A variety of mucoactive medications are used to treat chronic lung disease. When evaluating the role of the cough, it must be considered as an important protective mechanism. Therefore, it may be more important to improve the effectiveness of cough than to suppress or eliminate a chronic cough in patients with chronic lung disease. This article discusses the composition of mucus and phlegm, the process of mucin secretion and mucus clearance, and reviews current therapy and mucolytics in use or being studied for mucus clearance disorders.
Normal airway mucus lines epithelial surfaces that are potentially exposed to the outside environment. Mucins and mucus can detoxify noxious or reactive aerosols, decrease ambient water loss for the epithelia, and capture and clear inhaled pathogens and particles. The normal mucin network may also inhibit bacterial biofilm formation. The major macromolecular constituents of normal mucus are the secreted gel-forming mucin glycoproteins. Phlegm production is a hallmark of chronic inflammatory airway diseases such as bronchiectasis, chronic bronchitis, and cystic fibrosis. When expectorated, phlegm is called sputum. Sputum has altered macromolecular and polymer composition and biophysical properties, which vary with disease. Mucin glycoprotein overproduction and hypersecretion are common features of chronic inflammatory airway disease. However, in some pathologic conditions such as cystic fibrosis, airway sputum contains little intact mucin and has increased content of DNA, filamentous actin, and lipids. Cough clearance is a secondary airway defense when mucociliary clearance is impaired. The effectiveness of cough depends on volume and flow of exhaled air and the biophysical properties of airway phlegm.
Mucus secretion and clearance is the primary physical defense of the airway epithelium. The energy intensive process of mucin synthesis, oligomerization, granule storage, and, finally, exocytosis serves as protection for epithelial surfaces exposed to an external environment. Mucus secretion defends the eyes, nose, middle ear, airways, and urogenital tract from microbial invasion. Mucin polymers, or mucus, prevent water loss and dehydration of these epithelia, and mucus production and clearance by cilia are an important means of airway hygiene.
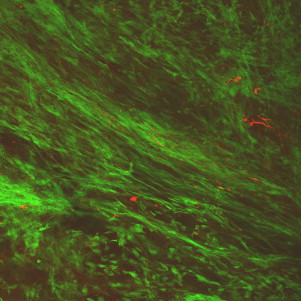
While mucus plays a defensive role, mucus overproduction can overwhelm mucociliary clearance, producing airflow obstruction. Infection and inflammation in the airway leads to poor mucus clearance, stimulates mucus secretion and production, and can cause ciliary dysfunction. Retained secretion containing mucus and inflammatory products with DNA and filamentous (F)-actin copolymers ( Fig. 1 ) is called phlegm from the Greek word for inflammation. Excessive phlegm is cleared by cough, which can be an effective secondary defense of the airway. When phlegm is expectorated, it is then called sputum.
Composition of mucus and phlegm
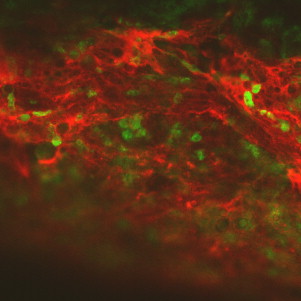
Mucus is the normal secretory product lining the epithelium. It is more than 90% water with the principal polymeric component being the gel-forming mucins MUC5B and MUC5AC. The former is a primary secretory polymeric protein from submucosal glands and the latter is the main gel-forming mucin from surface mucous or goblet cells. There are small amounts of MUC2 in the airways of persons with chronic infection and inflammation such as in bronchiectasis or cystic fibrosis (CF). MUC7 is expressed in serous cells of the submucosal glands but gene expression levels are not altered in chronic airway diseases such as CF. In health, these gel-forming mucins form long, linearly linked oligomers joined by disulfide bonds. In normal mucus, there is minimal intramolecular cross-linking and the polymeric nature comes from the length of the oligomers and their entanglement, producing what has been called a “tangled network.” The abnormal sputum structure seen in conditions like plastic bronchitis or fatal asthma may be due to abnormal cross-linking between adjacent mucin oligomers ( Fig. 2 ).
The core mucin proteins are heavily decorated by sugar moieties forming a bottlebrush structure. Serine and threonine are prominent among these sugars. Studies of the core proteins in mucins have been hampered as antibodies to the core mucin proteins may bind poorly because of the carbohydrate coat.
Between the epithelium and the mucus layer is periciliary fluid, or airway surface fluid (ASF). While ASF was once thought to be a simple iso-osmolar, low density, Newtonian liquid, it is now known to contain a complex network of membrane-bound mucins attached to the epithelium microvilli and cilia, including MUC1 and MUC16. The nature of the interaction between this ASF network and the overlying mucus layer is an area of active investigation. It is thought that the hydration of the airway surface liquid is largely regulated by ion channels in the epithelial surface including the CF transmembrane ion regulator channel, the calcium activated chloride channel, and the epithelial sodium channel.
Mucus clearance is determined, in part, by cilia or airflow acting on the mucus and by the interaction between the mucous layer and the epithelium below. These, in turn, are influenced by the biophysical and surface properties of the mucous layer.
Rheology is the study of the deformation and flow of matter under an applied stress. It is used to characterize material behavior as liquid, solid, or gel-like. An ideal, or Newtonian, liquid responds to an applied stress by an induced deformation with energy loss. The amount of deformation relative to the energy loss determines the loss modulus (viscosity) of the substance. An ideal, or Hookian, solid responds to an applied stress by energy storage and release of this stored energy when the stress ceases. This storage modulus is called elasticity. The complex modulus, also known as mechanical impedance, is the vector sum of viscosity and elasticity and is sometimes referred to as the rigidity factor. A viscoelastic substance or gel, like mucus, responds to an applied stress by initially storing energy and, with continued stress, it will flow like a liquid. When the stress is removed, the stored energy is released. The elastic behavior of mucus is important for ciliary transport as it allows the kinetic energy of beating cilia to be used for mucus transport. In the absence of elasticity, this interaction would be inefficient. Conversely, a viscous component is needed to prevent the elastic mucus from snapping back between ciliary beats and it allows the mucus to flow after secretion from submucosal glands.
For a gel, viscosity and elasticity are not static measures but vary with the energy or stress that is applied. Many gels have an increase in viscosity as the shear rate increases; this is called shear thickening. Some gels will have a decrease in viscosity with applied stress but will thicken when the stress is removed. This reversible shear thinning, or thixotropy, is characteristic of paints which can be spread with an applied stress (like brushing) and then rapidly thicken after the stress is removed, preventing the paint from running off. Some gels have a sudden and dramatic decrease in viscosity that is permanent and caused by irreversible breaking of polymeric bonds under stress. This is called apparent yield stress. The sudden yielding of the polymeric structure may enhance bulk transport by cough.
Viscoelastic behavior that is favorable for ciliary clearance may not be ideal for cough clearance. Ciliary clearance is most effective when there is a fairly low viscosity and preserved elasticity while cough clearance tends to be better with higher viscosity secretion and is less affected by elasticity. However, it is the surface properties of the phlegm that most strongly determine the cough clearability of secretions.
The principal surface properties of mucus or phlegm are the interfacial or surface tension and wettability as measured by the contact angle of a droplet of the secretion. Wettability and interfacial tension can be used to calculate the work of adhesion, which is the attractive force of a liquid or gel to a surface like the airway epithelium. Cohesivity is the tendency for a gel to remain attracted to itself and form threads when slowly stretched. This thread forming ability is called spinnbarkeit or spinnability, and is measured using a device called a Filancemeter. Spinnability can be mathematically transformed into cohesivity, and the product of adhesivity and cohesivity is called tenacity. The tenacity of mucus appears to be the strongest determinant of its cough clearability in vitro.
Mucin secretion and mucus clearance
Mucus secretion is often stimulated by infectious and inflammatory mediators as protective response. There are a variety of pathways involved in mucin secretion, including stimulation of chloride channels, activation of the epithelial growth factor receptor, cell stress, and environmental challenges such as exposure to hyperosmolarity. Surface goblet cells are not directly innervated but they can rapidly degranulate and release mucin to environmental stress. Secretion from the serous cells and mucous cells in the submucosal gland is under receptor-mediated response and neurogenic control, and, therefore, can be modulated by agents like muscarinic antagonists.
Most of the factors that stimulate mucin secretion also stimulate ciliary beating; although faster ciliary beating does not necessarily lead to faster mucociliary transport. Although the term mucus hypersecretion is frequently used for secretion retention in the airways, secretion retention can be due to impaired ciliary function or to mucus hypersecretion that overwhelms the ciliary clearance mechanism. Ciliary dysfunction can be congenital or acquired with acquired ciliary dysfunction often resulting from airway infection or inflammation. Persons with primary ciliary dyskinesia (PCD) who have congenital ciliary dysfunction usually have less lung disease than persons with CF, suggesting that cough is an important clearance mechanism for patients with PCD and that defective mucociliary clearance is probably not the most important factor contributing to lung disease in CF.
The biophysical properties of mucus are modified by secretion hydration, the degree of polymerization of the mucous gel, and additional polymeric constituents such as DNA and F-actin copolymers associated with chronic inflammation and neutrophil necrosis. This secondary network is extremely tenacious and contributes to the poor cough clearability of CF sputum.
Just as it is difficult to know if there is mucus hypersecretion based on secretion retention, it is also true that the volume of sputum expectorated is a poor indicator of the effectiveness of an intervention meant to improve mucus clearance. This is due to temporal changes in the rate of secretion clearance, variable dilution of expectorated sputum with saliva, reticence to expectorate, weakness contributing to a poor expiratory airflow and cough, and reduction in the volume of phlegm because of therapy leading to less sputum expectorated. With the possible exception of short-term acute interventions, expectorated sputum volume is a poor indicator of the degree of impairment or improvement. In addition, the color and texture of sputum do not indicate whether there is hypersecretion or infection.
Cough clearance depends on the properties of the phlegm and the cough. An explosive cough with a large volume of air and rapid airflow is more likely to shear secretions and propel them in the airway. This is associated with effective vocal cord closure and preserved muscle strength. Both of these can be compromised in persons with neuromuscular weakness or patients who receive sedative or paralytic agents. Secretions that are viscous and exhibit apparent yield stress may be easier to propel by cough. It is also easier to cough while sitting or standing upright perhaps because this presents a greater profile of the secretion droplet to the cough airflow.
Because phlegm adherence to the epithelial surface is one of the strongest determinants of cough impairment, there may be a role of mucolytics in unsticking secretions from the epithelium, thus breaking adhesive bonds. Abhesive (the opposite of adhesive) drugs that reduce secretion stickiness can be effective in promoting cough clearance and improving pulmonary function. There is evidence that surfactant phospholipids reduce the surface tension of airway mucus in the proximal airway and make the ciliary beating more effective at propelling mucus. It has been demonstrated that there is surfactant dysfunction and an increase in sputum tenacity associated with diseases such as chronic obstructive pulmonary disease (COPD) and CF.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


