Purpose
To determine the relationship between eyelid pressure during blinking and the fluorescein staining of the cornea and conjunctiva in dry eye patients.
Design
Cross-sectional prospective study.
Methods
The pressure of the upper and lower eyelids was measured with a specially designed blepahro-tensiometer in 130 eyes of 65 dry eye patients (D group) and in 58 eyes of 31 normal controls (N group). The correlations between the location and degree of ocular surface staining scores and the eyelid pressure were calculated for the D group.
Results
The pressures of the upper and lower eyelids were significantly higher in the D group than in the N group (upper P < .0001, lower P = .0040). The lower eyelid pressure was significantly correlated with the ocular surface staining scores for the inferior cornea (r = 0.19, P = .0307) and conjunctiva (r = 0.19, P = .0252).
Conclusions
The significant correlation between the eyelid pressure and the ocular surface staining suggests that mechanical friction on the ocular surface by the eyelids may be one of the factors that affects the fluorescein staining of the inferior ocular surface.
Dry eye disease has been defined as a disorder of the tear film caused by a deficiency in tear formation or excessive evaporation of the tears. The presence of dry eyes can damage the ocular surface and is manifested by a variety of signs and symptoms. In 2007, the International Dry Eye WorkShop defined dry eye as a “multifactorial disease of the tear and ocular surface that results in symptoms of discomfort, visual disturbances, and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.”
It is well recognized that blinking and eyelid dynamics play important roles in the distribution of tears and in the maintenance of the integrity of the ocular surface. It is also known that functional or anatomic abnormalities of the eyelids can cause ocular surface disorders, and oculoplastic surgery for abnormal eyelids can restore ocular surface integrity.
Blepharospasm is a blinking disorder characterized by repeated forceful spasmodic contractions of the orbicularis oculi muscle, and many patients with blepharospasm suffer from dry eye symptoms. However, it has not been determined whether there is a causal relationship between dry eye and blepharospasm. On the other hand, Mathers and Lemp used specular microscopy to demonstrate that the shearing force of blinking removed cells from corneal epithelium, and they suggested that the shearing forces of the eyelid movements alter the migration and turnover of epithelial cells by increasing exfoliation.
Recently, Cher proposed a new term, “blink-related microtrauma,” for ocular surface disorders arising from the mechanical friction or lubrication disorders of the eyes. Superior limbic keratoconjunctivitis (SLK) was an example of this condition. Korb and associates proposed another term, “lid-wiper epitheliopathy,” for the epitheliopathy that is characterized by staining of the conjunctival epithelium at the eyelid margin by fluorescein and/or rose bengal. They suggested that higher shear stress is generated at this region. Thus, the behavior of the eyelid on the ocular surface during blinking should have a large influence on the flux of the tears produced beneath the eyelids.
Eyelid tension or pressure is defined as the tension or pressure exerted by the eyelids on the cornea and conjunctiva. In 1869, Snellen first proposed the concept of eyelid tension and reported that it could alter the shape of the cornea. Since then, eyelid tension or pressure has been measured by various instruments that measure the tension of the eyelid on the ocular surface. However, a standardized method of measuring the eyelid tension or pressure has not been established because the methods and measuring devices were not easy to use and were not accurate.
To overcome these problems, we have developed a simple and easy-to-use eyelid pressure measurement system called a blepahro-tensiometer, which uses tactile pressure sensors. Measurements of the eyelid pressure with the blepahro-tensiometer have shown that reliable and valid measurements of the pressure of the eyelids on the ocular surface can be obtained.
The purpose of this study was to determine the effect of eyelid pressure elicited by blinking on the ocular surface, and to determine which area of the ocular surface will be affected by blinking.
Methods
Study Design
The study was approved by the Institutional Review Board of Ehime University (No. 0701006) and University Hospital Medical Information Network Clinical Trials Registry (ID number UMIN000004256). An informed consent for the examinations was obtained from all subjects, and the procedures used conformed to the tenets of the Declaration of Helsinki. This was a prospective, cross-sectional study designed to determine the relationship between eyelid pressure during blinking and the fluorescein staining of the cornea and conjunctiva in dry eye patients.
Subjects
The eyelid pressure was measured in 130 eyes of 65 dry eye patients and 58 eyes of 31 normal controls between March 2008 and November 2008 at the Ehime University School of Medicine. The dry eye group (D group) consisted of 13 men and 52 women whose average ± standard deviation age was 58.7 ± 15.0 years with a range from 19 to 91 years. The normal control group (N group) consisted of 14 men and 17 women whose average age was 51.1 ± 17.3 years with a range from 20 to 85 years.
Dry eye was diagnosed according to the 2006 revised Japanese Dry Eye Diagnostic Criteria. The revised criteria for dry eyes were: (1) presence of dry eye symptoms; (2) presence of either qualitative or quantitative disturbances of the tear film (Schirmer I test ≤5 mm or fluorescein tear break-up time [BUT] ≤ 5 s); and (3) presence of conjunctivocorneal epithelial damage (fluorescein staining score ≥3 points or rose bengal staining score ≥3 points or lissamine green staining score ≥3 points). The presence of all 3 criteria is required to establish a diagnosis of definite dry eye. Individuals with 2 positive criteria among the 3 are diagnosed with probable dry eye. Individuals with the presence of either 1 or no positive criteria are diagnosed as normal.
Cases of allergic conjunctivitis, eyelid closure failure, deformed eyelids, conjunctival concretion, or abnormal blinking disorders and cases with a history of any type of eye surgery were excluded. The differences in the age and sex distribution in the N and D groups were not significant.
Eyelid Pressure Measurements by Blepharo-tensiometer
We developed a simple and easy-to-use eyelid pressure measurement system using tactile pressure sensors (DigiTacts Single Point Sensors; Pressure Profile Systems, Inc, Los Angeles, California, USA). The pressures of the upper and lower eyelids were measured using the same sensor for each subject, as described in detail. Briefly, a sterile disposable soft contact lens (Focus Dailies -3.0 diopter; Chiba Vision, Duluth, Georgia, USA) was placed on the cornea after the eye was anesthetized with topical 0.4% oxybuprocaine (Santen, Osaka, Japan) to protect the cornea. The pressure sensor with the protective polyurethane cap (Okamoto, Tokyo, Japan) was inserted between the soft contact lens and the inner surface of the eyelid. The sensor was placed at the center of the upper eyelid and at the nasal region of the lower eyelids. The subjects were asked to close their eyes and keep their eyes closed for at least 5 seconds for the measurements. The measured pressure was divided into 2 phases: an increasing phase and a plateau phase. Then 2 best-fitting lines were drawn to fit the 2 phases, and the intersecting point was determined. The eyelid pressure was defined as the average of 150 tension values obtained during the 5 seconds after the intersection point. An ophthalmic technician was trained on the protocol for measuring the eyelid pressure, and after she became proficient with the device, she was instructed to perform the measurements.
Evaluation of Ocular Surface Staining
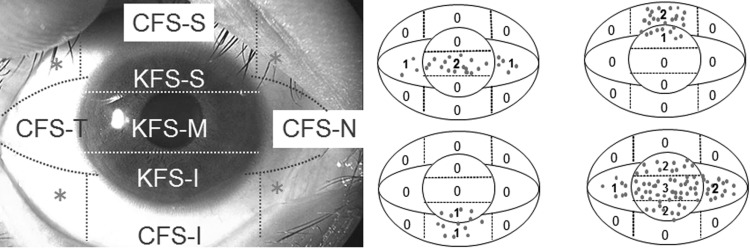
After instillation of 2 μL of 1% fluorescein Na solution into the cul-de-sac, the location and degree of the ocular surface staining were determined by slit-lamp microscopy with a yellow stop filter (Carl Zeiss Meditec, San Francisco, California, USA). The cornea and conjunctiva were divided into 7 sections ( Figure ), and the ocular surface staining was scored in each area on a scale of 0–3. Examples of the ocular surface staining scores are shown in the Figure . The corneal fluorescein staining was denoted as KFS while that of the conjunctiva was denoted as CFS. The ocular surface staining was evaluated before eyelid pressure measurements.
Evaluation of Other Factors Used to Assess Ocular Surface
We calculated the correlations between the location and scores of the ocular surface staining and other factors used to assess the condition of the ocular surface. These factors included the Schirmer I test scores (mm), fluorescein tear film BUT, meibomian gland dysfunction (MGD; grade 0–3 after Shimazaki and associates ), tear meniscus height (TMH; low/medium/high), superior conjunctivochalasis (grade 0–3 after Yokoi and associates ), inferior conjunctivochalasis (grade 0–3 after Hirotani and associates ), superior or inferior lid wiper epitheliopathy (LWE; grade 0–3 after Yamamoto and associates ), eyelid shape (1 fold/2 folds in the eyelid), and eyelid ptosis (present/absent) ( Table 1 ).
| Other Tests for Evaluating | Score |
|---|---|
| Schirmer I test | (mm) |
| BUT | (second) |
| MGD | (0–3) |
| TMH | (low / medium / high) |
| Superior conjunctivochalasis | (0–3) |
| Inferior conjunctivochalasis | (0–3) |
| Superior LWE | (0–3) |
| Inferior LWE | (0–3) |
| Eyelid shape | (1 fold / 2 folds in the eyelid) |
| Eyelid ptosis | (+/−) |
Statistical Analyses
All data are presented as the means ± standard deviations. Statistical analyses were performed with the Student t tests, Pearson coefficient of correlation, and multiple linear regression analyses. A P value <.05 was considered statistically significant. All analyses were done with JMP for Windows, Version 7 (SAS Institute, Cary, North Carolina, USA).
Results
Eyelid Pressure in Normal Eyes and Dry Eyes
The mean eyelid pressure for the normal eyes (N) group was 16.25 ± 6.18 mm Hg for the upper lid and 16.39 ± 6.82 mm Hg for the lower lid. For the dry eyes (D) group, the mean eyelid pressure was 20.23 ± 5.73 mm Hg for the upper lid and 19.55 ± 6.58 mm Hg for the lower lids. The values for both eyelids were significantly higher in the D group than in the N group ( Table 2 ; upper P < .0001, lower P = .0040). When the eyelid pressures were examined by age, no significant difference was observed between ages <39 years and and 40–49 years in the N and D groups. However, the eyelid pressures were significantly higher in the D group than the N group for the older ages, especially ages of 50–59 years ( Table 2 ; upper P = .0068, lower P = .0127) and 60–69 years ( Table 2 ; upper P = .0007, lower P = .0230). In the N group, all of the eyelid pressure values decreased with increasing age, while this trend was not observed in the D group, where the values for each age group were not significantly different, although no significant difference was observed between N and D groups in lower eyelid pressure for ages over 70 years ( Table 2 ).
| Age | ≤39 | 40–49 | 50–59 | 60–69 | 70+ | Total | ||
|---|---|---|---|---|---|---|---|---|
| Upper eyelid pressure (mm Hg) | N | 21.36 ± 5.03 | 18.86 ± 5.77 | 14.14 ± 3.95 | 11.22 ± 5.95 | 11.54 ± 3.08 | 16.25 ± 6.18 | P < .0001 b , c |
| D | 21.22 ± 4.20 | 19.38 ± 5.93 | 19.25 ± 5.24 | 21.03 ± 5.95 | 20.28 ± 6.73 | 20.23 ± 5.73 | P = .9515 b | |
| P = .9351 a | P = .8232 a | P = .0068 a , c | P = .0007 a , c | P = .0002 a , c | P < .0001 a , c | |||
| Lower eyelid pressure (mm Hg) | N | 21.72 ± 7.23 | 15.86 ± 6.41 | 13.00 ± 4.75 | 13.52 ± 7.09 | 15.43 ± 5.47 | 16.39 ± 6.82 | P = .0009 b , c |
| D | 21.91 ± 6.11 | 17.85 ± 6.99 | 18.34 ± 5.94 | 20.83 ± 6.90 | 18.90 ± 6.83 | 19.55 ± 6.58 | P b = .5527 | |
| P = .9364 a , c | P = .4573 a | P = .0127 a , c | P = .0230 a , c | P a = .1383 | P = .0040 a , c | |||
| N | 15 | 14 | 12 | 6 | 11 | 58 | ||
| D | 19 | 12 | 35 | 34 | 30 | 130 | (eyes) | |
a P values between dry eyes and normal eyes.
Effect of Eyelid Pressure and Other Ocular Factors on Ocular Surface Staining Scores in Dry Eye Patients
The ocular surface staining scores in each region are shown in Table 3 . The correlations between the ocular surface staining scores and the eyelid pressure values of each region are shown in Table 4 . The ocular surface staining scores of the inferior cornea (KFS-I) and inferior conjunctiva (CFS-I) were significantly correlated with the higher pressures in the lower eyelid (r = 0.19 and r = 0.20, and P = .0307 and P =.0252, respectively). The correlations between the upper and lower eyelid pressure values and the staining scores for the superior and middle cornea and the intrapalpebral conjunctiva were not significant ( Table 4 ).
| Section | Mean ± SD Score |
|---|---|
| KFS-S | 0.19 ± 0.48 |
| KFS-M | 0.59 ± 0.73 |
| KFS-I | 0.85 ± 0.79 |
| CFS-S | 0.42 ± 0.76 |
| CFS-T | 0.99 ± 0.74 |
| CFS-N | 1.00 ± 0.77 |
| CFS-I | 0.51 ± 0.66 |
| KFS-S | KFS-M | KFS-I | CFS-S | CFS-T | CFS-N | CFS-I | |
|---|---|---|---|---|---|---|---|
| Upper eyelid pressure | |||||||
| r | −0.14 | −0.04 | 0.10 | −0.07 | 0.11 | 0.17 | 0.06 |
| P | .1260 | .6288 | .2805 | .4537 | .2338 | .0647 | .5380 |
| Lower eyelid pressure | |||||||
| r | 0.04 | 0.06 | 0.19 | −0.05 | 0.10 | 0.13 | 0.20 |
| P | .6774 | .5333 | .0307 a | .6151 | .2858 | .1459 | .0252 a |
| Schirmer I test scores | |||||||
| r | −0.11 | −0.14 | −0.03 | −0.10 | −0.21 | −0.25 | −0.04 |
| P | .2234 | .1265 | .7489 | .2738 | .0224 a | .0068 a | .6655 |
| BUT | |||||||
| r | −0.22 | −0.04 | 0.02 | −0.27 | −0.09 | −0.02 | −0.25 |
| P | .0131 a | .6803 | .8564 | .0018 a | .3154 | .8170 | .0043 a |
| MGD | |||||||
| r | 0.30 | 0.18 | 0.19 | −0.11 | 0.21 | 0.20 | 0.19 |
| P | .0012 a | .0507 | .0435 a | .2387 | .0251 a | .0263 a | .0371 a |
| TMH | |||||||
| r | 0.13 | −0.02 | 0.00 | −0.06 | −0.11 | −0.05 | −0.02 |
| P | .1499 | .8195 | .9596 | .5038 | .2331 | .6065 | .7949 |
| Superior conjuctivochalasis | |||||||
| r | 0.12 | 0.00 | −0.03 | 0.36 | 0.02 | −0.01 | 0.03 |
| P | .1954 | .9764 | .7448 | <.0001 a | .8361 | .9016 | .7741 |
| Inferior conjunctivochalasis | |||||||
| r | −0.06 | −0.05 | 0.06 | −0.01 | 0.04 | 0.03 | 0.03 |
| P | .5237 | .5843 | .5152 | .9316 | .6218 | .7712 | .7371 |
| Superior LWE | |||||||
| r | −0.01 | −0.06 | 0.11 | −0.17 | 0.06 | 0.18 | 0.02 |
| P | .8880 | .5277 | .2054 | .0507 | .5098 | .0475 a | .7935 |
| Inferior LWE | |||||||
| r | −0.01 | 0.05 | 0.07 | −0.18 | 0.09 | 0.09 | 0.02 |
| P | .9045 | .5925 | .4335 | .0435 a | .3076 | .2954 | .8360 |
| Eyelid shape | |||||||
| r | −0.03 | 0.12 | 0.03 | −0.08 | 0.04 | 0.10 | −0.06 |
| P | .7406 | .1802 | .7792 | .3715 | .6787 | .2735 | .5005 |
| Eyelid ptosis | |||||||
| r | 0.17 | −0.07 | −0.19 | 0.23 | −0.14 | −0.14 | −0.10 |
| P | .0632 | .4406 | .0429 a | .0122 a | .1420 | .1441 | .3040 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


