Purpose
To evaluate the impact of cataract surgery on subfoveal choroidal thickness and central retinal thickness in the elderly.
Design
Prospective observational case series.
Methods
This cohort study included 29 eyes of 29 patients with senile cataract, but no previous ocular surgery or other ocular abnormality. All 29 eyes received standard surgery by phacoemulsification and intraocular lens implantation. Subfoveal choroidal thickness and central retinal thickness were measured at baseline and 1, 3, and 6 months postoperatively by spectral-domain optical coherence tomography. Multiple regression analysis was conducted to identify predictors of larger changes in subfoveal choroidal thickness, including sex, age, baseline choroidal thickness, axial length, refractive status before surgery, and duration of surgery.
Results
The 29 patients with senile cataract received cataract surgery without complication. Mean subfoveal choroidal thickness was 193.8, 208.9, 210.2, and 209.3 μm at baseline and at postoperative 1, 3, and 6 months, respectively, with a statistically significant increase after surgery (repeated-measures ANOVA; P < .0001). In 20 eyes (69.0%), subfoveal choroidal thickness remained high even 6 months after surgery. Multiple regression analysis revealed that male sex ( P = .014) and thicker baseline choroid ( P = .0048) predicted larger increases in subfoveal choroidal thickness. In contrast, the tendency of transient increase in central retinal thickness was not statistically significant.
Conclusion
Most elderly patients with senile cataracts are expected to maintain increased subfoveal choroidal thickness for at least 6 months after cataract surgery.
Recent advances of enhanced depth imaging (EDI) using spectral-domain optical coherence tomography (SD OCT) enables the observation of the choroid with sufficient intra- and inter-observer agreement. SD OCT has revealed the importance of the change in choroidal thickness in numerous retinal and choroidal disorders, including central serous chorioretinopahthy, age-related macular degeneration (AMD), and diabetic retinopathy, but also physiological conditions including age, sex, axial length, refractive status, and circadian change.
Surgery for senile cataract is one of the most commonly performed ophthalmic surgeries, with significant importance for quality of vision in the elderly. Pseudophakic macular edema and Irvine-Gass syndrome are among the well-known complications of cataract surgery on the retina, though its pathogenesis has not been fully understood. Recently, retinal thickening after cataract surgery has been reported even in healthy eyes without definite morphologic change on SD OCT. Considering the close relationship between the retina and the choroid, it is worthwhile to address the relationship between choroidal thickness and cataract surgery. In addition, because choroidal thickness is considered to reflect the condition of choroidal vasculature, addressing the relationship may be of interest for the ongoing discussion on the possible association between cataract surgery and progression of AMD.
In this study we investigated, through SD OCT, the change in subfoveal choroidal thickness after cataract surgery in patients with senile cataract.
Patients and Methods
This study was conducted with the approval of the Instituitional Review Board of the University of Tokyo Hospital, and informed consents were received from all the enrolled patients. Following standard ophthalmologic examination, including best-corrected visual acuity (BCVA), dilated pupil ophthalmoscopy, and SD OCT imaging, 29 eyes of 29 consecutive patients were entered in this study. If both eyes were operated for their cataract during the study period, the first eyes were included for analysis. Exclusion criteria were eyes with histories of ocular diseases, including diabetic retinopathy, early or late AMD, retinal vein occlusion, uveitis, or other vascular and inflammatory retinal disorders. The evaluated eyes of the included patients could not have a history of prior ocular surgery for the entry to this study.
All examinations were conducted at the Department of Ophthalmology, University of Tokyo Hospital. BCVA and Spectralis SD OCT (Heidelberg Engineering Inc, Dossenheim, Germany) examinations and biomicroscopy were performed at baseline (before cataract surgery) and 1, 3, and 6 months postoperatively.
Cataract Surgery
Surgeries were performed between July 4, 2012 and January 6, 2013 by experienced surgeons using a standardized phacoemulsification technique. All surgeries were performed using INFINITI Vision System (Alcon Inc, Fort Worth, Texas, USA). After the phacoemulsification, the blue light–filtering intraocular lens was implanted in the bag. Complications including posterior capsule rupture, vitreous loss, prolapse through the wound, and iris trauma were exclusion criteria, although no patient enrolled experienced surgical complications. Postoperative treatment consisted of topical combination betamethasone/gatifloxacin and bromfenac eye drops for 4 weeks, followed by bromfenac eye drop for another 2 months. All patients experienced improvement in BCVA and no patients required further treatment for the development of macular edema and posterior capsule opacity during the observation period.
Spectral-Domain Optical Coherence Tomography
Central retinal thickness and subfoveal choroidal thickness were measured using SD OCT (Spectralis, wavelength: 870 nm; Heidelberg Engineering Co, Heidelberg, Germany) with EDI modality after pupil dilation. In the SD OCT, 100 frames were averaged together with the aid of eye tracking. Because the choroidal thickness shows circadian change, the patients were scheduled to be examined at the same time at each visit (within 1 clock hour difference). In the Spectralis SD OCT, a previously tracked image could be used as a reference to obtain new images at the same point of the fundus at each visit. A 6-mm horizontal section running through the center of the fovea with a quality score ≥25 was selected. The subfoveal choroidal thickness was measured manually using Heidelberg Eye Explorer software (version 5.4; Heidelberg Engineering Co). Two masked independent observers measured subfoveal choroidal thickness perpendicularly from the outer edge of the hyper-reflective retinal pigment epithelium (RPE) to the inner sclera at the fovea using Spectralis linear measurement tools. The inter-observer agreement was tested by Pearson correlation. The measurements from the 2 observers were then averaged together for analysis. Values of the central retinal thickness were those obtained through automated measurement by the machine.
Statistics
Changes in the subfoveal choroidal thickness and central retinal thickness after cataract surgery were analyzed by repeated-measures ANOVA and Bonferroni posttest. Peak postoperative values were compared to the baseline by paired t test. The magnitude of the change from baseline to the peak was analyzed with possible explaining variables by multiple regression model. A P value of less than .05 was considered statistically significant. Statistical analysis was performed by JMP 10 pro software (SAS Inc, Cary, North Carolina, USA).
Results
Twenty-nine eyes of 29 patients with senile cataract were included. Mean ± SD age of the patients was 73.0 ± 7.2 years, and 14 patients were male. Mean ± SD axial length was 23.6 ± 1.35 mm, and axial length in 5 eyes was more than 25 mm. All patients fulfilled the evaluation visits at baseline and after surgery.
There was no complication in the postoperative course of any patient. By 1 month postoperatively the inflammation indicated by cells or flare in the anterior chamber on slit-lamp microscopy disappeared in all patients. No cystoid macular edema or subretinal fluid developed, as evaluated by SD OCT. We also confirmed a favorable inter-observer agreement to measure subfoveal choroidal thickness on the OCT at baseline (Pearson correlation = 0.948, P < .0001).
The mean central retinal thickness of the 29 eyes at baseline and at postoperative1, 3, and 6 months was 222.7, 230.8, 225.9, and 224.7 μm, respectively ( Figure 1 ). Repeated-measures ANOVA did not indicate a statistical significance ( P = .468). Bonferroni posttest also did not show statistical significance for the tendency of the increased central retinal thickness at 1 month ( P = .165), 3 months ( P = .569), and 6 months ( P = .659) postoperatively.
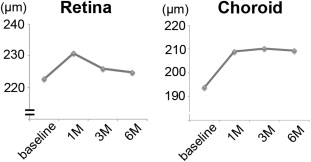
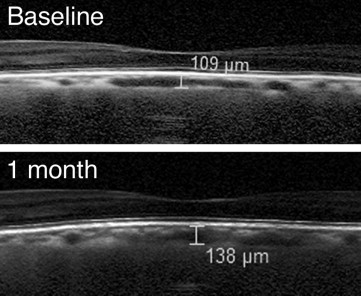
The mean subfoveal choroidal thickness of the 29 eyes at baseline and at postoperative 1, 3, and 6 months was 193.8, 208.9, 210.2, and 209.3 μm, respectively ( Figure 1 ). Figure 2 is an example of subfoveal choroidal thickness measurement before and after cataract surgery. Repeated-measures ANOVA indicated a statistical significance ( P < .0001). The Mauchly sphericity test did not reveal a problem ( P = .862), and consistent with this, sphericity adjustments by Greenhouse-Geisser Epsilon ( P < .0001) or Huyn-Feldt Epsilon ( P < .0001) did not change the statistical significance. Bonferroni posttest revealed that compared to the baseline, the choroid became thicker at each postoperative measurement: 1 month ( P < .0001), 3 months ( P < .0001), and 6 months ( P < .0001) postoperatively.
For 29 eyes the subfoveal choroidal thickness at baseline and at the postoperative peak were compared. The mean ± SD choroidal thickness at baseline for 29 eyes was 193.8 ± 82.5 μm and that of the postoperative maximum was 214.9 ± 90.2 μm. The difference was statistically significant ( P < .0001) by paired t test. In the 29 patients maximal subfoveal choroidal thickness was recorded at 1, 3, and 6 months postoperatively for 15 patients (51.7%), 8 patients (27.6%), and 6 patients (20.7%), respectively. To seek factors that could predict a larger amplitude of the change in subfoveal choroidal thickness (baseline to postoperative peak, μm), a multiple regression model was used ( Table ). The evaluated variables comprised age, sex, baseline choroidal thickness, axial length, refractive status before surgery, and the duration of surgery. The multiple regression analysis revealed that thicker baseline choroid ( P = .0048) and male sex ( P = .014) were significantly associated with a larger amplitude of increase in subfoveal choroidal thickness after cataract surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


