Key points
- •
Sinus surgery failure occurs most commonly in the frontal recess and is largely attributable to surgical technique.
- •
Image guidance is an extremely helpful adjunct to complete frontal recess dissection even for the most experienced surgeons.
- •
Angled 45° and 70° endoscopes significantly improve visualization.
- •
The use of through-cutting hand instrumentation is critical for sound mucosal-sparing technique to minimize scar formation.
- •
Mucosal preservation is key, regardless of technique, to ensure frontal patency.
Introduction
The frontal recess comprises the intricate outflow tract of the frontal sinus and is bordered by the agger nasi cell anteriorly, the lamina papyracea laterally, the middle turbinate medially, and the bulla ethmoidalis posteriorly. In addition, there are many unique frontal cells that add to the level of surgical complexity. Dissection in the frontal recess proposes several challenges. These challenges include significant variable anatomy, challenging visualization, narrow caliber, proximity to vital structures including the skull base and orbit, and the need for advanced instrumentation. As such, sinus surgery failure occurs most commonly in the frontal recess. Common findings at the time of revision frontal sinus surgery include edematous or hypertrophied mucosa, retained agger nasi cell, neo-osteogenesis within the frontal recess, lateral scarring of the middle turbinate, residual anterior ethmoid cells, and residual frontal cells. With the exclusion of edema and neo-osteogenesis, the remaining causes are the direct result of surgical technique. Proper instrumentation is necessary for delicate mucosal-sparing surgical technique. Here, the authors provide an overview of the current instrumentation and adjunctive technologies used commonly in complete frontal recess dissections.
Introduction
The frontal recess comprises the intricate outflow tract of the frontal sinus and is bordered by the agger nasi cell anteriorly, the lamina papyracea laterally, the middle turbinate medially, and the bulla ethmoidalis posteriorly. In addition, there are many unique frontal cells that add to the level of surgical complexity. Dissection in the frontal recess proposes several challenges. These challenges include significant variable anatomy, challenging visualization, narrow caliber, proximity to vital structures including the skull base and orbit, and the need for advanced instrumentation. As such, sinus surgery failure occurs most commonly in the frontal recess. Common findings at the time of revision frontal sinus surgery include edematous or hypertrophied mucosa, retained agger nasi cell, neo-osteogenesis within the frontal recess, lateral scarring of the middle turbinate, residual anterior ethmoid cells, and residual frontal cells. With the exclusion of edema and neo-osteogenesis, the remaining causes are the direct result of surgical technique. Proper instrumentation is necessary for delicate mucosal-sparing surgical technique. Here, the authors provide an overview of the current instrumentation and adjunctive technologies used commonly in complete frontal recess dissections.
Image guidance
Image guidance can be a helpful adjunct to frontal recess dissection even for the most experienced surgeons. Aside from providing confirmation of complete frontal recess dissection, the image-guidance system planning station can be used preoperatively to study anatomic variants and help develop a plan for intraoperative dissection. The triplanar view that an image-guidance system provides gives the surgeon additional information to safely open the sinus. Individual preference and institutional availability should guide the decision to choose between electromagnetic or optical-based systems because both systems provide comparable accuracy in anatomic localization.
Angled endoscopes
Proper visualization of is of utmost importance when performing frontal recess dissection. Although some describe frontal sinus surgery without angled endoscopes, in general, a minimum of a 30°, and preferably a 70°, endoscope is needed for adequate visualization. Reverse or offset angled endoscopes are extremely helpful. Reverse endoscopes are designed with the light-post oriented superiorly, thus allowing for easier use of curved frontal sinus instruments because the light-post does obstruct access as it does with traditional endoscopes. Irrigating lens-cleaning sheaths can also be helpful to maintain a clear field.
Hand instrumentation
The use of through-cutting hand instrumentation is critical for sound mucosal-sparing technique. A list of commonly used hand instrumentation in frontal recess dissection is listed in later discussion.
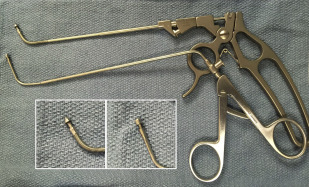
45° Mushroom Punch
The 45° mushroom (Karl Storz, Tuttlingen, Germany) punch is particularly useful to enlarge an existing opening circumferentially ( Fig. 1 ). In addition, it is the only frontal sinus hand instrument capable of removing horizontal partitions in an anterior to posterior direction in a through-cutting manner. This situation is commonly encountered in the posterior frontal recess. The Hosemann punch is similar to the 45° mushroom punch with much greater cutting strength (see Fig. 1 ). This instrument is best used for removal of osteitic bone of the frontal sinus floor.