Purpose
To study the effects of laser-assisted subepithelial keratectomy (LASEK) with mitomycin C (MMC) on the keratocyte population.
Design
Prospective, nonrandomized, interventional, comparative case series.
Methods
Fifty-six eyes treated at Vissum Santa Hortensia, Madrid, Spain, were included in the study. We compared 28 eyes treated with LASEK with intraoperative 0.02% MMC versus 28 non-treated eyes. Keratocyte density was measured 3 months after the surgery in the anterior, mid, and posterior stroma and was compared with the corresponding layers in the control eyes. The anterior layer in the LASEK group was compared with 2 layers in the control group: the most anterior stromal layer and the 80 μm-deep layer, because that was the mean ablation depth performed in eyes that underwent LASEK.
Results
We found a statistically significantly lower keratocyte population in the most anterior stromal layer after LASEK with MMC compared with both the most anterior stromal layer and the 80 μm-deep layer in controls. On the contrary, the treated group showed a significantly higher keratocyte density in both the mid stroma and the deep stroma. The comparison between the average densities through the entire cornea showed a significantly higher keratocyte population in the LASEK with MMC group.
Conclusions
LASEK with MMC seems to cause a decrease in the anterior stromal cells 3 months after the surgery compared with nonoperated corneas. There seems to be a compensating proliferation of keratocytes in the deeper corneal layers, suggesting that the ability of keratocytes to repopulate the cornea is maintained after the surgical procedure.
Mitomycin C (MMC) has played a deciding role in the current revival of excimer laser surface ablation techniques. MMC is an alkylating agent with cytotoxic and antiproliferative effects that reduces the myofibroblast repopulation after laser surface ablation, and therefore reduces the risk of postoperative corneal haze. It is used prophylactically to avoid haze after primary surface ablation and therapeutically to treat pre-existing haze.
The keratocytes are the target of the MMC antihaze action. It is the cytotoxic and antiproliferative effects of the MMC on the corneal stromal keratocytes that causes its capacity to reduce haze, because it inhibits its activation, proliferation, and differentiation into myofibroblasts. However, this antimitotic effect has led to fear the consequences of a possible long-term depletion of the keratocyte population. The few studies analyzing the postoperative keratocyte population after intraoperative MMC show contradictory results ( Table 1 ). Therefore, we decided to study keratocyte density after laser-assisted subepithelial keratectomy (LASEK) with intraoperative MMC and to compare it with that of nonoperated healthy control eyes.
| Authors | No. of Eyes Receiving MMC | Subject of Study | Type of Study | MMC Dose (%) | MMC Application Time | Last Follow-up | Keratocyte Density at Last Follow-up |
|---|---|---|---|---|---|---|---|
| Kim et al. | 18 | Animal study (rabbits) | Prospective, randomized, comparative study | 0.02 | 2 min | 3 mos | Decreased |
| Netto et al. | 182 | Animal study (rabbits) | Prospective, randomized, comparative study | 0.0020.02 | 12 s to 2 min | 1 mo | Time and dose-dependent decrease |
| Rajan et al. | 16 | Laboratory study (human corneas in vitro) | Prospective, randomized, comparative study | 0.02 | 1 min, 2 min | 1 mo | Time-dependent decrease |
| Xu et al. | 20 | Animal study (rabbits) | Prospective, randomized, comparative study | 0.02 | 5 min | 6 mos | Nondecreased |
| Gambato et al. | 36 | Human study | Prospective, randomized, comparative study | 0.02 | 2 min | 3 yrs | Reported as nondecreased (but no data available) |
| Midena et al. | 56 | Human study | Prospective, randomized, comparative study | 0.02 | 2 min | 5 yrs | Nondecreased compared with eyes without MMC |
Methods
We performed a prospective study of consecutive eyes that underwent LASEK to correct a myopic error (with or without astigmatism) and that received intraoperative MMC prophylactically because of an ablation depth of more than 50 μm.
When evaluating for surgery, we excluded patients with unstable refraction and keratoconus suspects. We excluded from analysis those cases with previous ocular surgery (either refractive or other type) and those with a systemic disease that could alter the wound-healing process, such as diabetes or connective tissue disorders. A group of normal subjects with nonoperated healthy corneas also were analyzed and served as controls.
All study patients underwent a full ophthalmologic examination before surgery that included the measurement of uncorrected visual acuity, the best spectacle-corrected visual acuity (using a Snellen chart [Nidek auto chart projector CP 670; Nidek Co, Ltd, Gamagori, Japan] and including manifest and cycloplegic refractions), slit-lamp biomicroscopy, tonometry (CT-80; Topcon, Tokyo, Japan), corneal pachymetry (DGH 5100 contact pachymeter; DGH Technology, Inc, Exton, Pennsylvania, USA), keratometry and corneal topography (CSO; Compagnia Strumenti Oftalmici, Firenze, Italy), mesopic pupil measurement (Colvard pupillometer; Oasis, Glendora, California, USA), and funduscopy.
Surgical Technique
All procedures were performed by 2 surgeons (M.A.T.; L.d.B.-L.), using the same Esiris Schwind Excimer Laser (Schwind Eye Tech Solutions, Kleinostheim, Germany) using a PRK nomogram and conventional treatment.
All surgeries were performed using topical anesthesia (lidocaine 2%). De-epithelialization was performed using 20% alcohol solution (diluted in balanced salt solution) instilled inside an 8-mm corneal marker centered on the pupil and left for 40 seconds. A cellulose sponge was used to remove the alcohol and balanced salt solution was instilled copiously to rinse the ocular surface. The edges of the flap were dried with a sponge and the epithelial flap was peeled back with a crescent blade (Alcon Surgical, Orlando, Florida, USA), leaving a hinge at the 12-o’clock position. The stromal bed was dried with a sponge, the eye tracker was set in the center of the pupil, and the ablation was performed. After laser ablation, a 7-mm round cellulose sponge soaked in MMC 0.02% was applied for 30 seconds over the ablated stroma. The programmed ablation was 10% less that the intended correction to avoid overcorrection. The stroma then was rinsed copiously with balanced salt solution, and the epithelial flap was repositioned using the same cannula. A therapeutic soft contact lens (Acuvue Oasys; Johnson & Johnson Vision Care, Inc, Jacksonville, Florida, USA) was placed carefully on the eye and antibiotic drops (ciprofloxacin 3 mg/mL) and nonsteroidal anti-inflammatory drops (ketorolac trometamol 5 mg/mL) were applied.
Postoperative Follow-up
The medications consisted of topical antibiotic (ciprofloxacin 3 mg/mL) and steroid (fluorometholone alcohol 2.5 mg/mL) drops 4 times daily during the first week after surgery. The steroid drops then were tapered and stopped 1 month after surgery. The therapeutic contact lens was removed after re-epithelialization was complete, 5 to 7 days after surgery. Examinations were scheduled at 1 day, 1 week, and 1 and 3 months after surgery. Confocal microscopy was performed at the 3-month postoperative visit.
In Vivo Confocal Microscopy
Laser scanning in vivo confocal microscopy was performed using the Heidelberg Retina Tomograph II with the Rostock Cornea Module (HRTII/RCM; Heidelberg Engineering, Heidelberg, Germany). This microscope uses a 670-nm red wavelength diode laser source. A ×60 objective water immersion lens with a numerical aperture of 0.9 (Olympus, Tokyo, Japan) was used. The dimensions of the images obtained using this lens are 400 × 400 μm, and the manufacturer quotes the transverse resolution and optical section thickness of 1 and 4 μm, respectively. The RCM uses an entirely digital capture system. The device can scan automatically through 80 μm of the cornea, at any depth, capturing 30 frames/s, but to obtain a scan of the entire cornea, the microscope needs to be advanced manually through the full thickness of the cornea.
The method of examination was as follows: each eye was anesthetized with 1 drop of 1% tetracaine chlorohydrate (Alcon Cusí Laboratories, Barcelona, Spain). Viscotears (Carbomer 980, 0.2%; Novartis, North Ryde, Australia) was used as a coupling agent between the applanating lens cap and the cornea. During the examination, all subjects were asked to fixate on a distance target aligned to enable examination of the central cornea. The lens then was advanced manually until it contacted the cornea. The full thickness of the central cornea was scanned. The total duration of in vivo confocal examination was approximately 2 minutes per eye, and none of the subjects experienced any visual symptoms or complications as a result of the examination.
Three scans through the entire cornea were recorded from each eye, and the one with fewer motion artefacts then was selected for analysis. All scans were performed by the same trained examiner (J.L.H-V.).
Keratocyte Density Measurement
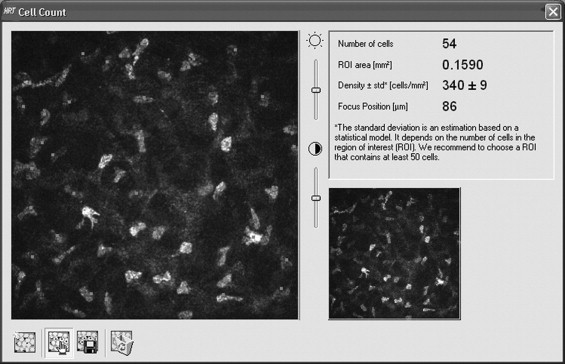
The digital images were loaded into an interactive computer program. One observer (P.C.) manually selected the bright objects (keratocyte nuclei) in each image. The same area (400 × 400 μm of cornea) was used for all images. The same examiner did the counting in all the scans. Objects that touched the bottom and left boundaries of this area were counted, whereas objects that crossed the top or right edges were not counted. The computer then provides the value of the keratocyte density expressed as cells per square millimeter ( Figure 1 ).
Volumetric density was estimated using the method published by McLaren and associates, in which the cell density was determined by the formula:
where N is the number of cells identified in the rectangular area A , and ϕ is the optical section thickness. This optical section thickness ϕ, or depth of field, was estimated, as McLaren and associates proposed, by the distance that the scanner moved from the gradual appearance of a cell to the gradual disappearance of that cell. The number of frames in which a cell would have been counted was multiplied by the average distance between frames. For this purpose, we used the automatic scan mode of the HRTII/RCM to obtain 3 scans with a mean thickness of 77 μm, a mean frame capture of 39 frames per scan, and an average distance between frames of 1.93 μm. In each of those 3 automatic scans, we checked 15 keratocytes (45 keratocytes in total). This method yielded a depth of field of 15.63 ± 1.82 μm.
At each determined depth of study, 3 images were analyzed: the one that most exactly corresponded to the determined depth and the images just anterior and posterior, with a difference between them of less than 20 μm. Cells were counted in the 3 images and the mean was obtained.
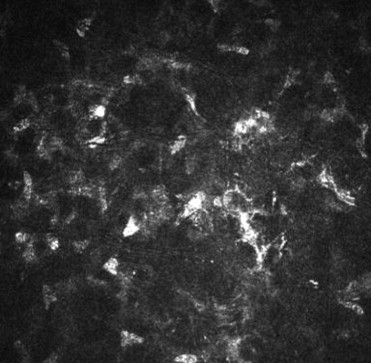
In the LASEK group, images were analyzed at the following depths: (1) anterior stroma (stromal bed; first good-quality image of the keratocytes under the epithelium; Figure 2 ), (2) mid stroma (200 μm above the endothelium), and (3) deep stroma (50 μm above the endothelium; Figure 3 ).