This content is designed to acquaint the clinician with some of the more common ultrasonographic manifestations of clinical conditions that the otolaryngologist is likely to encounter in a general practice. The clinician requires a thorough knowledge of head and neck anatomy to best interpret the variations from normal structures demonstrated on ultrasound. A knowledge of sonographic artifacts may assist the examiner in properly identifying the process under review. Ultrasonography may be the best imaging study for certain organs. In many instances it is the first clinical study that directs further imaging. By providing the clinician with clues as to the underlying pathology, it allows a more efficient direction in determining which aspiration techniques to use.
A thorough knowledge of head and neck anatomy is critical to defining what are normal and abnormal findings on high-resolution ultrasound. At first, the transverse and sagittal orientations of the transducer can be confusing to the operator. The best way to overcome this problem is to select concentrated areas of the neck and identify as many normal structures as possible within that area. Instead of using a Doppler whenever a suspect blood vessel is identified, the operator will better understand relationships by tracing as much as possible the course of the vessel in gray scale both in transverse and sagittal planes. The transition from normal anatomy and a sound knowledge of scanning artifacts will serve as the best foundation for properly interpreting pathologic conditions.
Ultrasound interpretation in head and neck pathology
The beauty of ultrasound is that the examination process occurs in real time with the examiner learning how to merge the various planes of view into a dynamic 3-dimensional image. There is no substitute for the circumstance where the operator/managing clinician is performing this dynamic examination while constructing a concurrent differential diagnosis. A technician who does not possess the knowledge base of head and neck pathology is quite limited in this aspect of ultrasonography. However, radiologic technicians and radiologists are well educated about standardizing the examination process. This redundancy from one examination to the next is valuable in comparison of normal with abnormal structure, and it lessens the likelihood of omissions.
The otolaryngologist who performs office-based ultrasound must avoid cutting corners in defense of time to maintain a proper standard and to avoid overlooking a key portion of the examination. As an example, it is easy to omit a proper survey of lymph node basins when concentrating on a thyroid nodule and, of course, both elements may be linked and are important to examine in the same ultrasound procedure. Conversely, a thyroid examination should be part of every head and neck ultrasound procedure. Thyroid pathology is common and malignancies can be occult and asymptomatic. In a similar manner, lymphadenopathy alone may not be as meaningful as lymphadenopathy in conjunction with an irregular thyroid nodule containing microcalcifications.
This article is constructed to present some of the pathologic conditions that affect the salivary glands, soft tissues, lymph nodes, thyroid and parathyroid glands, esophagus, vascular structures, congenital cysts, and even mandibular relationships. The content provides the physician with information and representative images of the more common conditions involving the head and neck. Some of this information may also be covered elsewhere in this publication, but it is presented here as a systems overview and stepping point for further in-depth study. High-resolution ultrasound is the best modality for detailing pathology of the thyroid gland before fine-needle aspiration cytology. An enlarged parotid gland is often mystifying at initial history and physical examination, but the added advantage of concurrent ultrasound usually allows the clinician to understand the problem and direct earlier proper management.
Skin and Subcutaneous Tissues
High-resolution transducers in the range of 10 to 12 MHz provide good detail of the skin and subcutaneous tissues. If one has access to even higher frequency probes, ie, 17 MHz, the image detail can be stunning. One very helpful use of the ultrasound examination of a skin-related process is to differentiate cellulitis from abscess, especially in children. A cellulitic process is diffuse and edema of the tissues can be identified on ultrasound. In contrast, an abscess is usually a discrete hypoechoic to anechoic area that may extend deep to the subcutaneous plane ( Fig. 1 ). A foreign body can usually be identified even if it is not ferromagnetic or may not demonstrate on conventional soft tissue radiograph. Fistulous tracts are hypoechoic channels that usually can be traced to the site of origin ( Fig. 2 ). If the fistula arises from the skin surface, the tract can be easily traced and the condition properly identified. A fistula arising from the aerodigestive tract that extends into the subcutaneous tissues or thyroid (fourth branchial pouch sinus) may be traceable on ultrasound ( Fig. 3 ).

Frequently, ultrasound is the initial study as part of a more comprehensive imaging profile. In many instances, it can suffice as the only requisite study. A sebaceous cyst is usually properly identified and characterized by physical examination alone, but it is instructive to demonstrate its sonographic characteristics ( Fig. 4 A, B). It is usually seen at the level of the dermis and can extend by pressure enlargement to involve the subcutaneous level. The mass is discrete and well-encapsulated and the contained sebum does not produce as homogeneous an image as a fluid-filled cyst. Posterior enhancement is present to some degree. Lipomas are common and usually arise from the subcutaneous adipose tissues ( Fig. 5 A). They have a soft, somewhat compressible physical characteristic, but occasionally differentiation from a lymph node can be difficult. Fine-needle aspiration without ultrasound guidance will be nondiagnostic and the lipocytes will be misinterpreted as contaminants during the penetration process. The ultrasonographic features of a lipoma are virtually diagnostic. The overall structure is ovoid and somewhat discrete from the surrounding subcutaneous tissues. Horizontal hyperechoic lines are its hallmark, probably representative of the connective tissue bands that compartmentalize the lipoma. Power Doppler confirms the avascular nature of the mass. Lipomas can be found wherever there is adipose tissue. An example of a parotid lipoma is demonstrated (see Fig. 5 B). The sonographic features are so typical that the diagnosis can be established on ultrasound study alone.
Salivary Glands
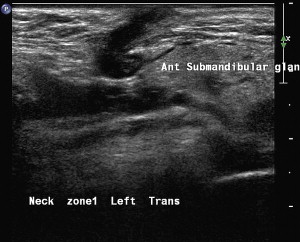
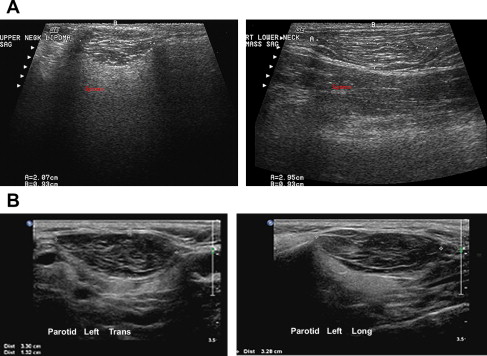
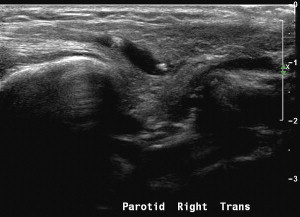
The normal parotid and submaxillary glands have the same ground-glass appearance on ultrasound. Whereas the submaxillary gland is relatively discrete and its dimensions easy to measure, the parotid gland is more difficult to define. Both glands contain large, intermediate, and small ducts and share an intimate relationship with surrounding lymph nodes. In fact, subcapsular lymphadenopathy is usually identified within the parenchyma of the parotid gland. Of all studies to investigate parotid pathology, ultrasound is an efficient and cost-effective modality with no radiation exposure. In addition to the initial study, it permits an easy method to efficiently track an inflammatory process over time.
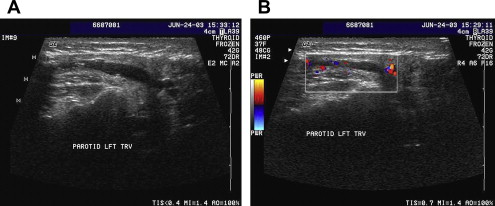
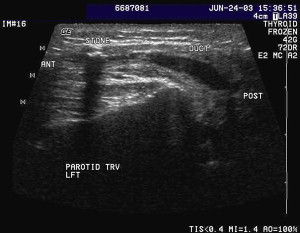
Obstructing Calculus
In this condition, the ductal system will be ecstatic ( Fig. 6 A). The examiner may not be certain whether these conduits are of ductal or vascular origin; the Doppler assessment clarifies the findings with certainty (see Fig. 6 B). A careful inspection of the ductal system distal to the gland hilum may reveal a discrete hyperechoic density that also demonstrates posterior shadowing artifact ( Fig. 7 ). Occasionally, multiple stones may be seen in the duct system, and if they are smaller than the walls of the obstructed duct, the ultrasound waves may cause them to move or vibrate. This can be seen on the real-time images and archived with cine loops ( Fig. 8 ).
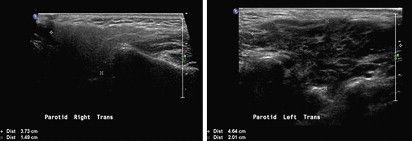
Diffuse Parotitis
The gland may be inflamed with evidence or obstruction to the main duct system. In this circumstance, there may be edema or areas of heterogeneity throughout the gland and the gland itself is enlarged ( Fig. 9 ). It is always a good idea in this circumstance to examine and measure the salivary glands in question bilaterally to compare the normal with abnormal architecture and dimensions.
Sjogren’s Syndrome
Lymphoepithelial lesions of the parotid glands have a very distinct image characteristic. The histopathology demonstrates discrete areas throughout the gland that resemble germinal centers in a lymph node ( Fig. 10 ). This same appearance can be identified on ultrasound with multiple discrete hypoechoic islands throughout the entire gland. This same echo-appearance is noted in Mikulicz disease and recurrent parotitis of childhood.

Parotid Cysts
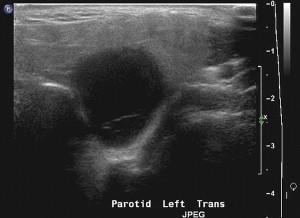
A single parotid cyst may represent a focal obstruction of a smaller proximal duct, or as a congenital anomaly (first branchial cleft cyst). These cysts are discrete, rounded, anechoic, thinly encapsulated, and demonstrate bright posterior enhancement ( Fig. 11 ). Parotid cysts, either single or multiple, may indicate HIV disease. Occasionally, the cyst will contain proteinaceous debris, which presents on ultrasound as discrete punctate areas throughout the cyst ( Fig. 12 ). In real time, this debris may demonstrate vibratory movement from the transmitted sound waves.

Tumor
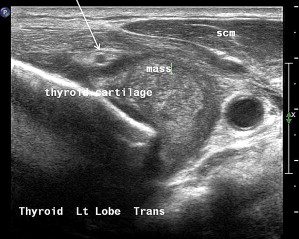
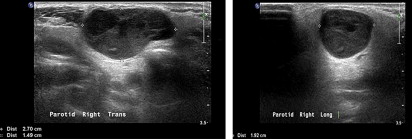
A mass within the parenchyma of either the submaxillary or parotid gland cannot be classified with certainty without cytologic confirmation; however, there are sonographic findings that may suggest the likelihood of malignancy. The most worrisome abnormalities are irregular ill-defined borders of the mass ( Fig. 13 ) with a surrounding normal gland, infiltration of the skin or adjacent muscles, and clear-cut malignant adenopathy of the upper neck in association with a parotid mass. Conversely, a very discrete mass with sharply marginated borders may demonstrate some irregularity in knoblike but confined projections. This type of mass may demonstrate a hypoechoic uniform echo architecture and posterior enhancement artifact, which usually is supportive of a cyst.

The one solid tumor that demonstrates posterior enhancement is a benign mixed tumor ( Fig. 14 ). A Warthin tumor may demonstrate characteristics of a cyst, but generally it is not as homogeneous as a mixed tumor and does not demonstrate discrete projections. Parotid malignancies such as adenoid cystic, mucoepidermoid, and acinic cell carcinomas often do not demonstrate specific sonographic features. Thus, fine-needle aspiration cytology is mandatory for any salivary gland mass.
Occasionally, the precise tissue type cannot be determined; the cytopathologist may be able to diagnose only malignancy, but not much more. Ultrasound-guided core biopsy (16- or 18-gauge) is an excellent adjunctive procedure in this circumstance to allow the pathologist to render a precise diagnosis before surgical intervention. Intraoperative frozen section may similarly plague the pathologist, especially if critical decisions regarding the facial nerve depend on accurate histopathology. A diffuse infiltrative process may be identified as parotid lymphoma, which can be partially characterized with fine-needle aspiration cytology and flow cytometry. Again, core biopsy under ultrasound guidance may be all that is required to precisely identify the lymphoma type and direct appropriate treatment.
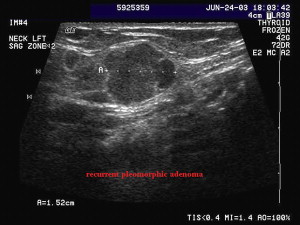
Patients with benign mixed tumors who have either tumor spill at surgery or improper management with incisional biopsy are at risk for multiple nodular recurrence. Ultrasound is an excellent modality to carefully map each of the recurrent nodules, either before revision surgery or intraoperatively ( Fig. 15 ).
Cervical cysts
Cystic lesions of the head and neck do not have the same uniform etiology. Some arise from congenital connections with the aerodigestive tract and others develop from obstructing ductal structures or ill-defined degenerative processes within a solid organ or mass.
Thyroglossal Duct Cysts
Although usually midline in location, thyroglossal duct cysts can present as masses off the midline over the thyroid ala, at the thyroid notch and thyrohyoid membrane, and even in the submental triangle. These cysts may be single or multiloculated but always demonstrate the same characteristics: (1) discrete capsule, (2) anechoic echo architecture, and (3) posterior enhancement ( Fig. 16 ).
Branchial Cleft Cyst
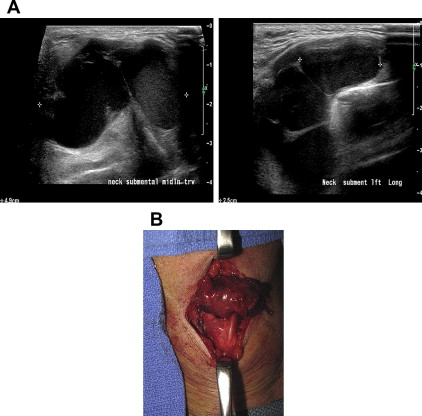
Second arch cysts are characteristically located at or near the carotid bifurcation and have the same sonographic characteristics as described for the thyroglossal duct cyst. A cyst in the upper neck, often in zone IIa, may represent degeneration of a metastatic squamous cell carcinoma to a lymph node ( Fig. 17 ). Occasionally a cyst will be identified on the left side of the neck in zone III or IV and may be associated with recurrent cellulitis or thyroiditis. Frequently, no discrete cyst is identified, only inflammation and occasionally abscess formation. Careful inspection of the area lateral to the thyroid ala and cricoid cartilage may demonstrate a fistulous tract, suggesting the likelihood of a fourth branchial pouch fistula arising from the pyriform sinus ( Fig. 18 A, B). Occasionally, fistulae can arise from the lateral wall of the hypopharynx. One clue to the proper condition may be entrapped food or vegetable matter, which produces an unusual reflective pattern (see Fig. 18 C). The ultrasound simply allows the clinician to suspect the diagnosis; esophagogram or contrast-enhanced CT swallow defines the pathology with best accuracy (see Fig. 18 D).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


