Modified Radical Neck Dissection
James Y. Suen
INTRODUCTION
In 1906, George Crile described the classical radical neck dissection (RND). It was the primary operation for surgical management of metastatic cervical lymph nodes for many decades. Starting in the late 1960s and later, Bocca and Pignataro, O. Suarez, Ballantyne, Jesse, and Suen began to describe modifications of the RND and demonstrated that the control and cure rates were equal to the RND.
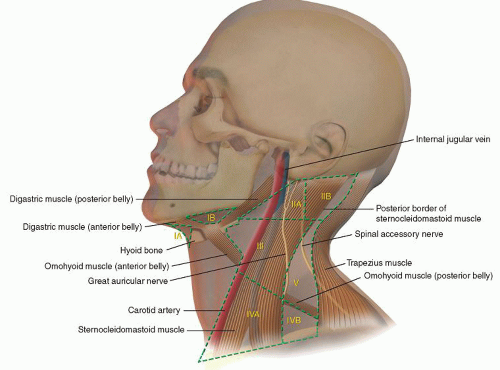
The technique of the modified radical neck dissection (MRND) includes removal of all cervical node levels (I, II, III, IV, and V) (Fig. 4.1) with preservation of one or more of the following: the spinal accessory nerve, the sternocleidomastoid muscle (SCM), and the internal jugular vein (IJV).
Cancer in the neck may represent either a primary cancer or metastasis from a cancer usually primary in the upper aerodigestive tract or the skin of the face or neck. Primary cancers in the neck arise from the tail of the parotid gland, the thyroid, the submandibular gland. Lymphoma is frequently encountered in the neck.
Other sites to consider that can metastasize to the neck include lungs, breast, cervix, prostate, and other intra-abdominal organs.
HISTORY
It is important to ask if the patient has a history of having had a skin cancer of the head and neck removed in the past or has a persistent sore area in the upper aerodigestive tract. Also it is important to inquire about hoarseness, dysphagia, and weight loss.
Question whether the patient has had other cancers, such as lung, breast, intra-abdominal, or prostate. These cancers can spread via lymphatics, and usually metastasize to the left supraclavicular lymph nodes.
PHYSICAL EXAMINATION
A complete examination of the head and neck must be performed. The location of the enlarged nodes can guide you to the primary site. It is important to check the thyroid gland for nodules.
The size, number, and mobility of the lymph nodes are important to note. Fixation to the skin or underlying structures may be a contraindication to this procedure.
CONTRAINDICATIONS
1. Life expectancy of <3 months
2. Uncontrollable cancer at the primary site
3. Lymph nodes fixed deeply and unchanged by irradiation and/or chemotherapy
4. Surgeon who is inexperienced with the MRND
PREOPERATIVE PLANNING
Imaging Studies
a. Ultrasound (US), if the surgeon is experienced using it. US can identify the size and number of cervical lymph nodes and is inexpensive.
b. Computed tomography (CT) scan can be very helpful. It can identify size and numbers of cervical lymph nodes and their internal architecture. It can be performed quickly and is less expensive than a magnetic resonance imaging (MRI) scan.
c. MRI can also provide the same information regarding cervical lymph nodes. It is more expensive and takes a longer time to perform.
d. Positron emission tomography-computed tomography (PET-CT) can identify unknown primaries and will usually identify metastatic cervical lymph nodes. It is also capable of identifying distant metastases or second primary cancers, particularly thyroid. This scan is very expensive and takes several hours to complete.
Biopsy
A fine needle aspiration biopsy (FNAB) should identify the histology, if there is an experienced pathologist reading it. Some metastatic lymph nodes may be necrotic, and if the FNAB samples only the necrotic fluid, the diagnosis may be missed.
With FNAB being available, it is unusual to need an open biopsy. Lymphoma may be difficult to diagnose by this technique and might require removal of a lymph node.
SURGICAL TECHNIQUE
The MRND should remove essentially the same lymph nodes as an RND (Fig. 4.2). The SCM is in the middle of the dissection and makes the surgery more difficult. The SCM can be divided at the inferior attachment to the clavicle to make the surgery easier, or it could be resected with the lymph nodes. The SCM muscle should be removed if tumor is adherent to it or invading into it.
An incision should be planned so that all the lymph nodes can be accessed. My preference is a “hockeystick” incision. This incision begins at the mastoid tip and should be carried almost straight down to just above the clavicle; the incision should be curved medially to the midline. Before I start the incision, I place scratch marks, with a knife, on each side of the incision mark and place these at several spots. With a long incision, it is easier to match these points up for accurate closure of the skin.
The incision is usually made with a monopolar needle-tip cautery through the skin and dermis, then I switch to the blade-tip Bovie. The blade tip is useful for dissecting while in the off position. During the flap incision and elevation, I watch for the external jugular vein that can bleed significantly. This vein can be preserved or ligated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


