Purpose
To establish the growth behavior of small ciliary body tumors in a relatively large cohort of patients over an extended period.
Design
Retrospective, noncomparative case series.
Methods
Ciliary body tumors less than 4 mm in size within the penetration power of ultrasound biomicroscopy (UBM) were included. Tumor height was assessed by ultrasound biomicroscopy. Tumor growth was defined as an increase in height of at least 20% from baseline, as measured on 2 consecutive UBM readings. The data were collected longitudinally, and a statistical analysis was performed.
Results
Forty-two patients were included in the study with a median follow-up of 9.0 years (range, 1.0 to 17.2 years). The median age was 59 years (range, 17 to 82 years). Median initial tumor height was 2.05 mm (range, 1.11 to 3.80 mm). The overall average rate of growth was 0.0014 mm per year ( P = .68). The 5- and 10-year accumulative tumor growth rates were 12% and 29%, respectively. In the first 3 years after diagnosis, the growth rate of ciliary body lesions with an initial tumor thickness less than or equal to 2 mm was 0.054 mm per year ( P = 0.0001); thereafter, tumor size appeared to stabilize. Tumors with an initial thickness greater than 2 mm showed a small but significant rate of regression of 0.0125 mm per year ( P = 0.04).
Conclusions
Most small tumors of the ciliary body show little growth over an extended period and can be managed conservatively without invasive diagnostic interventions. However, long-term follow-up is required. Indications for treatment include growth in height or lateral extension, extrascleral extension or the need for cataract surgery.
The role of ultrasound biomicroscopy (UBM) in the detection and management of ciliary body and anterior segment lesions has been well documented. Tumors of the ciliary body can be difficult to manage. The differential diagnosis includes nevi, melanoma, melanocytoma, and rarer tumors such as leiomyoma, adenoma, adenocarcinoma, and medulloepithelioma. Ciliary body melanoma accounts for only 10% of all uveal melanoma, but has a worse prognosis compared with that of choroidal melanoma, with higher mortality rates resulting from metastasis. A new tumor–node–metastasis (TNM) classification system for uveal melanoma has recently been published. Although this system categorizes choroidal and ciliary body melanoma together, it grades ciliary body involvement with a worse prognosis. Therefore, early detection of ciliary body melanoma and distinguishing it from benign tumors in the ciliary body are important. Because of the hidden location of the ciliary body on clinical examination, these lesions often are not identified until they grow large enough to invade the anterior segment or produce symptoms. Where other methods may be limited, UBM is an effective tool in detecting these tumors and providing accurate estimations of size, location, and growth. UBM also can be used to evaluate internal tumor features, to define tumor margins in planning for both iridocyclectomy and plaque radiotherapy, and to monitor for recurrences after treatment.
In a previous study, we showed that small lesions of the ciliary body can be monitored closely with UBM without the need for invasive diagnostic interventions. Over a median follow-up of 4.3 years, it was evident that most small tumors of the ciliary body behave benignly, showing little growth over time. This is an extension of that study on 42 patients with ciliary body tumors of less than 4 mm (within the penetration power of UBM). Our goal is to establish the behavior of this relatively large cohort of patients over a median follow-up of 9.0 years.
Methods
We conducted a retrospective chart review of all patients with ciliary body tumors who were followed up at the Princess Margaret Hospital, Toronto, Canada, between April 1990 and December 2008. All patients with ciliary body tumors of a size within the penetration power of the ultrasound biomicroscope (less than 4 mm) were included in the study.
Cases were evaluated for the presence of sentinel vessels, tumor extension to the anterior chamber or iris, cataract, increased intraocular pressure induced by the tumor, and associated ocular inflammation. Any treatment instituted was documented.
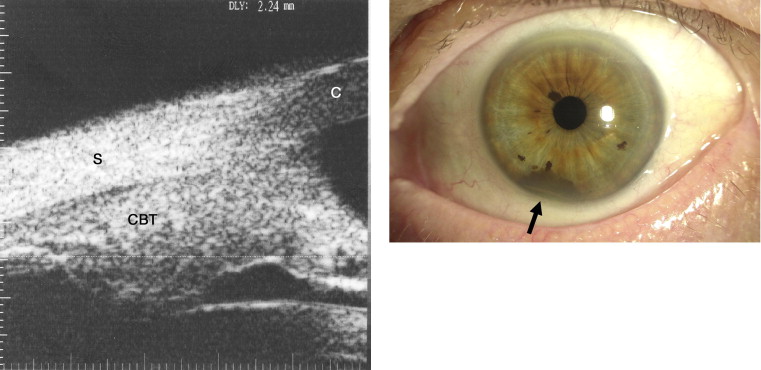
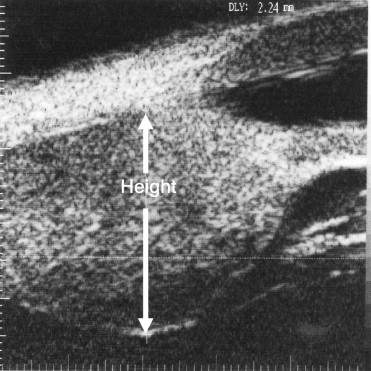
UBM was performed as previously described. The commercial version of the ultrasound biomicroscope with a 50-MHz transducer was used (Humphrey Instruments, San Leandro, California, USA). Radial sections through the greatest thickness of the tumor were obtained using an eye cup with 1% methyl cellulose. Tumors were considered as primarily ciliary body in origin when most of the tumor mass was in the ciliary body region ( Figure 1 ). Tumors with most of the lesion in the iris or choroid were considered primary iris or choroidal tumors, respectively, and were excluded. Height was measured from the internal surface of the sclera to the tumor surface at the thickest portion of the tumor ( Figure 2 ). The primary outcome measure was tumor growth, which was defined as an increase in tumor height of at least 20% from baseline, as measured on 2 consecutive UBM readings. For those receiving treatment, tumor size was evaluated until the time of treatment. Intraobserver and interobserver variability in the reproducibility of UBM measurements can be a factor depending on the definition of the structure measured and the experience of the ultrasonographer. A rate of 20% on 2 consecutive UBM measurements was chosen as a definition for growth to minimize any uncertainty resulting from measurement variability.
UBM characteristics, including the internal reflectivity, the internal structure, and features such as hyperechoic and hypoechoic patterns, the presence of cystic spaces, and the outer contour of the tumor, were characterized. Iris extension and anterior extension of the tumor relative to the scleral spur also were documented. These features were described in a previous study.
The data were collected longitudinally. The rate of tumor growth was estimated by using mixed model regression accounting for between-individual variation and within-individual variation. The same modeling technique was applied to estimate the rate of tumor growth in the first 3 years and that in subsequent years. The accumulative incidence of tumor growth was estimated by the Kaplan-Meier method where the event was defined as the increase in tumor height of 20% or more from baseline for 2 consecutive measurements. The time to growth was calculated from the start of follow-up to the first date that the growth, as defined earlier, was recorded. Differences between survival curves were analyzed by the log-rank test. A proportional hazard model was applied to assess the effect of continuous variables such as initial tumor height on tumor growth. Results were considered significant if the P value was .05 or less. The statistical analysis was performed using the SAS software version 9.1 (SAS Institute, Cary, North Carolina, USA).
Results
Forty-two patients with ciliary body tumors less than 4 mm in height were included. Clinical data are shown in Table 1 . The median follow-up was 9.0 years (range 1.0 to 17.2 years). The median age was 55.4 years. Twenty patients were male and 22 were female. Twenty-two were right eyes and 20 were left eyes. Other clinical data were available in all but 1 patient. At presentation, 4 patients had evidence of sentinel vessels, 19 patients had a unilateral cataract, and 2 patients had associated ocular inflammation (1 patient had scleritis and another had uveitis). The intraocular pressure was normal in all patients at presentation.
| Patient Data | Values |
|---|---|
| Demographic characteristics (n = 42) | |
| Follow-up (yrs) | |
| Median | 9.0 |
| Range | 1.0 to 17.2 |
| Age (yrs) | |
| Median | 55.4 |
| Range | 16.8 to 81.6 |
| Gender | |
| Male | 20 (47.6%) |
| Female | 22 (52.4%) |
| Eye | |
| Right | 22 (52.4%) |
| Left | 20 (47.6%) |
| Clinical findings (n = 41) a | |
| Sentinel vessels | 4 (9.8%) |
| Cataract | 19 (46.3%) |
| Associated ocular inflammation | 2 (4.9%) |
| Scleritis | 1 (2.4%) |
| Uveitis | 1 (2.4%) |
| Intraocular pressure | |
| Normal | 41 (100%) |
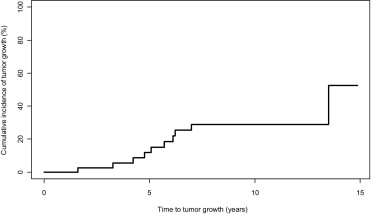
With UBM, the initial median tumor height was 2.05 mm (range 1.11 to 3.80 mm). The overall rate of growth was 0.0014 mm per year ( P = .68). The Kaplan-Meier curve for growth over time is shown in Figure 3 . By 5 years after diagnosis, 5 tumors (12%) demonstrated at least 20% growth from baseline as measured by UBM on 2 consecutive measurements. By 10 years, 9 tumors (29%) grew significantly. Overall, growth in height occurred in 10 tumors. The average time to growth was 5.4 years (range 1.6 to 13.5 years).
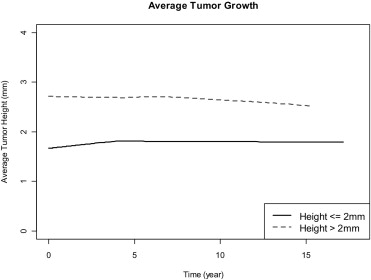
Smaller tumor height was a significant risk factor for growth ( P = .01). Tumors with an initial thickness less than or equal to 2 mm had a slow but significant rate of growth of 0.0154 mm per year ( P < 0.0001); whereas, tumors with an initial thickness greater than 2 mm showed a small but significant rate of regression of 0.0125 mm per year ( P = 0.04) ( Figure 4 ). Nine of the 19 smaller tumors (47.4%) progressed while only 1 of the 23 larger tumors (4.3%) progressed. However, the rate of growth for the smaller tumors was only significant in the first 3 years after diagnosis (0.054 mm per year; P = 0.0001), after which tumor size appeared to stabilize and the rate of growth was not significant (0.0044 mm per year; P = 0.22) ( Figure 4 ).
Ten patients were offered treatment over the course of follow-up ( Table 2 ). Nine patients had a larger initial tumor size (> 2 mm) and one patient had a smaller initial tumor size (≤ 2 mm). The median initial tumor height was significantly larger in patients offered treatment (2.67 mm; range 1.84 to 3.80 mm) versus those not offered treatment (1.91 mm; range 1.11 to 3.80 mm) ( P = 0.008). Four patients were offered treatment due to growth in tumor height. Three patients were offered treatment because of growth in base or a change in shape and volume of the tumor. One patient was offered treatment due to the presence of extrascleral extension on the initial examination. This patient declined and is still being followed almost 18 years after the initial presentation even though the intraocular and extraocular portions of the tumor have consistently grown. Finally, 2 patients were offered treatment before undergoing cataract surgery despite the stable size of the tumor.
| Treatment | Reason for Treatment | Pathologic Diagnosis | Treatment Time after Diagnosis (mos) |
|---|---|---|---|
| Offered treatment but declined | Extrascleral extension | 0 | |
| Brachytherapy | Height growth | 10 | |
| Iridocyclectomy | Height growth | Malignant melanoma of the ciliary body a | 13 |
| Iridocyclectomy | Change in shape and increase in volume of tumor | Choroidal nevus b | 14 |
| Brachytherapy | Treatment before cataract surgery | 14 | |
| Enucleation | Base growth (ring melanoma) | Malignant melanoma of the ciliary body c | 39 |
| Brachytherapy | Base growth (partial ring melanoma involving 5 clock hours of ciliary body) | 57 | |
| Brachytherapy | Height growth | 86 | |
| Offered brachytherapy at last follow-up | Height growth | 114 | |
| Brachytherapy | Treatment before cataract surgery | 123 |
a Predominantly spindle-cell type.
b Nevus with HMB-45 positivity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


