Purpose
To determine whether diabetes mellitus is protective for nuclear sclerotic cataract at baseline and 6 and 12 months after vitrectomy surgery.
Design
Prospective, interventional cohort study.
Methods
Phakic diabetic and nondiabetic patients undergoing vitrectomy surgery for a variety of retinal conditions underwent Scheimpflug lens photography in the operated and fellow eye at baseline and at 6 and 12 months after vitrectomy surgery.
Results
Of 52 eyes included in the analysis, 23 eyes were from diabetic patients, 14 of which had surgery for ischemic retinopathy. At baseline, eyes with ischemic diabetic retinopathy had less nuclear sclerotic cataract than nonischemic diabetic and nondiabetic eyes. This was true for eyes undergoing vitrectomy surgery ( P = .0001) and for fellow eyes ( P = .003). Nuclear sclerotic cataract developed after vitrectomy surgery in nonischemic diabetic eyes and nondiabetic eyes at the same rate. Diabetic eyes with ischemic retinopathy showed no significant progression of nuclear opacification, and therefore had significantly less postvitrectomy nuclear cataract at 6 months ( P < 1 × 10 −6 ) and at 12 months ( P < .001) than nondiabetic or nonischemic diabetic eyes. Normalizing to baseline opacity and adjusting for age and other comorbidities did not alter this result.
Conclusions
Ischemic diabetic retinopathy, not just systemic diabetes mellitus, protected against nuclear sclerotic cataract at baseline and after vitrectomy surgery. These findings are consistent with the hypothesis that increased exposure to oxygen is responsible for nuclear cataract formation.
With increasing age, the nucleus of the crystalline lens gradually increases in opacity and hardness in all individuals. When nuclear opacities become visually significant, they are called nuclear sclerotic cataracts . In most Western populations, nuclear sclerotic cataracts are the most common reason for cataract surgery. In the United States, cataract surgery is the most often performed surgery, at a total direct cost of more than $3 billion per year.
Epidemiologic studies in populations around the world have identified recurring risk factors for nuclear cataracts including age, smoking, poorer nutrition, and living in a warmer climate. Studies that measured the incidence of specific types of cataract between monozygotic and dizygotic twins showed that approximately one third of the risk of nuclear cataracts can be attributed to heredity. Surprisingly, the biochemical links that connect environmental and hereditary risk factors to nuclear cataracts are not well understood.
Although much effort has been applied toward identifying risk factors for nuclear cataract, new information is emerging about possible protective factors. The most provocative of these is the presence of systemic diabetes mellitus. Two large epidemiologic studies revealed that diabetic patients may have a lower risk of nuclear cataract. The Age- Related Eye Disease Study, which examined 4477 individuals 60 to 80 years of age, found that moderate nuclear opacities were less common in persons with diabetes mellitus (odds ratio, 0.68; 95% confidence interval, 0.47 to 0.98). The 5-year follow-up results from the Reykjavik Eye Study confirmed that the incidence of nuclear sclerotic cataract was significantly lower in diabetic than in nondiabetic individuals (relative risk, 0.32; 95% confidence interval, 0.12 to 0.75; P < .01: Sasaki K, et al. IOVS 2006;47:ARVO E-Abstract 4135). A recent study suggested that systemic diabetes mellitus may protect against postvitrectomy nuclear sclerotic cataract. Smiddy and Feuer found that incident cataract surgery for postvitrectomy nuclear cataract was lower in diabetic than in nondiabetic individuals. The case-control study used cataract extraction as a primary end point in patients who had undergone vitrectomy for diabetic retinopathy, epiretinal membrane, or macular hole. The cumulative cataract extraction rates for the 3 groups 2 years after vitrectomy were 15%, 66%, and 53%, respectively. After adjusting for age, the difference between diabetic patients and the other 2 groups combined was highly significant ( P < .006). A significant weakness of this small, retrospective study was the use of cataract surgery as a surrogate for visually significant cataract, because diabetic patients may have reason to delay or avoid additional surgical procedures.
Nuclear sclerotic cataract is caused by oxidation of the proteins in the lens nucleus. In a study of donor eyes, degeneration of the vitreous body also was associated with nuclear cataract, independent of age. Vitrectomy surgery leads to nuclear cataract within 2 years in most patients older than 50 years. Because vitrectomy and vitreous degeneration increase fluid circulation in the eye, it was suggested that oxidative damage in nuclear cataract is caused by molecular oxygen from the retinal vasculature reaching the lens as a result of fluid circulation within the vitreous cavity. In 2006, we reported that vitreous oxygen tension was significantly lower in diabetic than in nondiabetic patients. We postulated that lower oxygen in the vitreous may be responsible for the lower prevalence and incidence of nuclear sclerotic cataract and a decreased incidence of surgery for postvitrectomy nuclear sclerotic cataract in diabetic patients. The lower oxygen tension found in the vitreous of diabetic patients may be a result of ischemic retinopathy and associated small vessel disease within the vascularized tissues of the eye. Quantification of the rate of cataract progression after vitrectomy in diabetic and nondiabetic patients may help to test this possibility. Herein we used quantitative Scheimpflug photography to document prospectively the progression of nuclear sclerotic cataract from baseline to 6 and 12 months after vitrectomy surgery in patients with ischemic diabetic retinopathy, diabetes with no retinopathy, and in nondiabetic patients.
Methods
In a single academic-based retina practice, patients who were undergoing vitreous surgery for a variety of retinal conditions were asked to participate in the research study. Inclusion criteria were age 51 to 80 years, ability to provide informed consent, better than hand movement vision in the fellow eye, and willingness to be followed up for 1 year. Exclusion criteria were prior cataract surgery, history of traumatic cataract, and prior vitrectomy surgery. Informed consent was obtained by the surgeon (N.M.H.).
The following information was recorded for all patients: age; medical history; presence of diabetes mellitus; surgical eye; diagnosis; presence or absence of ischemic diabetic retinopathy; procedure performed; presence of panretinal photocoagulation before vitrectomy; use of intraocular gas tamponade; any intraoperative adverse events, such as lens damage; and any deviations from the study protocol. A 5% dextrose solution was added to the vitrectomy infusion fluid for all diabetic eyes. Otherwise, there were no differences in surgical technique for diabetic or nondiabetic patients. For purposes of this study, ischemic diabetic retinopathy was defined as eyes with proliferative diabetic retinopathy, diabetic vitreous hemorrhage, or diabetic traction retinal detachment requiring vitrectomy surgery.
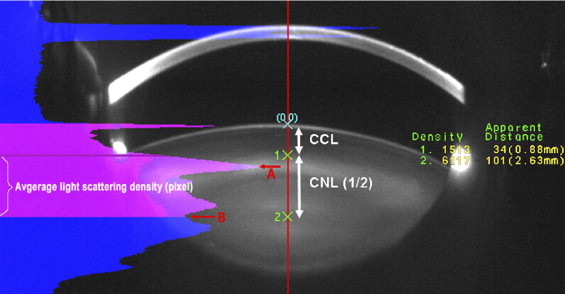
Before vitrectomy surgery, each patient underwent digital Scheimpflug lens photography. Although Scheimpflug technology has the ability to image cortical cataract, posterior subcapsular cataract, and nuclear cataract, no patients in this study had significant cortical or posterior subcapsular cataract at baseline or during follow-up. Only nuclear opacities progress after vitrectomy surgery. Therefore, the primary end point of the study was nuclear sclerotic cataract progression as measured by Scheimpflug photography at 6 and 12 months after vitrectomy surgery. Scheimpflug photographs quantify the density of nuclear light scattering in pixel intensity units. Lens images for both eyes were taken by the EAS-1000 anterior eye segment analysis system (NIDEK EAS-1000, Gamagori, Japan). Lens images were obtained at the same settings: slit length, 10 mm; flash power, 150 watt seconds; and at 0 and 180 degrees. Images were acquired and analyzed with the EAS-1000 analysis software (EAS_Win_Ver 123J). Nuclear opacity was quantified using average light scattering per pixel on the central line between the anterior surface of adult nucleus and central clear zone (a comparatively clear area at the center of the lens; Figure 1 ).
Statistical analysis was performed using the Student t test adjusted for multiple comparisons (Bonferroni; GraphPad Software Inc, LaJolla, California, USA). Multiple regression analysis was performed using Rweb1.03 on the server at bayes.math.montana.edu and SPSS software version 14.0 (SigmaPlot; SPSS, Inc, Chicago, Illinois, USA). P values less than .05 were considered significant.
Results
Fifty-two patients were enrolled. Three patients were excluded from the analysis because of lens trauma during surgery, poor cooperation with lens photography, or vasculopathy not related to diabetes. For 46 patients, 1 eye was included in the study. For 3 patients, both eyes were included in the study. Therefore, 52 eyes were included in the final analysis. Table 1 shows the retinal diagnoses for the eyes that were included in the study. There were 23 eyes from diabetic patients. Among them, 14 eyes had surgery for proliferative diabetic retinopathy. Nine eyes from diabetic patients had surgery for retinal diseases not related to ischemic diabetic retinopathy. Table 2 shows the number and age distribution of the patients in the study. Patients undergoing vitrectomy surgery for complications of ischemic diabetic retinopathy were significantly younger than the nonischemic patients (nondiabetic patients and nonischemic diabetic patients) requiring vitrectomy ( P = .005).
| Reason for Surgery | No. of Patients | No. of Surgical Eyes | DM | Ischemia |
|---|---|---|---|---|
| Proliferative diabetic retinopathy | 14 | 14 | 14 | Yes |
| Macular hole | 17 | 20 | 5 | No |
| Retinal detachment | 3 | 3 | 0 | No |
| Premacular fibrosis | 12 | 12 | 3 | No |
| Vitreous opacity | 3 | 3 | 1 | No |
| Total | 49 | 52 | 23 |
| Age (yrs) | No. of Cases | |||
|---|---|---|---|---|
| Baseline | 6 Months (IOL) | 12 Months (IOL) | ||
| Ischemic | 59 ± 6 a | 14 | 13 (0) | 8 (2) |
| Nonischemic | 65 ± 7 a | 38 | 28 (2) | 26 (14) |
| Total patients | 52 | 41 | 34 | |
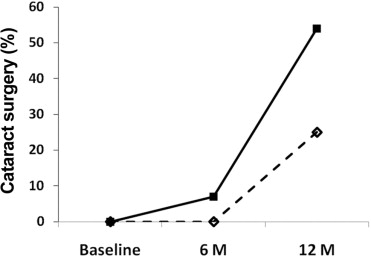
Of 14 eyes with ischemic retinopathy, Scheimpflug photographs were obtained from 13 patients at 6 months. One patient was lost to follow-up, and no eyes had cataract surgery. For this group of eyes, 8 patients returned for follow-up at 12 months. Two underwent cataract surgery and 6 underwent Scheimpflug photography. Four patients in the ischemic group were lost to follow-up and 2 were awaiting the 12-month time point. Therefore, of the 8 eyes for which follow-up was available at 12 months, 2 (25%) of 8 underwent cataract surgery ( Figure 2 ). Of the 38 eyes with nonischemic retinopathy, Scheimpflug photographs were obtained from 26 eyes at 6 months, 2 underwent cataract surgery, and 10 were lost to follow-up. For the nonischemic eyes at 12 months, 12 patients underwent Scheimpflug photography, 12 were lost to follow-up and 14 underwent cataract surgery ( Figure 2 ). Therefore, of the 26 eyes for which follow-up was available at 12 months, 14 (54%) of 26 had cataract surgery ( Figure 2 ). Therefore, a smaller percentage of ischemic eyes had cataract surgery at 6 and 12 months than nonischemic eyes ( Figure 2 ). Because the small sample size, this difference was not statistically significant.
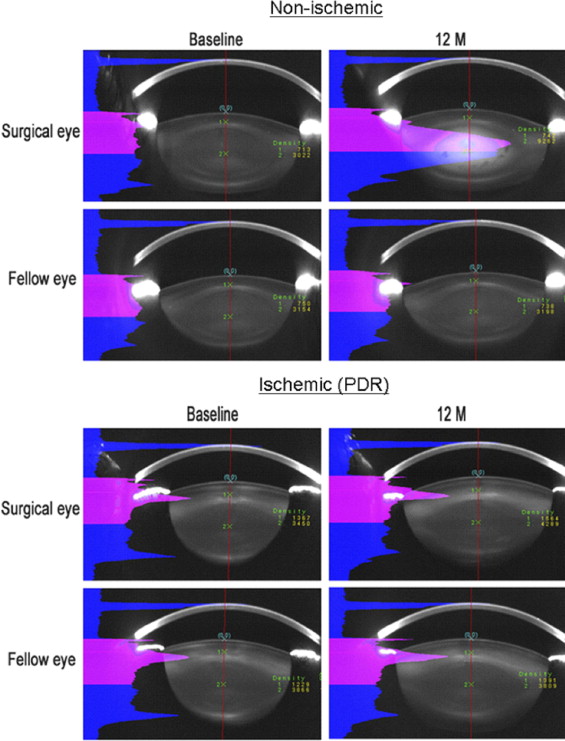
Scheimpflug photography was used to quantify nuclear opacity before and at 6 and 12 months after vitrectomy. Figure 3 shows Scheimpflug images from the operated and unoperated eyes of a nondiabetic patient 51 years of age and from a diabetic patient with ischemic retinopathy 56 years of age. In the nondiabetic patient, significantly more nuclear light scatter developed in the eye undergoing vitrectomy surgery than in the lens of the unoperated fellow eye. By contrast, in the patient with ischemic diabetic retinopathy, the eye undergoing vitrectomy surgery showed very little nuclear cataract progression compared with the lens in the fellow eye.
Nonischemic eyes had similar progression of nuclear cataract after vitrectomy. Table 3 shows the average nuclear light scattering units as measured by Scheimpflug photography before and after vitrectomy in the nondiabetic eyes and the nonischemic diabetic eyes undergoing surgery for non–diabetes-related conditions such as macular hole and macular pucker. There was no statistically significant difference between these 2 groups. Therefore, for the purpose of the analysis, nondiabetic and nonischemic diabetic eyes collectively were grouped as nonischemic eyes for comparison with eyes with ischemic diabetic retinopathy.
| Age (years) | Surgical Eyes | Fellow Eyes | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | 12 Months | Baseline | 6 Months | 12 Months | ||
| Nondiabetic | 63.9 ± 6.8 | 72.6 | 102.1 | 107.1 | 68.1 | 67.7 | 70.0 |
| Nonischemic diabetic | 68.9 ± 7.2 | 69.4 | 102.6 | 107.4 | 68.8 | 70.7 | 79.1 |
| P value | .09 | .50 | .96 | .98 | .90 | .70 | .65 |
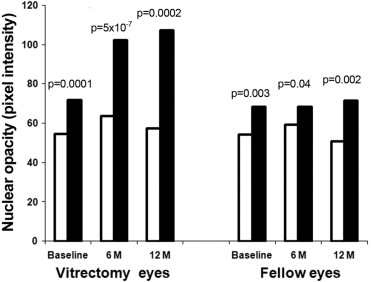
Ischemic and nonischemic eyes had different rates of cataract progression after vitrectomy. Figure 4 shows the average nuclear light scattering before and after vitrectomy in the ischemic eyes with diabetic retinopathy compared with the nonischemic eyes. The fellow eyes also are represented. At baseline (before vitrectomy), eyes with ischemic diabetic retinopathy had less nuclear light scattering than nonischemic eyes. This was true for eyes scheduled for vitrectomy surgery ( P = .0001) as well as fellow eyes ( P = .003). At 6 and at 12 months after vitrectomy surgery, eyes with ischemic retinopathy continued to have significantly lower nuclear opacity than nonischemic eyes ( P < .001 for both). In the fellow unoperated eye, the significant difference in nuclear opacity remained at 6 and 12 months.