BAUSCH & LOMB HANSATOME & ZYOPTIX XP
This section will introduce the reader to the Hansatome & Zyoptix XP, which are similar in function. Basic information and pearls for the operation of this instrument are provided; however, a specific certification course must be completed prior to its use.
The Hansatome is a two-piece mechanical device designed to create a superior hinged flap as the microkeratome pivots on the slotted post of a suction ring. The motor is mounted vertically over the microkeratome head and the single-gear mechanism allows it to engage and rotate along the curved elevated gear track on the suction ring opposite the slotted pivot post. The blade oscillates within the microkeratome head at 7,500 rpm. The standard suction rings have an outer diameter of 20 mm.
Micro-rings have the same inner diameters as the standard rings, but have an outer diameter of 19 mm. The micro-rings are useful for patients with narrow palpebral fissures or tight lids. The available inner diameters in both the standard rings and the micro-rings are 8.5 and 9.5 mm. The 8.5-mm ring is appropriate for patients with steeper corneas; that is, keratometry readings of >45.00 diopters (D), or when a smaller flap is adequate (
Table 4.1). When a larger flap is required, such as in custom treatments, large pupil treatments, hyperopia, or mixed astigmatism, or when the cornea is relatively flat, the 9.5-mm ring is preferred. Patients with keratometry readings >48.00 D are at increased risk of buttonholed flaps, and patients with readings <40.00 D are at heightened risk of a free cap.
Some surgeons feel that the superior hinge is less desirable in the patient with a relative tear deficiency, because nerve bundles entering the cornea from the 3 and 9 o’clock meridians will both be severed. A nasal hinge would preserve the nerves entering the cornea from the nasal side. Other surgeons do not feel this is a significant problem provided the surface can be stabilized preoperatively with punctal plugs, tear supplements, or topical cyclosporine. Any dry eye patient undergoing LASIK surgery should be cautioned about the added risk. All efforts should be made to enhance tear stability prior to surgery. Dry eye patients whose problem cannot be significantly improved with therapy have more problems with recovery after LASIK surgery, regardless of which microkeratome is used.
The most commonly used plates are the 160- and 180-µm plates; however, 130- and 200-µm plates are also available. The actual central flap thickness is typically less than the chosen plate thickness; however, the surgeon is advised to measure the actual flap thickness using intraoperative pachymetry. This is because of the variance that is possible
between intended and actual flap thickness. The Hansatome will usually make an even thinner flap if the patient has a thin cornea. The mean central flap thickness created with the 160-mm plate is 129 µm ± 21µm, and for the 180-µm plate is 136 µm ± 25µm.
An early problem with the Hansatome was the relatively high incidence of epithelial loosening and defects within the newly created flap. This was particularly true in patients more than 50 years old, or with subclinical anterior basement membrane dystrophy. Since the advent of the Zero Compression Head, incidences of epithelial loosening and defects in the flap have fallen dramatically. The left/right eye adapter fits between the motor and the microkeratome head. It is labeled such that only the appropriate label “R” or “L” will be visible once the unit is properly assembled.
Prior to the operation, the scrub technician and surgeon should review the microkeratome checklist. The placement of the suction ring is similar to that for other microkeratomes.
Firm posterior pressure will help avoid pseudosuction, in which suction is applied to the conjunctiva but not the sclera. After suction has been achieved, the ring is allowed to float anteriorly, and the tissue that could potentially interfere with the microkeratome pass is swept aside.
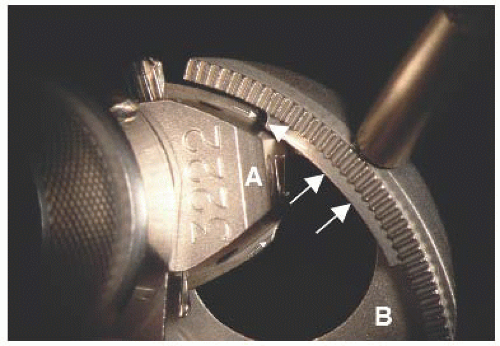
Once suction has been achieved, the intraocular pressure (IOP) should be checked and a pressure >65 mmHg confirmed. The cornea is moistened with topical anesthetic. The Hansatome is placed on the slotted pivot post of the ring. If the microkeratome is not aligned properly, it will not seat. Twisting the head or forcing the microkeratome down on the post will not be effective. The microkeratome should be removed, realigned properly, and then replaced. A pearl for easily aligning the microkeratome with the post is to look for landmarks on the ring and the head. On the ring of the Hansatome there is a ledge central to and just below the gear track that serves as an important landmark. There is a dovetail on either side of the microkeratome head. The leading edge of the appropriate dovetail should be lined up with the inferior border of the ring ledge. This will allow the microkeratome to easily drop down on the pivot post, and the leading edge of the microkeratome will drop beneath the ring ledge. With a slight manual advancement, the microkeratome is fully engaged and ready for automated advancement. Proper alignment of these landmarks is illustrated in
Figure 4.1 (See Video 2).
Once the gear is engaged in the track, the forward pedal is depressed and the surgeon can let go of the microkeratome, allowing it to complete its pass. Holding the ring handle stabilizes the device. As the Hansatome is reversed, suction can be released to avoid traumatizing the corneal epithelium. The patient should be cautioned about moving the eye when suction is released and the flap is still within the device. The Hansatome and ring are then lifted off the eye as a unit.
If the microkeratome fails to advance at the first tooth of the gear track, before the cornea has been engaged, it is safe to reverse the device, reengage, and proceed. However, if the flap is partially cut and the microkeratome becomes jammed, do not reverse and then advance. This will result in an irregular flap. If drape, lid, or speculum is blocking the Hansatome pass, clearing the track or widening the speculum may allow the pass to continue. In this case, it is safe to attempt to advance the microkeratome. If the Hansatome becomes jammed and will not reverse at the
end of the pass, suction can be released and the unit lifted anteriorly and inferiorly. The unit should not be disassembled until the flap has been inspected, in case a free cap has occurred and the tissue is still in or on the Hansatome.
Bausch & Lomb has also manufactured the Zyoptix XP microkeratome. The Zyoptix XP was developed in order to reduce the variance seen between the predicted and the actual flap thickness. In contrast to the Hansatome, the Zyoptix XP has an elevated gearless drive assembly designed to minimize contact with eyelashes or drapes. The translation drive has a “two-link” mechanism, and the suction ring supports this link mechanism. The ring has also been designed to reduce the risk of pseudosuction and suction breaks. The microkeratome has the additional advantage of 360-degree variable hinge positioning. The device can be adjusted for the particular eye by flipping a lever to the right or left. Data provided by Bausch & Lomb (2005) for the 120-µm plate show a mean flap thickness of 116.0 µm ±16.1 µm with a range of 60 to 145 µm (n = 50).