eyes that required a third injection, this was done on average 11.0 ± 1.5 months (median = 11.5) after the first implant ( Supplemental Figure 3 , available at AJO.com ). Only 1 eye required a fourth injection within 12 months (1.9%). For patients who completed 12 months of follow-up, no significant differences were observed between eyes treated for vitritis or uveitic CME in the mean number of injections (1.76 ± 0.7 vs 1.65 ± 0.7, P = .54), percentage of eyes requiring 2 injections (53.5% vs 39.0%, P = .19), or mean time to second injection (6.73 vs 6.71 months, P = .97). Among eyes with CME, a trend was observed for higher mean number of injections when concomitant vitritis was present (2.14 vs 1.56, P = .06), without significant differences in mean visual acuity (0.50 ± 0.6 logMAR vs 0.55 ± 0.5 logMAR, P = .81) or mean central retinal thickness (229 ± 29 μm vs 272 ± 76 μm, P = .23) at month 1, or at month 12 (0.51 ± 0.5 logMAR vs 0.72 ± 0.6 logMAR, P = .36; and 343 ± 147 μm vs 418.8 ± 222 μm, P = .30, respectively).
Systemic Treatment
The probability of dose reduction, defined as reduction in ≥5 mg of prednisolone or any decrease in second-line immunomodulatory therapy dose for patients on systemic treatment at baseline (n = 34, 53.9%), was 36% at 1 month, increasing to 42% at 3 months and 46% at 6 months, and peaking at 62% at 12 months ( Supplemental Figure 4 , available at AJO.com ). Standardization of Uveitis Nomenclature criteria definition for dose reduction (oral prednisolone <10 mg/day) was not possible to apply in our series as only 22% of patients (12/63) were on high-dose maintenance steroids (prednisolone ≥10 mg) at baseline. The probability of systemic steroid discontinuation was 8% at 1 and 3 months, increasing to 11% at 6 months and 36% at 12 months.
Adverse Effects and Complications
The most frequent adverse effect was raised IOP (≥21 mm Hg) in 40.2% of the eyes (33/82), requiring ocular hypotensive treatment in 39% (32/82) and glaucoma surgery in 2.4% of study eyes (2/82). The percentage of pseudophakic patients increased from 51.2% (42/82) at baseline to 56.1% (46/82) at final follow-up. Among the 142 injections there were 3 cases of vitreous hemorrhage (2.1%, 3/142), 3 cases of hypotony (2 in vitrectomized eyes) (2.1%, 3/142), 2 cases of implant dislocation into the anterior chamber (1 in aphakic eyes, 1 in pseudophakic eyes with iris-claw intraocular lens) (1.4%, 2/142), and 1 case of endophthalmitis (0.7%, 1/142). No cases of retinal detachment were observed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


