Purpose
To identify the characteristics that are associated significantly with visual field (VF) defects in highly myopic eyes.
Design
Retrospective, observational series.
Methods
The medical records of 492 eyes of 308 patients with high myopia (myopic refractive error > 8 diopters or axial length ≥ 26.5 mm) with a follow-up of 5 years or more were reviewed. The VFs were determined by Goldmann kinetic perimetry, and the VFs were quantified in 100 sectors within the V4 isopter. Eyes with loss of 10% or more of the sectors were classified as having significant VF defects, and a further loss of 10% or more during the follow-up period was classified as a significant progression. To avoid the influence of the posterior fundus changes resulting from the high myopia, eyes with any type of myopic macular or peripheral lesions that could cause visual field defects were excluded.
Results
Significant VF defects were newly developed in 13.2% of these selected highly myopic eyes during a mean follow-up ± standard deviation of 11.6 ± 5.5 years. The incidence of significant VF defects in myopic eyes was significantly higher in eyes with an oval optic disc than that in eyes with a round optic disc. An oval optic disc was present significantly more frequently in the myopic eyes with VF defects. Temporal and nasal VF defects were present in the same eye. Among the eyes with significant VF defect, the temporal VF defects were observed in 61.5% of the eyes with round discs, in 75.0% of the eyes with vertically oval discs, and in 68.2% of the eyes with obliquely oval discs. During a mean follow-up ± standard deviation of 10.2 ± 3.4 years, 73.8% of the eyes showed a significant progression of the VF defects. An abrupt change of the scleral curvature (types VII and IX staphyloma by Curtin) was the only factor significantly associated with a progression of the VF defects.
Conclusions
Because the VF defects are progressive, we suggest that high myopia is a high risk factor for VF defects and that these eyes be examined at least once yearly. The combination of stretching and distortion of the optic nerve fibers resulting from an abrupt change of scleral curvature may be the factors that lead to the damage of the optic nerve fibers in highly myopic eyes.
It is well known that visual field defects frequently are present in eyes with pathologic myopia. These visual field defects can be divided into 2 types: those that are the result of the chorioretinal lesions commonly found in highly myopic eyes, and those that are not associated with these lesions and have no identifiable cause. It has been suggested that the latter type of visual field defects may be the result of glaucoma, because recent studies have suggested that primary open-angle glaucoma can develop in myopic eyes, and a study of 64 394 Japanese individuals showed that there was a significant and positive association between the degree of myopia and the prevalence of open-angle glaucoma for a specific age and gender group. In the United Kingdom, the relative risk of glaucoma in eyes (n = 953) with myopia (spherical equivalent refractive error ≥ 5 diopters [D]) was 3.1. However, the relationship between glaucoma and high myopia remains questionable because the degree of myopia in the former study was not presented, and the classification of high myopia in the latter study was relatively low at −5.0 D or more.
A PubMed search identified only 2 studies that examined the prevalence of glaucoma in highly myopic eyes. Thus, Curtin reported that the incidence of primary open-angle glaucoma was 3% in myopes with an axial length of more than 26.5 mm and 28% in those with an axial length of more than 33.5 mm. In the second study, Xu and associates examined 122 eyes with myopic refractive errors of more than 8 D in the Beijing Eye Study and showed that 10 eyes (8.2%) had optic disc glaucoma, defined as a glaucomatous appearance of the optic disc, and 7 eyes (5.7%) had perimetric glaucoma, defined as eyes with a glaucomatous appearance of the optic disc and corresponding visual field defects. Thus, a glaucomatous appearance of the optic disc was a prerequisite for classifying an eye as having glaucoma. However, the appearance, that is, shape and orientation, of the optic disc frequently is abnormal in highly myopic nonglaucomatous eyes. It then would be difficult to determine whether glaucoma is present in these highly myopic eyes by the appearance of the optic disc. In addition, highly myopic eyes often have chorioretinal changes, for example, large myopic conus, patchy areas of chorioretinal atrophy, that can give rise to visual field defects. It then would be difficult to diagnose glaucoma based on the presence of visual field defects in highly myopic eyes.
Thus, the purpose of this study was to determine the characteristics of highly myopic eyes that develop visual field defects and also to determine the factors significantly associated with the visual field defects in these eyes, including those with extreme myopia. To avoid the influence of the posterior fundus changes resulting from the high myopia, eyes with any type of myopic macular and peripheral lesions that could cause visual field defects were excluded. We also analyzed only the areas within the V4 isopters of the Goldmann visual fields by modifying the method of Kwon and associates. We show that there was a high incidence (13.2%) of visual field defects in highly myopic eyes that could not be explained by the observed fundus lesions. The visual field defects were progressive, and multiple regression analysis showed that the presence of an abrupt change of scleral curvature was the only factor significantly associated with the progression of the visual field defects.
Methods
The medical records of the 2 eyes of 1175 consecutive patients with pathologic myopia (myopic refractive error > 8 D or axial length ≥ 26.5 mm) who were examined in our High Myopia Clinic from 1996 through 2005 were analyzed. The exclusion criteria were: peak intraocular pressure (IOP) of more than 21 mm Hg, use of antiglaucoma medication at the initial examination, history of optic neuritis or other neuro-ophthalmologic diseases, any type of myopic macular or peripheral lesions that could cause visual field defects such as atrophic or pigmented punched-out chorioretinal lesions; choroidal neovascularization; peripheral chorioretinal lesions; history of vitreoretinal surgery, glaucoma laser surgery, or glaucoma incisional or filtration surgery; and follow-up period of less than 5 years after the initial visit.
The visual fields were examined with the refractive errors corrected by disposable soft contact lenses. The astigmatic refractive errors were corrected by spectacles if they were more than 1 D after wearing soft contact lenses. The Goldmann visual fields were quantified using a grid system similar to that used by Kwon and associates ( Figure 1 ). A grid template was adapted from the visual field scoring system originally described by Esterman. This grid consisted of 100 sectors that lay within the V4 isopter. The grid template was drawn on a transparent piece of paper that was laid over the visual field findings, each sector detected was marked with a dot, and the number of dots that fell in but not on or outside the V4 isopter were counted. The number of dots in the entire area and in the nasal superior, nasal inferior, temporal superior, and temporal inferior quadrants was counted. The same grid template was used for the fellow eye by simply turning it over.
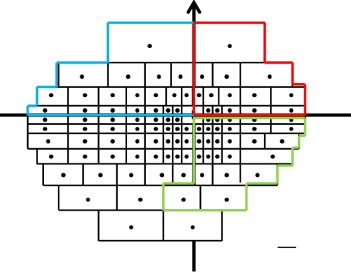
The visual field score ranged from 0, a total loss of vision within the V4 isopter, to 100, a full visual field. The final score was expressed as a percentage of the normal field. We considered that eyes with a loss in more than 10 of the sectors or more than 10% of the dots in each field had significant visual field defects. Patients who already had significant visual field defects at the initial examination were excluded. The defects in the visual field were quantified for the entire visual field and for each quadrant. There were 19 sectors in the superior nasal quadrant, 14 in the superior temporal, 27 in the inferior temporal, and 40 in the inferior nasal quadrant ( Figure 1 ). The lowest sector along the vertical line was assigned to the inferior temporal quadrant, and the second lowest sector along the vertical line was assigned to the inferior nasal quadrant ( Figure 1 ).
All patients underwent a complete ophthalmic evaluation, including manifest refractive error (spherical equivalent), best-corrected visual acuity, visual fields with a Goldmann perimeter, IOP measurements with Goldmann applanation tonometer, and detailed ophthalmoscopic examinations. The IOP measurements were made between 2:00 pm and 5:00 pm in all patients. The axial length of the eye was measured by A-scan ultrasonography (Ultrascan; Alcon, Fort Worth, Texas, USA) at least 10 times for each eye, and the average value was used for the statistical analyses. Before each recording, the A-scan Ultrascan was calibrated for accuracy against a standard length. For each ultrasonographic measurement, we confirmed the presence of 4 sharp spikes corresponding to the surface of the cornea, the front and back surfaces of the lens, and the surface of the retina.
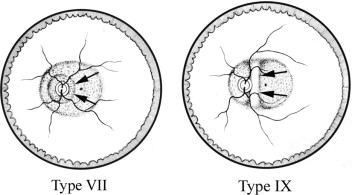
The type of posterior staphyloma was determined by its location and was classified by binocular stereoscopic ophthalmoscopy. The staphylomas were classified into 10 types: types I through V were primary staphylomas, and types IV through X were compound staphylomas ( Figure 2 ). We paid special attention to any abrupt changes in the scleral curvature temporal to the optic disc because our early observations suggested that these abrupt changes may be related to the visual field defects. An abrupt change of scleral curvature temporal to the optic disc was observed in all eyes with type VII and IX staphylomas ( Figure 2 ). The determination of a posterior staphyloma was based on a complete agreement of 3 of the authors (K.O.-M., N.S., M.M.).
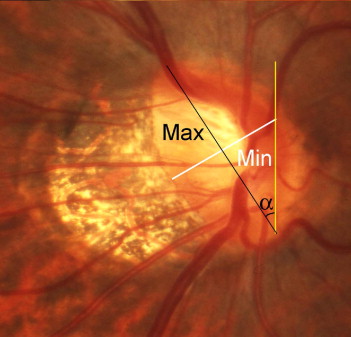
We also analyzed the shape and orientation of the optic disc. The ovalness of the disc was determined by calculating the ratio of the maximum diameter to the minimum diameter (Mx/Mn ratio; Figure 3 ). When the Mx/Mn ratio of the optic disc was more than 1.5, the optic disc was defined as an oval disc, and a disc with an Mx/Mn ratio of 1.5 or less was defined as a round disc. The oval discs were subdivided into vertically oval, with the major axis ± 10 degrees of the vertical meridian; horizontally oval, with the major axis ± 20 degrees of the horizontal meridian; and obliquely oval, with the major axis between 11 and 69 degrees.
Magnetic resonance imaging was performed on the patients who agreed to have this examination to rule out the presence of intracranial lesions.
Statistical Analyses
The relationship between the optic disc shape and visual field defects was analyzed using chi-square tests. The differences in the patient’s age, myopic refractive error, axial length, IOP, the degree of the ovalness of optic disc, and the presence of an abrupt change of scleral curvature temporal to the optic disc for those with and without visual field defects were analyzed by Mann–Whitney U tests. Multiple regression analyses also were performed to determine the correlations between these factors and the visual field score. Multiple linear regression analyses were used to determine whether the progression of the visual field defects per year was associated significantly with 6 possible factors: age at the initial examination, age at the last examination, axial length, initial IOP, mean IOP during the follow-up, Mx/Mn ratio of the optic disc, and the presence of an abrupt change of scleral curvature temporal to the optic disc. Because the refractive error was correlated significantly with the axial length (Spearman correlation coefficient, r = −0.595; P < .001), only the axial length was analyzed as a potential factor associated with the progression of visual field defects. For patients with bilateral visual field defects, data from only the right eye were used for the statistical analyses. A P value of less than .05 was considered statistically significant.
Results
From the 2 eyes of 1175 patients, 1858 eyes were excluded: 1269 eyes because their follow-up period was less than 5.0 years; 281 eyes that already had significant visual field defects at the initial examination; 20 eyes that were being treated with antiglaucoma medication at the initial examination; 18 eyes that had severe cataracts that prevented a detailed observation of the optic disc; 149 eyes for a choroidal neovascularization; and 52 eyes with other retinal pathologic features, for example, chorioretinal atrophy and retinal detachments, that could cause visual field defects. In addition, 43 eyes were excluded because of the presence of peripheral pigmentary changes mimicking retinitis pigmentosa, and 15 eyes because of visual field defects resulting from the presence of a brain infarction. Eleven eyes were excluded because of prior vitreoretinal surgery.
In the end, 492 eyes of 308 patients with high myopia met our inclusion criteria. There were 122 men (204 eyes) and 186 women (288 eyes). The mean age ± standard deviation (SD) was 40.6 ± 16.6 years (range, 8 to 78 years). The mean refractive error ± SD was −13.4 ± 4.1 D (range, −8.25 to −30.0 D), and the mean axial length ± SD was 28.6 ± 1.7 mm (range, 26.6 to 33.0 mm). The mean IOP ± SD at entry was 14.7 ± 2.4 mm Hg (range, 8 to 21 mm Hg). Among the 492 eyes, in 65 eyes (13.2%) of 44 patients, significant visual field defects developed: loss of sensitivity in 10% or more of the sectors in 1 or more quadrants, during a mean follow-up ± SD of 11.6 ± 5.5 years (range, 6 to 30 years). Significant visual field defects were detected in the superior temporal field in 52 eyes, in the inferior temporal field in 42 eyes, in the superior nasal field in 42 eyes, and in the inferior nasal field in 37 eyes. One eye had a change in 2 quadrants, 13 eyes had a change in 3 quadrants, and 33 eyes had a change in 4 quadrants. All of the 44 patients received antiglaucoma medication after the development of significant visual field defects. The average number of medications ± SD during the follow-up was 1.2 ± 0.4 (range, 1 to 3). Magnetic resonance imaging scans, obtained within ± 1 month after the development of VF defects, were available in the medical records of 25 of the 44 (56.8%) patients, and none of them showed a presence of intracranial lesion that would have caused the visual field defect.
Among the 492 eyes, the optic disc was round in 322 eyes (65.4%) and oval in 170 eyes (34.6%). In the 170 eyes with oval optic discs, 84 eyes were vertically oval, 8 were horizontally oval, and 78 eyes were obliquely oval. The correlations between the optic disc shape and visual field defects are shown in Table 1 . In the 427 eyes without significant visual field defects, the round disc type was found significantly more frequently than the oval disc type, whereas in the 65 eyes with significant visual field defects, the oval disc was found significantly more frequently than the round disc ( P < .0001, chi-square test).
| Optic Disc Shape | Significant Visual Field Defects | |
|---|---|---|
| Absent (427 Eyes) | Present (65 Eyes) | |
| Round | 296 eyes (69.3%) | 26 eyes (40.0%) |
| Oval | 131 eyes (30.7%) | 39 eyes (60.0%) |
| Horizontal (oval) | 8 eyes (1.9%) | 0 eyes (0%) |
| Vertical (oval) | 64 eyes (15.0%) | 20 eyes (30.8%) |
| Cyclotorted (oval) | 59 eyes (13.8%) | 19 eyes (29.2%) |
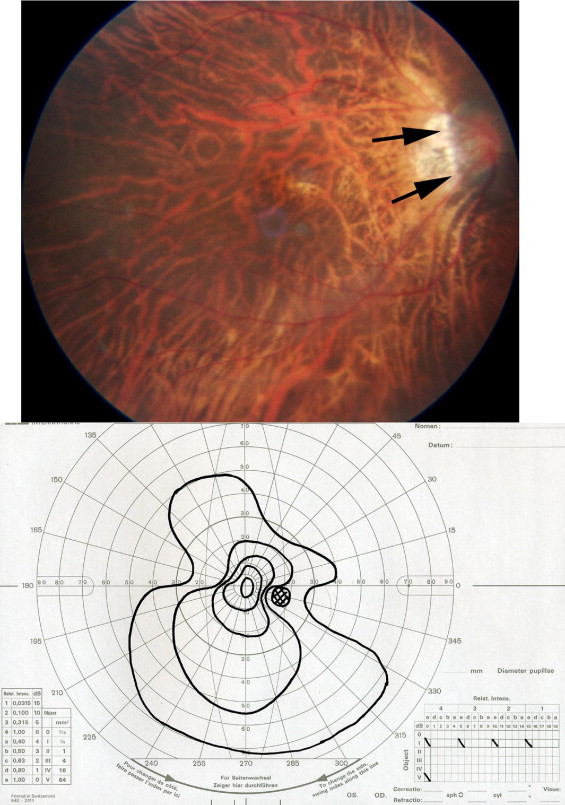
The incidence and the sites of the visual field defect in eyes with different optic disc shapes are shown in Table 2 . Because there were only 8 eyes with a horizontally oval optic disc, this type was not analyzed further. Among the eyes with significant visual field defects, 53.8% of the eyes with round optic discs, 65.0% of the eyes with vertically oval discs, and 52.6% of the eyes with obliquely oval discs had both temporal and nasal visual field defects, and the visual fields had a gourd-like shape ( Figure 4 ).
| Optic Disc Shape | |||
|---|---|---|---|
| Round (322 Eyes) | Vertical Oval (84 Eyes) | Oblique Oval (78 Eyes) | |
| Prevalence of significant visual field defects | 26 eyes (8.8%) | 20 eyes (23.8%) | 19 eyes (24.4%) |
| Area of significant visual field defects | |||
| Nasal only | 10 eyes (38.5%) | 5 eyes (25.0%) | 6 eyes (31.6%) |
| Temporal only | 2 eyes (7.7%) | 2 eyes (10.0%) | 3 eyes (15.8%) |
| Both nasal and temporal | 14 eyes (53.8%) | 13 eyes (65.0%) | 10 eyes (52.6%) |
Next, we analyzed the factors that may be associated significantly with the visual field defects in eyes with an oval disc ( Table 3 ). A comparison of the clinical characteristics between eyes with and without visual field defects showed that the patients with visual field defects were significantly older, had significantly higher IOPs, had more oval optic discs, and more frequently had an abrupt change of scleral curvature temporal to the optic disc at the time when the visual field defect developed. The results of multiple regression analysis supported these results ( Table 4 ).
| Factors at the Development of Visual Field Defects | Without Visual Field Defect (123 Eyes) | With Visual Field Defect (39 Eyes) | P Value |
|---|---|---|---|
| Age (years) | 43.7 ± 15.3 | 52.7 ± 14.9 | .006 a |
| Refractive error (D) | −14.9 ± 4.8 | −14.5 ± 4.5 | NS |
| Axial length (mm) | 29.1 ± 1.9 | 29.1 ± 1.5 | NS |
| Intraocular pressure (mm Hg) | 14.4 ± 2.5 | 15.7 ± 2.4 | .006 a |
| Ratio of maximum to minimum diameter of the optic disc | 1.6 ± 0.4 (1.2 to 3.0) | 2.0 ± 0.5 (1.5 to 4.0) | < .001 a |
| Sudden change of scleral curvature temporal to optic disc | 19/123 | 14/39 | .01 b |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


