Purpose
To determine by magnetic resonance imaging (MRI) the prevalence and anatomy of anomalous extraocular muscle (EOM) bands.
Design
Prospective, observational case series.
Methods
High-resolution, multipositional, surface coil orbital MRI was performed using T1 or T2 fast spin echo weighting with target fixation control under a prospective protocol in normal adult subjects and a diverse group of strabismic patients between 1996 and 2009. Images demonstrating anomalous EOM bands were analyzed digitally to evaluate their sizes and paths, correlating findings with complete ophthalmic and motility examinations.
Results
Among 118 orthotropic and 453 strabismic subjects, 1 (0.8%) orthotropic and 11 (2.4%) strabismic subjects exhibited unilateral or bilateral orbital bands having MRI signal characteristics identical to EOM. Most bands occurred without other EOM dysplasia and coursed in the retrobulbar space between rectus EOMs such as the medial rectus to lateral rectus, from superior to inferior rectus, or from 1 EOM to the globe. In 2 cases, horizontal bands from the medial rectus to lateral rectus muscles immediately posterior to the globe apparently limited supraduction by collision with the optic nerve. All bands were too deep to be approached via conventional strabismus surgical approaches.
Conclusions
Approximately 2% of humans exhibit on MRI deep orbital bands consistent with supernumerary EOMs. Although band anatomy is nonoculorotary, some bands may cause restrictive strabismus.
The normal human orbit contains 6 extrinsic oculorotary extraocular muscles (EOMs), the levator palpebrae superioris muscle, and the orbicularis oculi muscle. Abnormalities of the EOMs are believed to be rare. Numerical aberrations of the EOMs have been reported, consisting of both absences of rectus and oblique EOMs as well as supernumerary bands resembling EOMs. Sparse case reports exist describing these supernumerary EOMs, most of which have been discovered after death or during surgery. Sacks published one of the first reports describing anomalous EOM bands discovered by cadaveric dissection.
Imaging of anomalous EOM bands has been limited because of their small dimensions as well as irregular courses and orientations. Indeed, until recently, EOMs themselves were difficult to characterize by imaging alone. EOM activity was inferred indirectly from clinical examinations, force generation testing, and electromyography. However, recent advances in orbital imaging with high-resolution magnetic resonance imaging (MRI) have clarified noninvasively the functional orbital anatomic features of living patients. Within the last decade, MRI has been able to demonstrate directly EOM locations, sizes, contractility, and innervation. Demer and associates illustrated the usefulness of high-resolution MRI in detecting hypoplasia and misdirection of cranial nerves, as well as neurogenic EOM atrophy in strabismus caused by cranial nerve palsies. In addition, MRI has been used to detect structural changes in Brown syndrome as well as widespread orbital dysinnervation in congenital fibrosis of the extraocular muscles. It seems reasonable to anticipate that anomalies in orbital anatomic features would be more likely discovered by MRI than by cadaveric dissections.
Herein, we demonstrate the usefulness of high-resolution orbital MRI in detecting and characterizing supernumerary EOM bands. We present a series of cases in which high-resolution MRI disclosed anomalous EOMs having a wide variety of morphologic features and discuss the potential clinical impact of these bands on ocular motility.
Methods
Between December 1, 1996, and December 31, 2009, a total of 118 orthotropic volunteers and 453 strabismic patients underwent high-resolution orbital imaging under a prospective protocol designed to optimize image resolution using the best available methods at the time. We selected for detailed analysis those cases with evidence of anomalous EOMs. Written informed consent was obtained prospectively according to a protocol approved by the Institutional Review Board of the University of California, Los Angeles, and in conformity with the Health Insurance Portability and Accountability Act. All subjects underwent complete ophthalmic examinations, including visual acuity assessment, stereopsis, slit-lamp and funduscopic examination, and cycloplegic or manifest refraction, or both.
High-resolution orbital MRI was performed using T1 or T2 fast spin echo weighting using a 1.5-T scanner (Signa; General Electric, Milwaukee, Wisconsin, USA). A surface coil technique was used for obtaining high-resolution orbital MRI with 2- to 3-mm image planes as described previously. Images always were obtained in quasicoronal planes perpendicular to the long axes of each orbit, as well as in other planes as appropriate to individual findings. Each orbit of alert subjects was scanned during fixation of a central target by the corresponding eye; subjects too young for cooperation were scanned under general anesthesia. Digital MRI images were converted into a spatially calibrated, 8-bit tagged image file format with the use of locally developed software and were quantified with the program Image J (Rasband WS. ImageJ. United States National Institutes of Health, Bethesda, Maryland; http://rsb.info.nih.gov/ij/ , 1997–2009).
To measure lengths of anomalous EOM bands, adjacent image sets were resliced along the paths taken by the bands. The cross-sectional area of each anomalous EOM band was computed using the area function of the ImageJ program after manually outlining the band’s thickest portion. Cross-sectional areas of the rectus EOMs were measured similarly at their thickest portions. To avoid confounding the measurements by contractile changes in extraocular muscle size induced by varying eye position, measurements were obtained in central gaze. To compare the prevalence of the anomalous EOM bands between the strabismic population and nonstrabismic population, the Fisher exact test was performed using GraphPad Prism for Windows (GraphPad Prism 5, Version 5.01, 2007; Graphpad Software, La Jolla, California, USA).
Results
From December 1996 through December 2009, a total of 118 normal subjects without strabismus and 453 strabismic subjects underwent high-resolution orbital MRI. Twelve of these subjects were identified who had a band consistent with 1 or more supernumerary EOMs. Bands had intensities equivalent to that of typical EOMs. Eleven of these subjects had underlying strabismus, giving a prevalence of supernumerary EOM bands in strabismic subjects of 2.4% and in normal subjects of 0.8%, a difference that was not statistically significant ( P = .48).
In the Table , the anomalous EOM bands’ sizes and courses are tabulated, as well as the cross-sectional areas of the rectus EOM in the corresponding orbits. Three subjects had supernumerary EOM bands connecting the vertical rectus muscles, 4 patients had bands connecting the horizontal rectus EOMs, 1 subject had a band connecting the lateral rectus (LR) muscle to inferior rectus (IR) muscle, 1 subject had a band coursing from the IR muscle to the globe, and 3 subjects had bands connecting the levator palpebrae superioris muscle to the superior oblique (SO) muscle. In all cases, the anomalous EOM band had a smaller cross-sectional area than each of the corresponding rectus EOMs.
| Case No. | Age (yrs) | Sex | Underlying Condition | Eye | Muscle Band Course | Band Length (mm) | Cross-section (mm 2 ) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Band | SR | MR | IR | LR | |||||||
| 1 | 1.3 | M | CFEOM type III both eyes | Right | Temporal edges of SR and IR | 17.1 | 7.1 | 31.4 | 37.1 | 27.1 | 32.0 |
| 1 | 1.3 | M | CFEOM type III both eyes | Left | Temporal edges of SR and IR | 16.6 | 5.7 | 30.8 | 42.3 | 32.8 | 33.0 |
| 2 | 61 | M | SO palsy left eye, INO both eyes | Left | Temporal edges of SR and IR | 14.9 | 3.1 | 44.2 | 34.5 | 35.5 | 35.8 |
| 3 | 16 | F | Partially accommodative V esotropia | Right | Temporal edges of SR and IR | 17.6 | 3.4 | 35.7 | 38.7 | 30.2 | 32.0 |
| 4 | 60 | M | Thyroid ophthalmopathy | Left | Central portion of MR to superior edge of LR | 19.2 | 4.0 | 42.7 | 51.4 | 46.3 | 43.5 |
| 5 | 18 | M | Normal subject | Right | Central portions of MR and LR | 16.9 | 4.2 | 42.6 | 37.1 | 24.6 | 42.4 |
| 6 | 38 | F | Familial monocular vertical gaze deficiency | Right | Inferior edges of MR and LR | 14.7 | 6.3 | 27.4 | 45.8 | 14.8 | 42.4 |
| 7 | 1.8 | M | CFEOM type III both eyes | Left | Inferior edges of MR and LR | 12.8 | 5.2 | 8.13 | 17.5 | 6.14 | 24.7 |
| 8 | 56 | M | Left hypertropia | Right | LR to IR | 13.0 | 3.5 | 41.1 | 35.3 | 27.6 | 41.4 |
| 9 | 35 | F | Infantile esotropia | Left | Supertemporal course from IR to temporal globe equator | 15.3 | 3.6 | 35.3 | 25.1 | 27.3 | 45.3 |
| 10 | 14 | M | Duane syndrome right eye, type III | Left | Nasal course from SR-LPS to SO near trochlea | 7.7 | 4.6 | 26.9 | 42.6 | 33.5 | 37.4 |
| 11 | 52 | F | Duane syndrome both eyes, type III | Left | Nasal edge of SR-LPS to SO near trochlea | 10.8 | 2.1 | 24.2 | 27.0 | 23.6 | 36.6 |
| 12 | 38 | M | Duane syndrome right eye, type I | Left | Nasal edge of SR-LPS to SO near trochlea | 7.2 | 3.0 | 24.8 | 24.7 | 27.1 | 17.7 |
Vertical Rectus Muscle Connections
Case 1
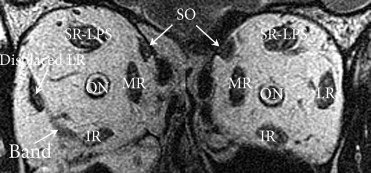
This 14-month-old boy had congenital blepharoptosis and supranuclear palsy of upward gaze in both eyes at presentation. He was orthophoric in central gaze. He was unable to move either eye above the horizontal midposition on attempted supraversion. MRI revealed bilateral muscular bands connecting the temporal edges of the IR muscle to the SR muscle in mid orbit ( Figure 1 ).
Case 2
This 61-year-old man had fluctuating vertical diplopia, worsening with exercise, at presentation. Harada-Ito surgery had been performed in the left eye 5 years previously for left SO muscle palsy. He had right hypertropia (4 Δ in central gaze, 12 Δ in infraversion). He also exhibited mild limitation of supraduction in both eyes, abduction nystagmus in both eyes with slow adduction saccades in both eyes, suggesting bilateral internuclear ophthalmoplegia. MRI demonstrated a muscular band between the temporal edges of the left SR muscle and left IR muscle posterior to the globe.
Case 3
This 16-year-old girl had a history of partially accommodative V-pattern esotropia. There was 20 Δ esotropia in central gaze, with overelevation in adduction in both eyes, but normal horizontal ductions in both eyes. MRI demonstrated an accessory EOM band between the temporal edges of the right SR muscle and IR muscle posterior to the globe.
Horizontal Rectus Muscle Connections
Case 4
This 60-year-old man had a diagnosis of thyroid ophthalmopathy. There was 25 Δ esotropia and 12 Δ left hypertropia in central gaze with moderate limitation to supraduction in the right eye in adduction, and mild overdepression of the right eye in adduction. There was also mild limitation of abduction in both eyes and mild limitation to infraduction in the left eye in adduction. MRI demonstrated enlargement of all EOMs, sparing of the tendons, as well as a muscular band between the central portion of the left MR muscle and the superior edge of the LR muscle posterior to the globe. Notably, the patient previously had undergone a standard orbital MRI elsewhere that failed to detect this muscular band.
Case 5
This 18-year-old man was recruited as a normal control subject. He had a normal ophthalmic examination with no signs of strabismus, including normal Hess screen test results, normal ocular versions, and stereopsis of 40 seconds of arc. MRI demonstrated a muscular band connecting the central portions of the right MR muscle and LR muscle posterior to the globe.
Case 6
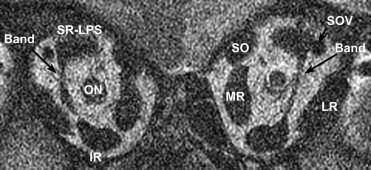
This 38-year-old woman had a history of an unspecified strabismus surgery at age 9 years and also reported a daughter with strabismus. There was 17 Δ right exotropia and 12 Δ right hypotropia in central gaze, with limitation of supraduction above horizontal midposition, and mild limitation to infraduction in the right eye. MRI demonstrated a hypoplastic right IR muscle and a band isointense to EOM connecting the inferior edges of the right MR muscle to the superior edge of the LR muscle posterior to the globe ( Figure 2 ). On supraversion, this EOM band appeared to contact the inferior edge of the optic nerve.
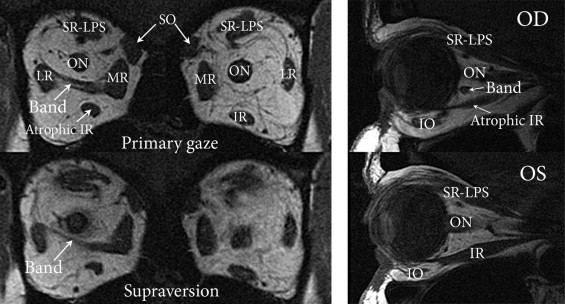
Case 7
This 22-month-old boy had a history of plagiocephaly, left ptosis, and inability to supraduct the left globe. On examination, he had 30 Δ exotropia and 15 Δ left hypotropia in primary gaze. The child was unable to supraduct the left eye above the horizontal midposition. High-resolution MRI demonstrated unilateral hypoplasia of the left IR and SR muscles, as well as an anomalous EOM band connecting the inferior edges of the left MR and LR muscles. Because of the patient’s age and difficulty with cooperation, the orbits could not be scanned in eccentric gaze positions. During subsequent strabismus surgery, the surgeon (J.L.D.) noted that resistance to passive supraduction in the left eye persisted after left inferior rectus disinsertion.
Other Rectus Muscle Bands
Case 8
This 56-year-old man had a 3-year history of intermittent vertical diplopia and right head tilt. There was a left hypertropia (22 Δ in primary gaze), limitation of infraduction in adduction in the left eye, overelevation of the left eye in adduction, and 8 degrees of relative excyclotorsion in the left eye. MRI demonstrated an abnormal band isointense to EOM extending from the right LR to IR muscles. In addition, the right LR muscle was found to be inferiorly displaced; the SO muscles were normal and symmetrical ( Figure 3 ).