Lacrimal Disorders
Dacryoadenitis
Andrew Mick
ICD-9: 375.00
THE DISEASE
Pathophysiology
Dacryoadenitis is a disease characterized by inflammation and enlargement of the lacrimal gland and surrounding tissues. Depending on the clinical characteristics and etiology, it is classified as acute, chronic, or granulomatous.
Etiology
Underlying causes of dacryoadenitis include infectious diseases, inflammatory disorders, malignancies, and benign enlargements.
Acute Dacryoadenitis
Andrew Mick
ICD-9: 375.01
THE DISEASE
The Patient
Clinical Symptoms
Sudden onset of pain in the superior temporal orbit
Upper temporal eyelid is swollen, red, and tender to touch (Fig. 11-1)
Secondary conjunctival injection and symptoms of eye irritation and tearing
Double vision in attempted superior gaze in severe cases
Clinical Signs
Unilateral more commonly than bilateral
Lacrimal gland enlarged and inflamed
Palpebral, orbital, or both lobes of the lacrimal gland may be involved
Chemosis of surrounding conjunctiva with an occasional follicular response
“S-shaped ptosis” due to relative involvement of upper temporal eyelid
Mucopurulent discharge may be present in bacterial etiologies
Tender palpable ipsilateral preauricular nodes more common with viral etiologies
Proptosis, downward displacement of the globe, or mild extraocular muscle (EOM) disruption in severe cases
Demographics
Acute dacryoadenitis is a rare disorder usually of infectious etiology. It is most common in children and young adults, but individuals of all ages can be affected. Route of infection can be blood borne, transconjunctival, transneuronal, or
through direct inoculation from trauma. Common causative agents are viruses including mumps, Epstein-Barr (mononucleosis), herpes simplex, herpes zoster, and rarely human immunodeficiency virus (HIV). Bacterial dacryoadenitis is less common and often accompanies traumatic inoculation. Bacterial etiologies include Staphylococcus sp., Streptococcus sp., Haemophilus influenzae, and Neisseria gonorrhoeae. Systemic inflammatory disorders such as sarcoidosis, Wegener’s granulomatosis, and Crohn’s disease usually manifest as chronic or bilateral dacryoadentis but must be ruled out. Rarely neoplastic etiologies including leukemia and lymphoma present as acute dacryoadenitis.
through direct inoculation from trauma. Common causative agents are viruses including mumps, Epstein-Barr (mononucleosis), herpes simplex, herpes zoster, and rarely human immunodeficiency virus (HIV). Bacterial dacryoadenitis is less common and often accompanies traumatic inoculation. Bacterial etiologies include Staphylococcus sp., Streptococcus sp., Haemophilus influenzae, and Neisseria gonorrhoeae. Systemic inflammatory disorders such as sarcoidosis, Wegener’s granulomatosis, and Crohn’s disease usually manifest as chronic or bilateral dacryoadentis but must be ruled out. Rarely neoplastic etiologies including leukemia and lymphoma present as acute dacryoadenitis.
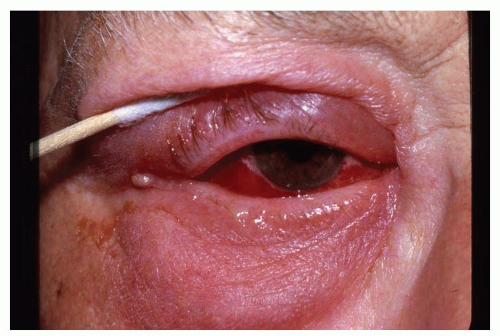 Figure 11-1. Dacryoadenitis. |
Significant History
Recent and rapid onset of symptoms
Occasional fever and leukocytosis
Laboratory Tests
Complete blood count (CBC) with differential: Leukemia, lymphoma
Culture any discharge on blood (most bacteria), chocolate (Haemophilus sp., Neisseria gonnorrhoeae), and thioglycollate agar (aerobic and anaerobic bacteria)
Computed tomography (CT), magnetic resonance imaging (MRI), or orbital ultrasound: Delineates extent of tissue involvement, especially indicated with proptosis, downward displacement of the globe, limited EOM motility, or decreased vision
Blood titers for appropriate suspected viral etiologies: Mumps, Epstein-Barr, HIV
Lacrimal gland biopsy: Atypical presentations or lack of appropriate treatment response
The Treatment
Broad-spectrum antibiotics should be initiated until cultures, titers, and laboratories can better direct therapy. Appropriate choices would include
Amoxicillin/clavulanate 500/125 mg twice daily
Cephalexin 250 to 500 mg four times daily
Penicillin/cephalosporin sensitive: Azithromycin: 500 mg daily for 3 days or 250 mg twice a day for 1 day, then once daily for 4 days
Severe presentations or pediatric cases: Referral for possible hospitalization with intravenous (IV) drug therapy
Viral Etiologies
Cool compresses
Topical lubricants
Appropriate analgesic as needed
Suspected herpetic: Acyclovir 400 mg five times a day (simplex) or 800 mg five times a day (zoster), Valacyclovir 1,000 mg three times a day, Famciclovir 500 mg three times a day
Chronic/Granulomatous Dacryoadenitis
Andrew Mick
ICD-9: 375.02
THE DISEASE
The Patient
Clinical Symptoms
Chronic or recurrent swelling and redness of the upper lid
Bilateral cases more common than with acute dacryoadenitis
Occasional pain and double vision
Clinical Signs
Localized mass in the lateral upper eyelid area
Lacrimal gland enlarged and inflamed
Proptosis, downward displacement of the globe, or EOM disruption in severe cases
Etiology
Chronic/granulomatous dacryoadenitits has a variety of etiologies: Inflammatory (sarcoidosis, Wegener’s granulomatosis, Crohn’s disease), infectious (tuberculosis, mumps, HIV, syphilis), and neoplastic (leukemia, lymphoma)
Significant History
Symptoms/signs of systemic infectious, inflammatory, or neoplastic disease
Laboratory Tests
Suspected leukemia/lymphoma: CBC with differential
Suspected sarcoidosis: Chest x-ray, serum angiotensin-converting enzyme (ACE)
Suspected Wegener’s granulomatosis: Sinus/chest x-ray, antineutrophil cytoplasmic antibody (ANCA) test, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)
Suspected Crohn’s disease: History of characteristic symptoms (weight loss, chronic diarrhea, abdominal pain), hematocrit/hemoglobin (gastrointestinal bleeding), ESR, x-ray with barium, abdominal CT
Suspected tuberculosis: Purified protein derivative with anergy panel
Suspected syphilis: Rapid plasma reagin or Venereal Disease Research Laboratory and fluorescent treponemal antibody absorption
Suspected HIV: Serology
CT, MRI, or orbital ultrasound: Delineates extent of tissue involvement, especiallyindicated with proptosis, downward displacement of the globe, limited EOM motility, or decreased vision.
Lacrimal gland biopsy
The Treatment
Treatment will depend on the underlying cause of the chronic dacryoadenitis and will involve referral to appropriate subspecialist for evaluation.
Dacryocystitis
Andrew Mick
ICD-9: 375.30
THE DISEASE
Pathophysiology
The disorder is characterized by acute or chronic infection or inflammation of the lacrimal sac. Complete or partial obstruction of the nasolacrimal duct is often the precipitating event prior to infection. Obstruction can result from developmental anomalies, nasal/sinus disease, trauma, neoplasm, dacryolith formation (lacrimal calculi), or systemic inflammatory disease.
Etiology
Acute (ICD-9: 375.32)
Lacrimal stenosis that results in secondary acute and severe infection
Commonly cultured bacteria are Gram positive (Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pneumoniae) and Gram negative (Pseudomonas aeruginosa, Escherichia coli)
Rarely anaerobicbacteria (Actinomyces israelii, Propionibacterium acnes)
Rarely fungi (Aspergillus sp., Candida sp.)
Chronic (ICD-9: 375.42)
Partial or complete blockage of the nasolacrimal system that results in secondary chronic infection
Commonly cultured pathogens include Gram-positive bacteria (Staphylococcus sp., Streptococcus sp.), coagulase-negative staphylococci, Gram-negative bacteria (P. aeruginosa, E. coli), and fungi (Aspergillus sp., Candida sp.)
The Patient
Clinical Symptoms
Acute
Pain, redness, and swelling around the lacrimal sac
Tearing and discharge
Occasional fever
Chronic
Tearing may be the only symptom in many cases
Occasional swelling around the lacrimal sac
Discomfort with local digital pressure
Clinical Signs
Acute
Edema and hyperemia around the lacrimal sac
Swelling concentrated under the medial canthal ligament
Mucopurulent discharge expressed from the puncta
Localized abscess with possible breakthrough to the skin surface (Fig. 11-2)
Occasional preauricular and submandibular swollen lymph nodes
Chronic
Epiphora
Local swelling around lacrimal sac
Mucopurulent material expressed from puncta with digital pressure
Demographics
Acute dacryocystitis occurs in all age groups with highest incidence in middle-aged adults. Women are afflicted more commonly than men and whites more commonly than other races. Chronic dacryocystitis can occur in infancy with congenital nasolacrimal obstruction. More commonly, it presents in elderly patients often due to involutional stenosis or scarring of the nasolacrimal drainage system.
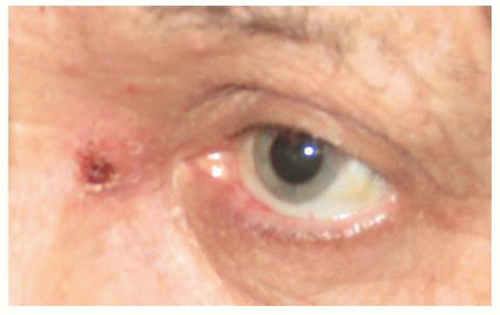 Figure 11-2. Dacryocystitis. |
Significant History
Tearing
Discharge
Chronic conjunctivitis
Chronic sinusitis or current upper respiratory tract infection
Laboratory Tests
Culture-expressed discharge on blood (all bacteria), chocolate (children: Haemophilus sp.), thioglycollate (aerobic and anaerobic), Sabouraud’s (fungal) agar
CT scan of orbit and sinuses to rule out widespread pathology or neoplasm: When no immediate improvement occurs with appropriate therapy
The Treatment
Broad-spectrum antibiotics that have coverage for the common bacterial causative agents should be initiated until cultures can better direct therapy. Appropriate choices would include
Amoxicillin/clavulanate 500/125 mg twice a day
Cephalexin 250 to 500 mg four times a day
If penicillin/cephalosporin sensitive: Azithromycin 500 mg daily for 3 days or 250 mg twice a day for 1 day, then once daily for 4 days
Severe presentations or pediatric cases: Referral for possible hospitalization with IV drug therapy
Warm compresses
Analgesic therapy is important because there is often significant pain. Appropriate therapy includes:
Mild pain: Acetaminophen 500 mg every 4 to 6 hours, Ibuprofen 400 to 600 mg every 4 to 6 hours, Naproxen 250 to 500 mg two times a day
Moderate pain: Acetaminophen with codeine (30 mg codeine) every 4 to 6 hours
Severe pain: Acetaminophen (500 mg) with hydrocodone (5 mg) every 4 to 6 hours, Ibuprofen (200 mg) with hydrocodone (7.5 mg) every 4 to 6 hours, Acetaminophen (325 mg) with oxycodone (10 mg) every 4 to 6 hours
Consider incision for nonresolving dacryocystitis with abscess
Consider external or endonasal endoscopic dacryocystorhinostomy (DCR) for nonresolving dacryocystitis
Febrile or pediatric cases with systemic disease should be referred for possible hospitalization with IV drug therapy
Canaliculitis
Andrew Mick
ICD-9: 375.31—ACUTE CANALICULITIS, LACRIMAL
ICD-9: 375.41—CHRONIC CANALICULITIS
THE DISEASE
Pathophysiology
The disorder is characterized by infection or inflammation of the canaliculi.
Etiology
Infectious agents include bacteria (A. israelii, Propionibacterium propionicum), fungi (Candida sp., Aspergillus sp.), and viruses (Herpes simplex). Canaliculitis is rarely associated with intracanalicular punctal plug occlusion.
The Patient
Clinical Symptoms
Irritation, redness, and swelling over medial portion of eyelids
Tearing and discharge
Clinical Signs
Mucopurulent discharge or concretions expressed from punctum
Concretions felt while probing canaliculus
Conjunctivitis more severe nasally
Erythematous area around punctal openings
Periocular skin vesicles (herpes simplex)
Demographics
Canaliculitis can affect people of all ages but is more common in elderly populations.
Significant History
Chronic/recurrent conjunctivitis
Epiphora
History of herpetic eye disease
Laboratory Tests
Culture any discharge from punctum on blood (all bacteria), chocolate (children: Haemophilus sp.), thioglycollate (aerobic and anaerobic bacteria), and Sabouraud’s (fungi) agar
The Treatment
Cultures positive for bacteria: Polymyxin B/trimethoprim solution four times a day or as directed by cultures
Cultures positive for fungus: Natamycin 5% suspension four times a day
Suspected herpetic infection: Trifluridine 1% solution four times a day
Removal of debris in canaliculus with irrigation
Canaliculotomy or snip punctoplasty may be indicated in nonresponsive canaliculitis
Epiphora
Andrew Mick
ICD-9: 375.20
THE DISEASE
Pathophysiology
The presentation of excessive tearing can be because of lacrimal hypersecretion or failure of the lacrimal system
to adequately drain the tears. The four primary mechanisms are as follows:
to adequately drain the tears. The four primary mechanisms are as follows:
Dry eye or other secondary causes of reflex hypersecretion of tears
Blockage within the lacrimal drainage apparatus or punctal malposition
Secondary hypersecretion of the lacrimal gland due to mechanical effects
Primary hypersecretion of the lacrimal gland
Etiology
Dry eye: Dryness produces ocular irritation that results in subsequent hypersecretion of tears
Secondary hypersecretion: Environmental irritants (smog, dust, or pollen) and mechanical irritants (trichiasis, entropion, or ectropion) can also produce irritation and induce hypersecretion
Primary hypersecretion: Many etiologies can produce direct stimulation of the lacrimal gland by infection/inflammation (see “Dacryoadenitis”): Viral infections (mumps, Epstein-Barr, herpes zoster), bacterial infections (Straphylococcus sp., Streptococcus sp., N. gonorrhoeae) inflammatory conditions (sarcoidosis, thyroid ophthalmopathy, Wegener’s granulomatosis, Sjögren’s syndrome)
Use of topical or systemic parasympathomimetic agents
Tumors of the lacrimal gland
Blockage of the Lacrimal Drainage System
Blockage of lacrimal drainage can be congenital or acquired and occur proximally or distally within the system.
Congenital Structural Blockage
ICD-9: 375.55 OR 743.65
The most common congenital causes of nasolacrimal obstruction include the following:
Failure of the distal end of the duct to completely canalize during development
Lack/malformation/membranes of one or more puncta
Lack/malformation/membranes of the canaliculi
Congenital tumors of the lacrimal sac:
Mucocele
Hemangioma
Dermoid
Membrane/cyst in the nasolacrimal duct
Acquired Structural Blockage
ICD-9: 375.56
Acquired nasolacrimal duct obstruction in adults is most often caused by age-related anatomical changes or low-grade infection or inflammation of the lacrimal drainage system. Proximal end blockage:
Lid ectropion resulting in eversion of the punctum away from the tear lake: Ectropion can be caused by any chronic inflammation/infection (blepharitis, allergic conjunctivitis), scarring (chemical burns, skin disease), facial nerve palsy, age-related changes to the lid anatomy, or history of blepharoplasty
Megalocaruncles: Enlarged caruncle that extends to the level of the lower punctum with excess tissue that pushes punctum away from its appositional location with the tear lake
Punctal stenosis: Scarring/narrowing/occlusion
Canalicular stenosis: Scarring/narrowing/occlusion, topical and systemic medications can cause scarring (topical timolol, systemic docetaxel, systemic 5-fluorouracil)
Distal end blockage:
Lacrimal sac and nasolacrimal duct obstructions: Dacryocystitis, dacryolith formation, cysts, mucocele, neoplasms
The Patient
Clinical Symptoms
Clinical Signs
Negative Jones I or II tests
Asymmetric dye disappearance test
Increased lacrimal tear lake
Lid, punctum, caruncle abnormalities
Tender swollen lacrimal gland or sac area
Expression of purulent material from the punctum
Demographics
Epiphora can present in all age groups.
Significant History
Persistent tearing
Recurrent sinusitis or dacryocystitis
Swelling or pain over lacrimal sac
History of facial trauma or lid surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


