Purpose
To compare long-term outcomes of full-bed deep lamellar keratoplasty (DLK) with penetrating keratoplasty (PK) for treating corneal leucoma caused by herpes simplex keratitis (HSK).
Design
Retrospective, comparative, interventional case series.
Methods
setting: Institutional. patients: Inclusion criteria were patients with corneal scarring induced exclusively by HSK who underwent primary graft of full-bed DLK or PK and completed a minimum of 12 months postoperative follow-up. There was no significant difference of corneal scarring and vascularization between the 2 groups before surgery. Choosing PK or full-bed DLK depended on the patient’s own willingness, except those patients with a preoperative endothelial cell count of less than 700 cells/mm 2 or whose endothelial cell count was undetectable were encouraged to undergo only PK. Exclusion criteria were patients with a past history of corneal perforation, nonprimary graft, non–HSK-related corneal scars, and failure to complete a minimum of 12 months of postoperative follow-up. Fifty-eight eyes of 58 patients in the full-bed DLK group and 63 eyes of 63 patients in the PK group met the inclusion criteria. main outcome measures: Postoperative managements, recurrence of HSK, graft rejection, graft survival rate, visual acuity, and corneal endothelial density.
Results
The mean postoperative follow-up duration was 45.8 ± 30.9 months in the full-bed DLK group and 47.9 ± 27.2 months in the PK group ( P = .70). As compared with the PK group, the full-bed DLK group experienced earlier suture removal ( P = .01), needed fewer postoperative visits ( P < .001), and had a higher proportion of eyes with full withdrawal of oral acyclovir ( P < .001) and topical corticosteroid ( P < .001). There were a total of 21 episodes of recurrent HSK in the PK group, more frequent than the 7 episodes in the full-bed DLK group, among which recurrent epithelial keratitis amounted to 13 episodes in the PK group, remarkably more frequent than the 1 episode in the full-bed DLK group. Twenty-six eyes (41.3%) encountered rejection episodes in the PK group, but no rejection episode was found in the full-bed DLK group ( P < .001). In 14 eyes in the PK group, graft failure developed because of graft rejection, recurrence of HSK, or both, whereas only in 1 eye in the full-bed DLK group did graft failure develop because of recurrence of HSK ( P = .001). The clear graft survival rate in the full-bed DLK group was significantly higher than that in the PK group ( P = .01). Corneal endothelial cell density was stable from 1 month through 5 years in the full-bed DLK group, but 51.3% cell loss was found in the PK group at 5 years after surgery. At the last visit, 66.1% of eyes with full-bed DLK grafts and 50.9% of eyes with PK grafts achieved a best-correct visual acuity of 0.5 or better ( P = .10).
Conclusions
Advantages of full-bed DLK over PK are no allograft rejection, longer graft survival, earlier drug withdrawal of topical steroid and oral acyclovir, less recurrence of HSK, and fewer follow-up visits. Full-bed DLK is preferable for treating HSK-induced corneal scarring with relatively healthy endothelium and with no history of perforation.
Herpes simplex keratitis (HSK) commonly causes recurrence and leads to severe corneal scarring. For recovering corneal clarity and rehabilitating visual acuity, corneal transplantation is needed. Penetrating keratoplasty (PK) is a conventional surgical procedure for treating HSK-induced corneal leucoma. However, after PK, although oral acyclovir helps decrease recurrence of HSK, graft rejection and chronic endothelial cell loss are still risks threatening graft survival. Conventional lamellar keratoplasty can avert postoperative rejection, but is not an ideal surgical procedure for treating HSK-induced corneal leucoma, because the technique usually creates irregular graft–recipient interface, leading to unsatisfactory transparency recovery and possibly higher frequency of herpetic recurrence in the graft. However, a comparatively new surgical procedure of deep lamellar keratoplasty (DLK) has been practiced in recent years. In DLK, pathologic stroma of the cornea can be removed as much as possible, and in a certain percentage of the patients, Descemet membrane can even be exposed in the optical area. Corneal clarity recovery can thence be achieved in DLK as ideally as in PK. Therefore, DLK may be an alternative to PK in treating HSK-induced corneal leucoma. A remarkable advantage of DLK over PK is that there is no postoperative endothelial rejection, because the recipient corneal endothelial layer is retained in situ for donor corneal grafting of DLK. Moreover, instead of donor cornea with healthy endothelium that is always required for PK, cryopreserved donor cornea without endothelium can be used for DLK.
For achieving the ideal excision of recipient corneal stroma as thoroughly as possible, several surgical techniques have been developed for DLK grafting in recent years. We previously developed a stromal-hooking and viscoelastic-detaching technique that enables removal of recipient stroma from the Descemet membrane in a single layer, unlike the techniques reported by others, in which stroma is excised layer by layer through a hard instrument dissecting procedure to approach the Descemet membrane. Using our hooking and soft viscoelastic detaching technique, the average surgical time is shortened to almost 1 hour, and the full layer of recipient stroma can be removed from Descemet membrane, extending the whole recipient bed rather than it remaining in the optical area only. We therefore named our surgical procedure full-bed deep lamellar keratoplasty (DLK), as described elsewhere. To exclude completely the possibility of immunologic rejection, we always use cryopreserved donor corneal button tissue without live cells in the tissue for DLK grafting, because fresh donor button tissue may induce epithelial and stromal rejection, even in DLK. In the present study, we investigated the advantages of full-bed DLK as compared with PK for treating HSK-induced corneal leucoma and evaluated the long-term postoperative outcomes in these 2 surgeries.
Methods
Patients
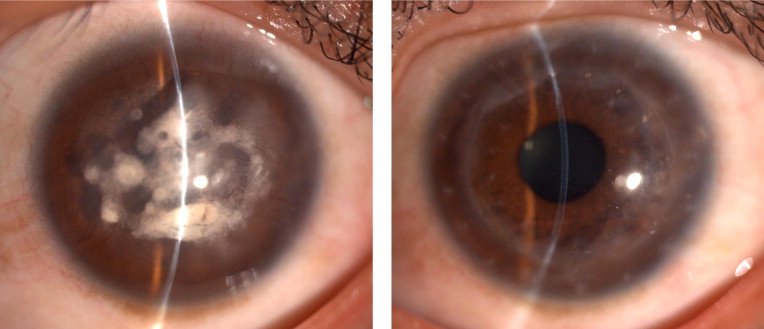
From April 2000 through October 2009, patients who had exclusively HSK-induced corneal scarring and underwent primary graft of full-bed DLK using Yao’s hooking-and-detaching technique or had received a primary graft of PK were reviewed through our database and were analyzed retrospectively. The diagnosis of HSK was made on the basis of typical recurrence in history, characteristics of clinical manifestations such as episodes of epithelial dendritic or geographic ulcer, typical stromal inflammatory edema with or without a cluster of keratic precipitates, which had good response to oral acyclovir or in combination with topical or systemic use of corticosteroid. Inclusion criteria were patients who had HSK-induced corneal leucoma ( Figure 1 , Left) and underwent primary graft of full-bed DLK or PK with a minimum of 12 months of postoperative follow-up. Exclusion criteria were patients with HSK-induced corneal leucoma with a history of corneal perforation; those who did not receive a graft by a primary transplant; those whose corneal scarring was not the result of herpes simplex virus infection, but suspiciously was the result of herpes zoster virus infection or other causes instead; and those who failed to complete a minimum of 12 months postoperative follow-up. Fifty-eight patients (58 eyes) who underwent full-bed DLK and 63 patients (63 eyes) who underwent PK met the inclusion criteria.
Before surgery, each patient was given a full explanation regarding potential advantages and disadvantages of full-bed DLK and PK for treating the corneal leucoma. With regard to the disadvantages of full-bed DLK, we especially emphasized the possible risks of perforation or rupture in Descemet membrane that may occur during surgery, in which a subsequent secondary PK may be necessary for the patient because of lack of fresh donor cornea readily available. Slit-scanning confocal microscopy (Confosan 2 or Confosan 3; Nidek Co., Ltd, Gamagori, Aichi, Japan), mostly carried out through the nonscarring or less severe scarring area in the periphery of the cornea, was performed routinely for all patients to evaluate the endothelial cell count. If the corneal endothelial cell count was less than 700 cells/mm 2 or was undetectable, the patients were encouraged to undergo only PK rather than full-bed DLK. Otherwise, the choice of surgical approaches depended on the patient’s own willingness.
Surgical Methods
All surgeries were performed by the same surgeon (Y.-F.Y.). Full-bed DLK was performed using Yao’s hooking-and-detaching technique ( Supplemental Video , available at AJO.com ). In brief, after trephination using a trephine 7.25 to 8.25 mm in diameter, a small area of Descemet membrane exposure was created first as a pocket in the recipient bed at 12 o’clock around the trephined margin by hooking the stromal fibers with a concave forceps tip, through which viscoelastic material was injected between the stromal layer and Descemet membrane, and the full stroma layer was detached from Descemet membrane extending to the full bed around the trephined margin. Stroma thereafter was removed in a single layer, making a complete exposure of Descemet membrane in the full bed. If the primary pocketing exposure did not exactly reach the very layer of Descemet membrane, a second or third round of the hooking-and-detaching process was required until the total stroma was removed in layers and Descemet membrane was exposed in the full bed. A donor corneal button 0 to 0.5 mm oversize, obtained from a cryopreserved eye stored at −20 C, from which epithelial cells and endothelial cells debris were scraped off by a sponge, but Descemet membrane was not stripped off from the donor, was sutured into the recipient bed. The recipient–graft junction was fixed either by a continuous 10-0 nylon suture or by 16 bites of interrupted 10-0 nylon sutures. The sutures were removed selectively based on refractive astigmatism and guided by topography.
In PK, a standard surgical procedure was used in all cases. The recipient bed was created by trephination using a trephine 7.25 to 8.0 mm in diameter. A fresh donor button, 0 to 0.50 mm oversize, preserved in a moist chamber, was used for PK grafting. During surgery, if an obvious cataract was observed after removing the recipient central cornea, a triple procedure of PK combined with extracapsular cataract extraction and intraocular lens implantation was performed in the PK group. In 1 eye, a preliminarily planed full-bed DLK was switched to PK because of large Descemet membrane tear occurred during surgery, which was included into the PK group for analysis. The recipient–graft junction was fixed either by a continuous 10-0 nylon suture or by 16 bites of interrupted 10-0 nylon sutures. The sutures were removed selectively based on refractive astigmatism and were guided by topography.
Postoperative Treatment and Follow-Up
Eyes in the full-bed DLK group were administered 0.3% ofloxacin or 0.5% levofloxacin (Santen Pharmaceutical Co., Osaka, Japan) and 0.1% fluorometholone (Santen Pharmaceutical Co.) eyedrops 4 times daily. The PK group was treated with 0.1% dexamethasone sodium phosphate combined with 0.3% tobramycin eyedrops (TobraDex; Alcon, Fort Worth, Texas, USA) 4 times daily. Topical steroids were used for at least 12 months and were tapered off according to the clinical outcome in both groups. All patients received oral acyclovir 200 mg 5 times daily in the first 3 months, which then were tapered to 400 mg twice daily for a further 12 to 18 months. If intraocular pressure (IOP) increased, TobraDex eyedrops was switched to 0.1% fluorometholone eyedrops 4 times daily. If adjustment of topical steroids did not work, topical antiglaucoma medication was added. Rejection episodes were treated with TobraDex eyedrops every 1 to 2 hours, which were tapered off over several weeks, depending on the clinical response, and meanwhile the oral acyclovir dose was adjusted from 200 to 400 mg 5 times daily and was tapered off over 6 to 8 weeks thereafter. Recurrence of herpes simplex epithelial keratitis was treated by oral acyclovir 200 mg 5 times daily only. Recurrence of herpes simplex stromal keratitis was treated by oral acyclovir 200 mg 5 times daily, together with 0.1% fluorometholone eyedrops 5 times daily, and in some more severe cases, oral dexamethasone 0.75 mg twice daily was initiated. When rejection and recurrence of HSK occurred simultaneously, the dosage of oral acyclovir was increased to 400 mg 5 times daily, and oral dexamethasone 0.75 mg twice to thrice daily or oral cyclosporine A 50 mg thrice daily sometimes was initiated with topical application of corticosteroid eyedrops, according to the specific clinical circumstances of the case.
All patients who underwent full-bed DLK or PK were scheduled to be followed up at 0.5, 1, 3, 6, 12, 18, and 24 months after surgery and every year after surgery thereafter. At each visit, a detailed clinical examination was performed, including uncorrected visual acuity, best-corrected visual acuity (BCVA), graft clarity, IOP, secondary glaucoma, development of cataract, rejection episodes, and recurrence of HSK. Patients were seen at shorter intervals or in an emergency based on clinical necessity.
Major Measurements
Vascularization of the recipient cornea was graded from 0 through 4, as described by a previous report. All intraoperative and postoperative complications were reviewed. Graft rejection was defined as development of an epithelial or endothelial rejection line or characteristic keratic precipitates, spreading corneal edema with cell infiltration in the stroma in a previously clear graft with normal thickness, a unilateral anterior chamber inflammatory reaction, or keratic precipitates limited to the previously clear graft. Recurrence of HSK was described as epithelial, stromal, or endothelial disease. Diagnosis of epithelial recurrence of HSK was based on clinical characteristics of a dendritic or a geographic ulcer, or a nonhealing epithelial defect that responded only to antiviral therapy. Differentiation of recurrence of herpetic stromal keratitis or herpetic endotheliitis from stromal and endothelial rejection sometimes is difficult, but if the initial location of corneal edema or lines or cluster of keratic precipitates, or both, can be identified, such as if the earliest abnormality of inflammation and edema occur in the host side spreading to the donor graft, this indicates herpetic recurrence, whereas if the earliest location of abnormality and lesion center were in the donor graft, this indicates rejection. Only the initial rejection episode and recurrence episode were used in the database for statistical computation. Graft failure was defined as an irreversible edema and cloudiness of the graft. The cause of graft failure was defined by the most closely related temporal event or series of events leading to the loss of central corneal clarity. High IOP was defined as eyes with normal preoperative IOP but with increased IOP of more than 21 mm Hg after surgery. Secondary glaucoma was defined as eyes with uncontrollable high IOP, needing continuous topical antiglaucoma medication for more than 3 months or even needing trabeculectomy for controlling the IOP. Complicated cataract was diagnosed when crystal lens turned out to be opaque after surgery.
Slit-scanning confocal microscopy was performed at 1, 3, 6, and 12 months after surgery and every year thereafter. Measurement of cellular density was analyzed using a software provided by the manufacture (Navis 3.1.0; Nidek Co., Ltd). Corneal endothelium density was counted and averaged from 3 central confocal images of an area of 0.05 mm 2 . The corneal endothelial cell loss was calculated as the decrease of cell density from 1 month to 1 year, 2 years, 3 years, 4 years, or 5 years after surgery, expressed as a percentage of the 1-month cell density.
Statistical Analyses
All data sets were tested for normality with the Kolmogorov-Smirnov test. The Pearson chi-square test, independent t test, and Mann–Witney U test were used, respectively, to investigate differences in categorical variables, normally distributed variables, and nonnormally distributed continuous variables. Kaplan-Meier survival analysis and the log-rank test were used to compare rejection-free, recurrence-free, and graft survival in the 2 groups. All tests were 2-tailed, and a P value of less than .05 was deemed statistically significant.
Results
General Characteristics
One hundred twenty-one eyes of 121 patients met the inclusion criteria for this study. Among them, 58 eyes received full-bed DLK grafts; 63 eyes received PK grafts, of which 18 eyes underwent a triple procedure of PK with cataract removal and intraocular lens implantation. Table 1 summarizes the general characteristics of the patients in the full-bed DLK and PK groups. Before surgery, no statistical significance was found between the 2 groups regarding gender, disease history, corneal scarring, and vascularization of recipient cornea ( Figure 1 , Left) and binocular morbidity rate. The mean age was 42.4 ± 13.0 years in the full-bed DLK group and 48.8 ± 16.2 years in the PK group ( P = .02). Both groups had a comparable mean postoperative follow-up period of approximate 4 years, during which the mean frequency of visits was significantly less in the full-bed DLK group (8.7 ± 3.8 times) than in the PK group (14.3 ± 7.0 times; P < .001). After surgery, the time for complete suture removal of the grafts was significantly earlier in the full-bed DLK group (12.9 ± 6.0 months; Figure 1 , Right) than that in the PK group (20.0 ± 13.9 months; P = .01). At the final visit, full withdrawal of oral acyclovir was found in 79.3% eyes in the full-bed DLK group, which was significantly higher than the 41.3% eyes in the PK group ( P < .001), together with full withdrawal of topical steroids in 72.4% eyes in the full-bed DLK group, which also was significantly higher than the 34.9% eyes of the PK group ( P < .001).
| Full-Bed DLK (n = 58) | PK (n = 63) | P Value | |
|---|---|---|---|
| Mean age ± SD (years) | 42.4 ± 13.0 | 48.8 ± 16.2 | .02 |
| Sex (male, female) | (37, 21) | (44, 19) | .48 a |
| Binocular morbidity (yes, no) | (16, 42) | (16, 47) | .79 a |
| Mean disease duration ± SD (years) | 11.9 ± 10.8 | 15.7 ± 13.4 | .10 b |
| Mean vascularization grade ± SD | 1.2 ± 1.1 | 0.9 ± 0.8 | .22 b |
| Mean follow-up ± SD (months) | 45.8 ± 30.9 | 47.9 ± 27.2 | .70 |
| Mean time to suture removal ± SD (months) | 12.9 ± 6.0 | 20.0 ± 13.9 | .01 |
| Mean visits of postoperative follow-up ± SD (times) | 8.7 ± 3.8 | 14.3 ± 7.0 | < .001 |
| Eyes stopping oral acyclovir at last visit (%) | 79.3 | 41.3 | < .001 a |
| Eyes stopping topical steroid at last visit (%) | 72.4 | 34.9 | < .001 a |
Recurrence of Herpes Simplex Keratitis
Characteristics of postoperative HSK recurrence in the 2 groups are summarized in Table 2 . Six eyes (10.3%) in the full-bed DLK group and 13 eyes (20.6%) in the PK group encountered recurrence episodes ( P = .12). The frequency of recurrence was 21 episodes in the PK group, which is remarkably higher than the 7 episodes in the full-bed DLK group. Recurrence-free survival was 96.6% at 1 year, 93.9% at 2 years, and 85.7% at 3 to 8 years in the full-bed DLK group, which is better than that in the PK group, in which recurrence-free survival was 88.9% at 1 year, 85.1% at 2 years, 77.9% at 3 to 7 years, and 62.3% at 8 years ( P = .15, log-rank test; Figure 2 ) . In the full-bed DLK group, in only 1 eye (1.7%) did graft failure develop as a result of HSK recurrence leading to corneal scarring. By contrast, in the PK group, graft failure developed in 5 eyes (7.9%) because of HSK recurrence.
| Full-Bed DLK | PK | P Value | |
|---|---|---|---|
| Total eyes receiving grafts, n | 58 | 63 | |
| Eyes with Recurrent HSK, n (%) | 6 (10.3) | 13 (20.6) | .12 |
| Total episodes of recurrent HSK in the grafts, n | 7 | 21 | |
| Recurrent episodes of different types of HSK | |||
| Epithelial keratitis, n | 1 | 13 | |
| Stromal keratitis, n | 5 | 6 | |
| Endotheliitis and keratouveitis, n | 1 | 2 | |
| Eyes deemed graft failure with scarring resulting from recurrent HSK, n (%) | 1 (1.7) | 5 (7.9) | .21 |
| Mean time to first recurrent HSK ± SD (months) | 21.3 ± 10.2 | 19.9 ± 24.9 | .89 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


