Parotidectomy is a commonly performed procedure for both benign and malignant lesions. When a significant portion of the gland is resected and the lost tissue volume is not replaced, a disfiguring contour defect can result. This defect can be disfiguring and have a profound impact on quality of life. Large defects are best replaced with vascularized tissue to provide stable volume.
Key points
- •
The contour deformity created when volume is not replaced after parotidectomy can be disfiguring and can significantly affect quality of life.
- •
Large-volume deficits are best corrected with vascularized adipose tissue because it is accurate acute contour restoration and provides a stable result over time.
- •
The preferred donor graft is the anterolateral thigh (ALT) free flap, because the donor site morbidity is minimal, it provides an ample tissue source that does not include denervated muscle, it can be harvested with a skin paddle if needed, and it allows access to neural and fascial graft tissue if needed.
- •
In the setting of facial paralysis, concurrent orthodromic temporalis tendon transfer is safe, adds minimal morbidity, and makes a significant contribution to facial symmetry.
Parotidectomy is commonly performed to address benign and malignant processes involving the parotid gland itself, aggressive cutaneous facial tumors, and adjacent head and neck malignancies. The surgical spectrum includes partial and superficial gland resection, total gland resection, and more radical procedures that include sacrifice of the facial nerve and adjacent structures. Complications also cover a broad spectrum and include facial nerve weakness to complete paralysis, sialocele, Frey syndrome, infection, hematoma, and contour deformities. Due to its location at the lateral cheek and angle of the mandible, a volume deficit in the parotid bed can lead to an obvious and unappealing deformity that is easily visible on both direct and lateral facial views. As a result, resection of substantial soft tissue in the process of parotidectomy, irrespective of facial nerve status, can result in dramatic and obvious disfigurement.
Facial symmetry is widely accepted as one of the key measurements of human beauty and, even more importantly, facial asymmetry and deformity have been shown to impart a social penalty beyond self-image. More than 50% of patients report being affected by facial contour abnormalities after parotidectomy. In the setting of radical parotidectomy, the effects of volume loss are arguably as profound and debilitating as the facial paralysis, because they compound the deformities imparted by loss of facial tone and movement.
There are several methods that have been described to fill the surgical defect created by parotidectomy, including sternocleidomastoid rotation flaps, superficial musculoaponeurotic system (SMAS) interposition flaps, temporoparietal biparietal fascia (TPF) flaps, autologous free fat or dermal/fat grafts, and processed alloplastic dermal implants. These may provide benefit for limited or superficial gland resection, but none of these methods provides enough bulk to restore facial symmetry after total gland resection. Additionally, many patients who require total and especially radical parotidectomy are subjected to postoperative radiation therapy. This assault can diminish volume achieved by tissue with a tenuous vascular supply. Furthermore, the use of acellular dermal implants has been associated with higher complication rates in the setting of previous or postoperative radiation. Critically, denervated muscle flaps provide short-term contour improvement, but long-term volume restoration is unreliable, because denervated muscle flaps lose bulk over time due to atrophy.
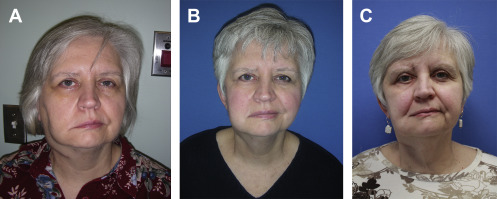
As the use of vascularized free tissue grafts has become commonplace in the reconstruction of complex head and neck defects, microvascular technique has become safe, reliable, and efficient. This has led to an expansion of indications to optimize facial form and function, including reconstruction of the isolated facial contour defects. The benefits provided by this method include accurate, lasting, and radiation-resistant volume correction ( Fig. 1 ); access to additional tissue at donor sites for nerve grafting and facial reanimation; and potential protection from radiation-induced complications. As a result, free tissue transfer is becoming the criterion standard for management of large-volume parotidectomy defects.
Past critiques of aggressive volume correction have argued that addition of tissue for the sake of contour can interfere with a surgeon’s surveillance of the surgical site for recurrence and that free tissue transfer adds additional morbidity at the donor and anastomosis sites. With current imaging techniques, any neoplastic tissue is readily distinguished from reconstructive tissue, mitigating the potential compromise of oncologic surveillance. Many total parotidectomies in the setting of malignancy are performed with concurrent neck dissection, eliminating the need for additional surgery required to locate donor vessels for microvascular anastomosis. When no concurrent neck dissection is planned, suitable vessels for anastomosis can generally be accessed through the existing parotidectomy defect. In cases of these vessels found insufficient, the pedicle can be tunneled under the skin to a minimal access incision. Furthermore, with newer flap harvest sites and techniques, donor site morbidity is minimal, not significantly more than the harvest of a nerve graft.
Many different free flaps, including radial forearm, lateral arm, gastrocnemius, groin, inferior epigastric perforator, and parascapular, have been described in the reconstruction of the parotidectomy defect. For several reasons, the authors find that an ALT flap is the preferred option in almost every instance. The most compelling argument for its use is a lack of donor site morbidity. The only long-term evidence left at the harvest site is a scar less obvious than that left by procuring a skin graft. Careful design and closure of the incision, for instance, with the application of a distal m-plasty, allows a surgeon to harvest a flap with a large skin paddle and achieve primary closure with the incision terminating above the hem of a pair of shorts. The donor site also allows access for the concurrent harvest of a tensor fascia lata graft if facial reanimation is to be performed as well as the motor nerve to the vastus lateralis (MNVL) when needed as a graft for facial reinnervation. The area and bulk of the ALT flap can be adjusted over a wide range depending on body habitus and volume needs, incorporating fascia, subcutaneous fat, and/or dermis. Thin flaps may be folded and thick flaps may be primarily thinned to create an ideal fit for the defect. Finally, the ALT flap is easily concurrently harvested by a second surgical team, minimizing added operative time for reconstruction.
Primary volume restoration
Given ready access to both the surgical defect and vessels for microvascular anastomoses, total parotidectomy soft tissue defects are optimally managed at the same operative setting as the ablative procedure. Furthermore, in the setting of malignancy and anticipated postoperative radiation therapy, immediate reconstruction with vascularized tissue may convey an additional radioprotective effect. This concept is supported by well-established evidence of revascularization of surrounding structures after transplantation of an adjacent vascular pedicle.
If immediate reconstruction is planned, flap harvest is optimally begun and completed concomitantly with the ablative procedure. Given the distance of the thigh from the head and neck region and the lack of requirement of a tourniquet, the ALT harvest site is optimally suited for this method. Furthermore, presence of ample skin and soft tissue in the typical thigh allows for harvest of a flap that accommodates an extended defect yet is still amenable to complete advancement flap closure. This volume can then be adjusted for size and contour once full margin clearance has been attained.
In the setting of radical parotidectomy, ALT free flap harvest is performed in a manner that allows for concomitant facial nerve reinnervation and reanimation if this is also required. In this instance, a vascularized contour flap is performed along with spanning grafts from the MNVL and orthodromic temporalis tendon transfer combined with a fascia lata extension for lower lip suspension. Aside from the temporalis tendon, all these elements are readily available in a single harvest site.
ALT flap harvest is begun with Doppler probe identification and marking of perforators to the overlying skin near the midpoint between the anterosuperior iliac spine and the superolateral patella. A cutaneous paddle amenable to primary advancement closure is always included in the flap harvest regardless of whether a skin defect is anticipated. This facilitates closure without significant contour defect in the thigh, allows for flap manipulation with less trauma to underlying structures, and provides an external monitor paddle when this is desired. Furthermore, this technique provides a vascularized dermal graft if additional bulk is required in patients with thin thighs.
Harvest is first begun with a single vertical incision at the medial aspect of the skin paddle, dissection to and then through the fascia overlying rectus femoris muscle, and identification of septocutaneous or, far more commonly, musculocutaneous perforators. In cases of the musculocutaneous perforators, these are followed through the vastus lateralis muscle until the vascular pedicle is reached. Once the location and vascular origin of the perforators are confirmed, full cutaneous flap design is completed, and the incisions are created. Commonly, an area of vascularized fascia lata of significantly greater dimensions than the skin paddle is harvested. This allows for further versatility with regard to volume replacement without additional harvest site morbidity. At this point, perforators are followed circumferentially through the vastus lateralis muscle with complete sparing of the surrounding musculature (perforator flap technique) ( Fig. 2 ). This method is critical to maximize the length of the vascular pedicle and, most importantly, to minimize the importation of denervated muscle into the volume correction because it is subject to tissue atrophy over time.
During pedicle dissection, MNVLs are encountered and dissected away from the vessels. These nerves, with their long branching pattern and redundant nature, provide an ideal substrate for reinnervation if this is required ( Fig. 3 ). Because of their redundancy proximally, nerve harvest or sacrifice is not associated with functional impairment. Harvest concomitantly with the ALT flap avoids an additional donor site morbidity and provides a potential advantage of motor nerve grafts for motor nerve replacement. Additionally, in instances of radical parotidectomy and anticipated temporalis tendon transfer, a nonvascularized 2-cm by 10-cm slip of remaining fascia lata is removed separately from the lateral thigh.
After the ALT free flap is revascularized, it is draped in the parotid bed and any existing neck dissection defect and then circumferentially suspended to SMAS and deep soft tissues. The flap is then modified to establish symmetric facial contour and skin and subcutaneous tissue is removed as required to accomplish this goal. Facial contour is slightly overcorrected to compensate for flap edema during harvest and reperfusion; however, gross overcorrection is not performed, because the soft tissue volume remains stable over time. This ability to reliably maintain established contour differentiates this reconstruction from the inevitable atrophy of both free and pedicled denervated muscle flaps. If pedicle geometry and soft tissue orientation permit, a cutaneous monitoring segment is created during flap modification and secured between the native skin flaps prior to closure ( Fig. 4 ).
Although external skin defect reconstruction with color-mismatched ALT skin is not optimal, restoration of large areas of skin with locoregional flaps often requires extensive dissection and skin tension that can obscure precise volume correction and accuracy of facial suspension. As a result, these defects are often addressed by an ALT skin paddle, which can be reduced in size by locoregional advancement. At a later point after completion of treatment, and often in the office setting under local anesthesia, color-mismatched skin can often be removed or minimized with serial excisions and local advancement flaps.
Management of the Radical Parotidectomy Defect
The setting of radical parotidectomy with facial nerve sacrifice presents issues and challenges beyond the scope of facial contour correction. Simultaneous management of facial nerve and reanimation issues allows for the best potential for recovery and provides the most rapid return to functional status. Immediate facial nerve grafting provides the best potential for long-term recovery of tone and function; however, grafting alone is not an ideal option in this patient population for several reasons. The potential for a good clinical outcome with nerve grafting alone is significantly decreased in typically elderly patients with parotid cancer based on age alone. In addition, the high potential for tumor recurrence and greater functional compromise of paralysis in this group make the lag time of up to 12 months for experiencing clinical effects of reinnervation less tolerable or acceptable. As a result, the authors typically use a combined approach with both nerve grafting and facial reanimation performed at the same setting as contour correction ( Fig. 5 ).
Both static facial suspensions and dynamic muscle transfer have been endorsed to provide immediate rehabilitation at the time of radical parotidectomy. Orthodromic temporalis tendon transfer, a well-established and increasingly popular reanimation technique, can impart both facial symmetry at rest and voluntary facial movement without creation of a secondary harvest site defect. Also favoring this option in the setting of parotidectomy, access to the insertion of the temporalis tendon on the coronoid is easily obtained through the same incision. Furthermore, this procedure can be performed without compromising the potential for reinnervation. Although the degree of voluntary facial movement generated through this procedure is variable and possibly affected by radiation therapy, surgical outcomes that establish immediate facial symmetry and support are nearly universal. These latter benefits are the most critical to attain in this oncologic patient population.
Although free muscle transfer is often cited as the ideal reanimation method to provide the greatest potential for restoration of dynamic facial function, this method is not considered a component of primary rehabilitation in the oncologic setting. Functional recovery using this technique is delayed as it may take months for reinnervation to occur, and radiation therapy compounds the unpredictable effects of long-term function of transferred free muscle. In select patients, such as those who are young and have a favorable oncologic prognosis, rehabilitation with free muscle flaps may be considered in delayed fashion.
Reanimation Technique
In the setting of both contour correction and reanimation, the ALT flap is typically revascularized and then carefully oriented inferiorly and monitored while nerve grafting and temporalis tendon transfer are under way (see Fig. 5 B). Attention is then focused on accessing the tendon of the temporalis muscle on the coronoid process. The masseter muscle, if unresected, is elevated off the lateral mandible and retracted medially to expose the coronoid process. The motor nerve to the masseter muscle is carefully preserved and in some instances identified and isolated for grafting purposes. The lateral coronoid is fully exposed and the tendon on the medial aspect is carefully elevated with superiostial dissection and protected by a right angle hemostat before coronoidectomy is performed with a sagittal saw ( Fig. 6 A ). The underlying temporalis tendon is now fully exposed and the full length is preserved. The portion of the tendon attached on the medial coronoid base and to the posterior-medial aspect of the mandibular angle that provide optimal length and avoid the need for fascia lata extension grafts (except to the midline lower lip). It is the authors’ opinion that minimizing use of extension grafts is critical to ensuring reliable movement and position after postoperative radiation therapy.



