Miscellaneous Orbital Tumors
This chapter is reserved for discussion of tumors that do not quite fit the subject matter or titles of previous chapters, and tumors of such uncertain origin that a classification has not been universally accepted.
Alveolar Soft Part Sarcoma
The name of this tumor tells us something about its histopathologic pattern (alveolar or pseudoalveolar), its predominant anatomic sites (soft parts), and malignant course (sarcoma). The tumor is unusual because its histogenesis is uncertain and its clinical course is erratic and unpredictable. Also, considering the tumor has been known since 1952 (Christopherson et al., 1952), it is foremost among all the orbital tumors in this text, time-wise, to have the least amount of publications concerning its nature.
Over the past 50 years, several names have been proposed to correctly identify the histogenesis of the tumor. These are: Malignant nonchromaffin paraganglioma, malignant granular cell myoblastoma, malignant angiosarcoma, malignant angioretinoma, and a unique form of rhabdomyosarcoma. Alas, none of these terms have been universally accepted.
Our own experience with alveolar soft part sarcoma (ASPS) is very limited. We have seen a few cases over the past 50 years, which were sent for clinical evaluation of a probable ASPS but returned home for ultimate definitive histopathologic diagnosis and management. There are no cases of ASPS listed in our 50-year registry of orbital tumors.
Incidence
Incidence data in the third edition of this text (1994) were largely based on publications before 1990. The two publications of the largest series of cases are Enzinger and Weiss (1978) and Lieberman et al. (1989). The former publication was based on 143 cases from the file of the Armed Forces Institute of Pathology. They listed the cases in the order of decreasing frequency and involvement of soft tissues of the lower extremity (thigh), head and neck, upper extremity, and trunk. In the head and neck, the tongue and orbit are the most frequent locations for ASPS.
Lieberman et al., analyzed 102 patients from the file of the Sloan-Kettering Cancer Center in New York City. Sixty-one of the patients were female, and 41 were male. The median age at diagnosis was 22 years (range 2 to 71 years) for females and 27 years (range 5 to 56 years) for males.
The publication of Font et al. (1982) was 12 cases of strictly orbital involvement, 9 cases from their own files and 3 individual case reports from three other authors. In addition, they acknowledged single case reports of ASPS of four publications prior to their review. The age range of these 16 cases was 10 months to 69 years with a median of approximately 20 years.
A recent update is that of Coupland et al. (1999). Their review of the literature disclosed reports totaling 50 cases of primary orbital ASPS. Orbital cases most often occur in children.
Clinical Features
These patients usually present with a painless, straightforward proptosis due to a soft tissue mass in the retrobulbar space of 4 to 6 weeks’ duration. If the mass is more forward in the orbit, between the eyeball and orbital wall, there will be some displacement of the eye with or without diplopia.
Imaging Aspects
On computed tomography (CT), the mass is smooth, well defined with bright enhancement. Magnetic resonance imaging (MRI) shows a high signal intensity relative to
muscle on T1-weighted scans. Angiography will show flow voids (see Fig. 20.1A).
muscle on T1-weighted scans. Angiography will show flow voids (see Fig. 20.1A).
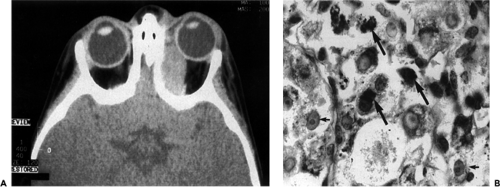 Figure 20.1 Alveolar soft part sarcoma. A: Computed tomography scan shows a large, oval, brightly enhancing, circumscribed mass along the medial wall of the left orbital of a 10-month-old boy. B: Biopsy specimen shows several tumor cells containing numerous diastase-resistant, periodic acid-Schiff (PAS)-positive granules (long arrows) in their cytoplasm. Also note the vesicular nuclei (short arrow), with prominent nucleoli (PAS after diastase, × 1,000). (From Jordan DR, MacDonald H, Noel L, et al. Alveolar soft-part sarcoma of the orbit. Ophthal Surg. 1995;26(3):269–270 , with permission.) |
Pathology
Grossly, these tumors are soft, well circumscribed, with or without a pseudocapsule, well vascularized, and with a pink, tan, or reddish brown color. Microscopically, the polyhedral cells are arranged in an organoid pattern and the groups of cells are delineated by sinusoidal vascular channels (see Fig. 20.1B). The center of a polyhedral group may appear hollow, because of necrosis, and it is responsible for the term, pseudoalveolar, rather than alveolar in reference to the gross pattern of the tumor. The cytoplasm is granular, eosinophilic, and periodic acid-Schiff (PAS) reagent positive. The granular material seems to be the precursor of the diastase-resident crystals, which have never been demonstrated in any other neoplasms (Enzinger and Weiss, 1978). The nuclei of the cells are large and vesicular with prominent nucleoli (see Fig. 20.2). Mitosis is sparse.
Immunohistochemistry
“Immunohistochemical staining showed positive immunoreactivity for neuron-specific enolase, vimentin, p53 (30%), p21 (10%) and cyclin D1 (20%), and negative immunoreactivity for CD45, cytokeratins, S-100 protein, glial fibrillary acidic protein, synaptophysin, chromogranin, calcitonin, serotonin, thyroglobulin, desmin, myosin, actin, HMB-45, pRB, p16, and BCL-2. The endothelium of the tumor blood vessels was demonstrated using JC70a and CD34. The growth fraction of the tumor cells was 3%” (Coupland et al., 1999).
Management and Course
Over the 50-year period this neoplasm has been known, wide and complete local excision of the tumor has been accepted as the best means of controlling the disease. Owing to the scarcity of data, the effectiveness of radiotherapy and
chemotherapy is difficult to evaluate. At present, their roles seem limited to treatment of recurrences. A tumor larger than 50 mm in diameter seems to be associated with higher incidence of local recurrence and metastasis (Lieberman et al., 1989). The tumor may metastasize late in its course, with a median time of 6 years. Thirty-eight percent of recorded metastases appear 10 years after diagnosis. The appearance of metastasis worsens the prognosis, with a median survival of approximately 3 years. There are several exceptions to this survival period reported in the literature. One of these is two survivors of 16 years duration, reported by Font et al., 1982. Metastasis usually occurs in the lung or skeletal bone. Exenteration of the orbit is usually reserved for recurrent tumor.
chemotherapy is difficult to evaluate. At present, their roles seem limited to treatment of recurrences. A tumor larger than 50 mm in diameter seems to be associated with higher incidence of local recurrence and metastasis (Lieberman et al., 1989). The tumor may metastasize late in its course, with a median time of 6 years. Thirty-eight percent of recorded metastases appear 10 years after diagnosis. The appearance of metastasis worsens the prognosis, with a median survival of approximately 3 years. There are several exceptions to this survival period reported in the literature. One of these is two survivors of 16 years duration, reported by Font et al., 1982. Metastasis usually occurs in the lung or skeletal bone. Exenteration of the orbit is usually reserved for recurrent tumor.
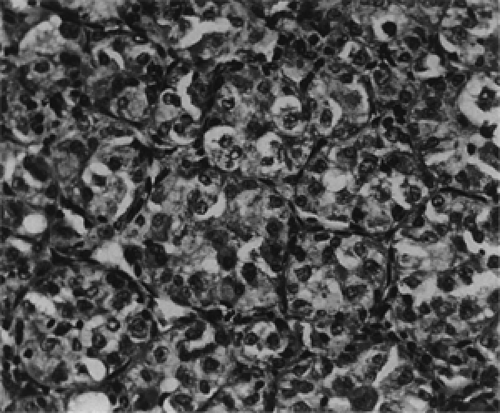 Figure 20.2 Alveolar soft part sarcoma. Specimen from buttock of a 24-year-old woman showing large polygonal cells with abundant cytoplasm arranged in discrete nests, in an organoid pattern. Note some degeneration and sloughing of tumor cells in the center of the nests, simulating an alveolar configuration (× 245). |
Ectopic Lacrimal Gland
The word ectopic is applied to the displacement or malposition, especially if congenital, of some tissue or organ from its usual anatomic position. The terms aberrant and heterotopia are also used in the same context. In ophthalmology, the descriptive designation, aberrant, is usually reserved for isolated choristomatous nodules of lacrimal gland tissue on the surface of the eye. For the deeper deposits of misplaced lacrimal gland in the orbit, ectopic seems to be the preferred term.
In the orbit, we believe it is preferable to restrict these terms to lacrimal gland deposits that are surgically proved to be separate from the normal glandular structure in the lacrimal gland fossa. In the past ophthalmic literature, these terms have sometimes been misused to describe some abnormality in the configuration or function of the lacrimal gland in its normal anatomic site. The latter, in particular, is evident in some case reports, in which lacrimal gland tissue is surgically encountered in the posterolateral retrobulbar space considerably posterior to the normal position of the lacrimal gland. In these cases, a definitive cleavage between the excised tissue and the lacrimal gland is not demonstrated, and the tissue specimens usually show an infiltration of mononuclear cells compatible with nonvasculitic inflammatory tumor in an expanded portion of lacrimal gland.
In the course of an anterolateral orbitotomy, we have occasionally encountered lacrimal gland tissue extending posteriorly toward the orbital apex. These cases always proved to be a posterior extension and enlargement of the lacrimal gland to accommodate a tumefaction associated with a cyst, an inflammatory lesion, or a neoplasm. This situation should not be considered an example of ectopic lacrimal gland.
In a review of the case reports in the literature that fulfill our stricter definition, the ectopic lesion may present in one of three ways. Most often, a small orbital mass is present at birth, or proptosis becomes manifest sometime in the first decade. In either case, the enlargement of the mass is exceedingly slow and, other than proptosis, symptomless. Therefore, removal of the ectopic structure is often delayed. Such was the case with the patients reported by Rush and Leone (1981), a 9-year-old boy; and Baldridge (1970), an 18-year-old male. The ectopic mass removed from a 6-month-old girl (Guy and Quisling, 1989) was believed to be nonprogressive.
In the second type, a relatively sudden proptosis heralds an otherwise dormant heterotopic lesion. The tissue excised from such a case usually shows a diffuse infiltration of inflammatory cells of some degree, suggesting that a reactive response to the ectopic tissue is responsible for the acute proptosis. The cases reported by Jakobiec and Font (1986), a 69-year-old man; Guy and Quisling, a 16-month-old boy; and Green and Zimmerman (1967), a 45-year-old woman may be of this type.
Last is the change that occurs in an ectopic nest that undertakes some secretory function, resulting in an epithelial-lined cyst similar to a ductal structure in the normal gland. Such was the mass near the supraorbital notch of a 16-year-old girl reported by Green and Zimmerman (1967). The cystic structure was drained but not completely excised. Five years later, another orbitotomy was performed to excise a recurrent cyst along the medial orbital wall. Postoperatively, the patient’s proptosis persisted. The patient was killed in an automobile accident shortly thereafter. An autopsy was performed that showed a malignant transformation (adenocarcinoma) of the ectopic lacrimal gland remnants.
A recent report of an orbital ectopic gland cyst (Kao et al., 2000) can be added to the preceding list. A 33-year-old man had a palpable mass above the inferior medial orbital rim for nearly 2 years. On CT scan, the mass was near the inferior rectus muscle. It appeared to be a thin-walled cyst measuring 15 × 12 × 13 mm containing clear fluid. The cyst was enucleated intact. It consisted of a small nest of normal lacrimal tissue surrounded by a cyst lined with two layers of lacrimal duct epithelial cells. Neither of the reports of lacrimal gland ectopia by McCulley et al. (2002) and Sakurai et al. (1997) meet our strict requirements for inclusion in the preceding lists.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


