Macular Choroidal Melanoma
Jerry A. Shields
Carol L. Shields
Uveal melanoma is the most common primary intraocular malignant tumor among Caucasians. The epidemiology, clinical features, diagnostic approaches, management, and prognosis of uveal melanoma have been discussed in detail in recent textbooks (1,2). Choroidal melanomas that occur in the macular area present unique therapeutic considerations, because their treatment sometimes can cause considerable visual loss. This chapter reviews the diagnosis and management of melanomas that arise in the macular area, a region that we define as an area about 6 mm in diameter with the foveola as its center. Because recent publications (1,2) have described this tumor in great detail, this chapter briefly reviews the diagnosis and management of macular choroidal melanoma.
CLINICAL FEATURES
Macular choroidal melanoma can assume a variety of clinical features (1,2). It usually presents as a sessile or dome-shaped pigmented mass located deep to the sensory retina (Fig. 49-1). If located in the macular area, it is more likely to have surface orange pigment at the level of the overlying retinal pigment epithelium. A secondary retinal detachment frequently accounts for visual impairment. Occasionally, a macular choroidal melanoma can be partly or entirely nonpigmented. With continued growth, the tumor can rupture Bruch’s membrane and assume a mushroom shape. If the tumor is amelanotic, blood vessels in the mass are visible ophthalmoscopically. In some instances, larger macular choroidal melanoma can cause total retinal detachment, cataract, congestive glaucoma, and extraocular extension. Such tumors are generally larger and carry a worse prognosis.
DIAGNOSTIC APPROACHES
In most instances, the diagnosis of macular choroidal melanoma can be made by recognition of its classic features using indirect ophthalmoscopy. The diagnosis can be supported or confirmed, however, by the judicious use of ancillary studies such as fluorescein angiography, ultrasonography, or, in more difficult cases, fine-needle biopsy (3). In cases that are atypical ophthalmoscopically, these ancillary studies assume a more vital role in diagnosis. These techniques are discussed in detail in the literature (1,2) and are only summarized here.
 FIGURE 49-1. Pigmented choroidal melanoma encroaching on the foveal area. |
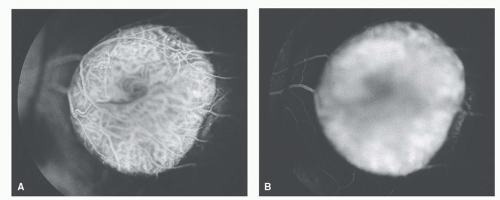 Figure 49-2. Fluorescein angiography of an elevated macular melanoma. A: Venous phase showing filling of the tumor vessels and the overlying retinal vessels (“double circulation”). B: Late angiogram showing diffuse hyperfluorescence of the mass. |
On fluorescein angiography, a typical choroidal melanoma shows mottled hyperfluorescence in the vascular filling phases and diffuse late staining of the mass and its overlying subretinal fluid. A larger melanoma, particularly one that has broken through Bruch’s membrane, shows more clearly the characteristic double circulation in which both the retinal vessels and the choroidal vessels in the tumor are evident (1,2) (Fig. 49-2).
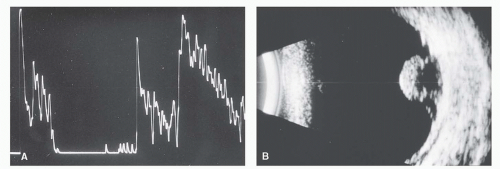 Figure 49-3. Ultrasonography of macular choroidal melanoma. A: a-Scan showing medium to low decreasing amplitude pattern. B: b-Scan showing pedunculated mass with basal acoustic hollowness and choroidal excavation. |
On A-scan ultrasonography, choroidal melanoma typically shows medium to low internal reflectivity; on B-scan, it shows a choroidal mass pattern with acoustic hollowness and choroidal excavation (Fig. 49-3). Ultrasonography can delineate small nodules of extraocular extension of the tumor. It is particularly helpful in eyes with opaque media. Computed tomography and magnetic resonance imaging can be used to visualize uveal melanoma and to completely delineate larger areas of orbital extension (1,2).
Fine-needle aspiration biopsy can be used diagnose choroidal melanoma in difficult cases that defy clinical diagnosis using less invasive measures (1, 2




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
