Inflammatory Orbital Pseudotumors
In this chapter, we will discuss the orbital manifestations of a group of clinical entities, which, for many years, were lumped together as pseudotumors. These entities are idiopathic orbital inflammation, idiopathic sclerosing inflammation, Tolosa-Hunt syndrome, multifocal fibrosclerosis, vasculitis, and Wegener granulomatosis. Birch-Hirschfeld (1930), in the period 1905 to 1909, coined the term, pseudotumor, to describe inflammatory swellings of the orbital contents that produced proptosis and, thereby, mimicked neoplastic disorders. A reader may now assume that the term, pseudotumor, would be obsolete. However, a recent publication (1999) pertaining to the orbit includes bacterial infection, fungal infections, sarcoidosis, Erdheim-Chester disease, Sjögren syndrome, and Wegener granulomatosis under the rubric, pseudotumor.
Idiopathic Orbital Inflammation1
This idiopathic orbital inflammatory process has also been called nonspecific orbital inflammation, idiopathic inflammatory pseudotumor, and nonvasculitic inflammatory tumor. It was separated from the conglomerate of pseudotumors by several authors in the 1960s and 1970s, and is now recognized as a clinical entity.
This entity has been known for over 50 years, but its cause remains elusive. The inflammatory orbital mass is probably a cell-mediated and humeral response to a primary immunopathologic dysfunction, but the antigen is unknown. Farrow (1973), who studied the tissue specimens of our early cases, thought the histopathology was remindful of the Arthus type of hypersensitivity reaction.
Incidence
It is difficult to accurately assess this factor on the basis of a review of the literature. First, there is a lack of a universal definition. The question of just what constitutes inflammatory tumor is highly subjective, sometimes depending on an author’s predetermined notion of what its clinical presentation should be. Of greater concern is the number of case studies in the literature that are not proven by histologic study. It is disappointing to review an article with an attractive title only to find that all or most case reports are based on an assumed diagnosis. This is particularly applicable to the published reports in the pediatric and radiology literatures. Our knowledge of this lesion would be better served if such reports would base their clinical data on the surgically proven cases, even though the number of patients is small. We prefer not to reference those many reports in the literature that are not based on factual data.
In our 50-year list of orbital tumors, there are 83 patients with idiopathic orbital inflammation, an incidence of 4.6% (83/1795) of total tumors. The real incidence is probably higher because a sizable number of presumed orbital cases are never biopsied. There were 40 males and 43 females. The age range of males is 2 to 89 years with an average age of 42.3 years and a median of 44 years. The greatest concentration (16 cases) of patients is in the fourth and fifth decades at the time of presentation. The age range of female patients is 7 to 79 years with an average age of 49.6 years and a median age of 44 years. The greatest concentration (12 cases) of patients is in the fifth and sixth decades at the time of presentation. Among the overall group of 83 patients, there are 7 with bilateral involvement, age range 2 to 68 years, 5 males and 2 females. Among the 83 patients, there were only 7 (ages 2 to 18 years) children.
The bulk of the literature addresses idiopathic orbital inflammation in adults. The latest review of this inflammatory tumor in children is that by Berger et al., 1996.
 Figure 19.1 Idiopathic orbital inflammation: A 76-year-old woman with right-sided blepharoptosis, edema, and erythema of eyelids, and frontal headache of 2 months’ duration owing to a lesion in the posterior orbit. Other findings were chemosis, proptosis, ophthalmoplegia, and a visual acuity limited to recognition of hand movements by the affected eye. A subtotal removal of the inflammatory lesion was performed. The patient was followed up for 87 months. The inflammatory process subsided without further treatment, but the eye remained sightless, blepharoptosis was complete, there was very little ocular motility, and optic atrophy developed. |
Clinical Features
The idiopathic inflammatory tumor has a relatively short and aggressive onset. In our Mayo series, the duration of symptoms averaged about 5 months. This tumor, among all those described in this text, is unusual in its tendency to locate in any orbital anatomical site and affect any of the tissues within the orbital confines including the extraocular muscles, lacrimal gland (dacryoadenitis), orbital fat, the connective tissue of Tenon capsule, trochlea, the outer dural sheath of the optic nerve, and periorbita. As a rule, some combination of two of these tissue elements is affected at any given time. Rarely are all orbital tissues involved, and the eye immobile. A unilateral orbital lesion, while under treatment or observation, may become bilateral.
The signs and symptoms voiced by the patient at the time of presentation are numerous such as swelling of the upper lid, a palpable mass in the anterior orbit with or without tenderness, axial protrusion of the eye, extraocular motility impairment, pain associated with an orbital mass, drooping of upper eyelid, a red eye, erythema of the upper eyelid, and visual loss >20/200. Usually, there is a combination of two clinical features. Vision is not impaired unless there is hyperemia or pallor of the optic disk. None of these clinical features is present in all cases (see Fig. 19.1).
Imaging Aspects
The imaging display, usually computed tomography (CT), of idiopathic orbital inflammation may be nearly as diverse as its presenting symptomatology. Any orbital structure may be involved, alone, or in combination. However, regardless of location, the lesions all tend to enhance after contrast administration and show irregular margins. In their various orbital sites, the lesions are rather distinctive, but their features are not necessarily specific to inflammatory tumor.
The lacrimal gland is a frequent location of the tumor. Here, the tough capsule of the gland tends to delimit the lesion, giving the tumor a circumscribed appearance that strongly suggests an intrinsic neoplasm. More often, the configuration of the lesion will show wisps of inflammatory tissue extending outward along the fascial planes between the lacrimal gland and the eyeball.
When located in an extraocular muscle, the inflammatory lesion also may be partially delimited by the muscle sheath but less so than a lesion in the lacrimal gland. The lesion in muscle tends to spread linearly, seldom producing the bulk that is associated with the edema of Graves orbitopathy. In addition, the inflammatory tumor may involve the lateral rectus muscle or the tendinous attachment of the extraocular muscle, features not seen with Graves orbitopathy.
In the apex of the orbit, the lesion tends to extend forward like a fan, closely resembling the configuration of some meningiomas. However, the forward border of the inflammatory lesion is more irregular than in meningioma owing to tufts and threads of tissue extending out into the fascial planes of the retrobulbar space. A metastatic carcinoma may also show the same features.
A variant of the apical lesion is the perineural infiltration of the sheath of the orbital optic nerve. The linear hyperdensity of the sheath infiltration contrasts with the hypodensity of the optic nerve core, giving the CT image a “tram-track” appearance. Again, an optic nerve meningioma may produce a similar imaging sign.
A peculiar tendency of the inflammatory tumor is to encompass the posterior wall of the eyeball by an infiltration of Tenon capsule and sclera. This produces a distinctive thickening and enhancement of the scleral ring. In addition, the infiltrating tumor may extend haphazardly into the retrobulbar tissues. These imaging features may also be seen with metastatic carcinoma, orbital cellulitis, and the scleritis associated with rheumatoid arthritis.
Last, the inflammatory process may be so intense and diffuse that it fills the entire retrobulbar space with “wall-to-wall” tumor, a feature also seen in Wegener granulomatosis (WG). Figures 19.2 to 19.7 show many of the differing features of CT imaging.
In the past decade or so, there has been a steady stream of publications wherein authors state a biopsy is no longer necessary to establish the diagnosis of idiopathic orbital inflammation. We have selected several quotations from the literature pertaining to this trend such as: “In the majority of pseudotumor cases, the diagnosis can be ascertained on the basis of the clinical information and the CT findings.” “The constellation of clinical findings and the results of diagnostic and laboratory tests exclude the need for a diagnostic orbital biopsy in the majority of cases.” “Because in most instances, the diagnosis of orbital pseudotumor can be made clinically together with
ancillary ultrasonographic and radiographic studies.” We do not believe any of these statements are factual. The imagery of CT is not specific for idiopathic orbital inflammation and can also be seen with many other orbital disorders, as noted in prior paragraphs. Actually, the reports of presumed orbital inflammation simply clutter up the literature and continue to thwart efforts to more specifically define idiopathic orbital inflammation as a separate clinical entity. Perhaps, it would be better not to accept cases for publication that are not proven by biopsy.
ancillary ultrasonographic and radiographic studies.” We do not believe any of these statements are factual. The imagery of CT is not specific for idiopathic orbital inflammation and can also be seen with many other orbital disorders, as noted in prior paragraphs. Actually, the reports of presumed orbital inflammation simply clutter up the literature and continue to thwart efforts to more specifically define idiopathic orbital inflammation as a separate clinical entity. Perhaps, it would be better not to accept cases for publication that are not proven by biopsy.
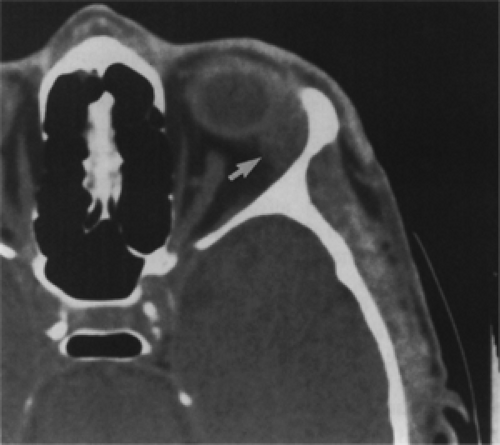 Figure 19.2 Idiopathic orbital inflammation: Axial computed tomography scan without contrast shows enlargement of the left lacrimal gland by a circumscribed homogeneous mass (arrow) in a 59-year-old man. However, the anterior and posterior borders of the lesion are not sharp. |
Pathology
Grossly, the color of the lesion is usually tan, gray, or yellow. Occasionally, the yellowish lesion may appear a bit pink, indicating a very vascular makeup. The tumors are said to be “gritty,” “rubbery,” “firm,” or “hard.”
I believe the best description of the complicated histopathology of this tumor, in the literature, is that by Spencer (1996) in his publication. The following summary is quoted directly from his text. “Edema and a polymorphic, light, inflammatory infiltrate at the early stages of the disease are highly characteristic; the infiltrating cells include lymphocytes, plasma cells, eosinophils with degranulation, and less often, polymorphonuclear leukocytes. Especially in children, whose orbital biopsies exhibit a heavy eosinophilic infiltrate, there may be an elevated absolute count of eosinophils in the peripheral blood.
As the disease progresses and fibrosis is laid down, the inflammatory cells become more widely separated by tracts of collagen, which radiate outward from the fibrous tissue septa and blood vessels into the orbital fat. The connective tissues of the muscles thicken, and hyperplasia of the periacinar and periductal connective tissues of the lacrimal gland will be observed. With progressive fibrosis, extraocular muscle degeneration occurs; the secretory acinar units of the lacrimal gland are obliterated, leading to blind-duct proliferation or hyperplasia. Once the acini of the lacrimal gland have been destroyed, they do not redifferentiate. Widely separated lymphoid follicles with germinal centers are frequently seen in the chronic stage of idiopathic orbital inflammation; this feature, combined with the presence of eosinophils, helps distinguish idiopathic orbital inflammation from thyroid-related orbitopathy. Compared to orbital lymphoid tumors, there is far more fibrosis in these tumors, and the lymphoid elements are widely separated; in other words, there is no diffuse, sheet-like hyperplasia of lymphocytes as is characteristic of the comparatively stroma-free lymphoid tumors of the orbit. Furthermore, lymphoid tumors of the orbit do not exhibit acute inflammatory signs and are generally unifocal masses rather than the diffuse or multifocal processes represented by idiopathic orbital inflammations.
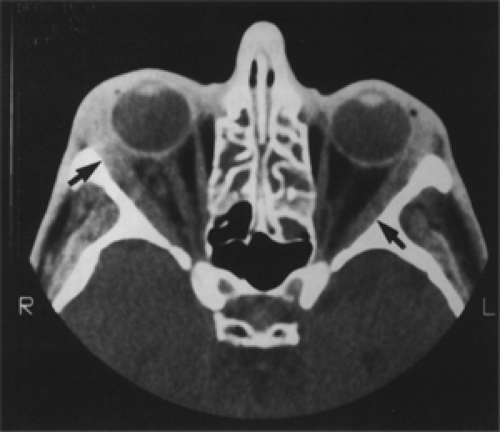 Figure 19.3 Idiopathic orbital inflammation: Presenting features in a 29-year-old man were bilateral swelling of the eyelids, palpable masses in each lacrimal gland fossa, and proptosis, more on the right side. Axial computed tomography scan shows thickening of the entire length of the lateral recti muscles by enhancing, infiltrative lesions (arrows). Surgically proved diagnosis on the right side. Postoperative radiotherapy was administered to right orbit. Two years later, exacerbation of disease occurred in the left orbit. Biopsy of left orbital lesion showed inflammatory tumor. In contrast, isolated involvement of lateral recti muscles in Graves orbitopathy is very rare. |
Evidence of perivascular lymphocytic cuffing in idiopathic orbital inflammatory pseudotumor is frequent, and occasionally eosinophils may be admixed. Such cuffing represents diapedesis of blood-borne cells into the immediate adventitial area of the capillaries or postcapillary venules; this finding, therefore, does not constitute true vasculitis.”
Another interesting finding in some of the biopsies of orbital inflammatory pseudotumor is necrosis of the orbital
fat, with a multinucleated foreign body giant cell response to the released lipid.
fat, with a multinucleated foreign body giant cell response to the released lipid.
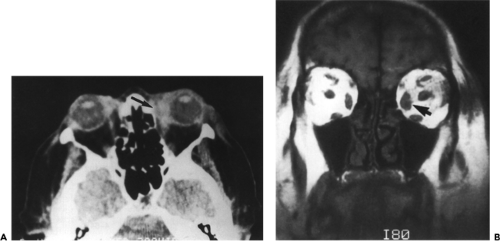 Figure 19.4 Idiopathic orbital inflammation: A: Axial computed tomography scan shows thickening and irregularity of anterior portion of left medial rectus muscle (arrow) by an infiltrating, enhancing lesion in a 67-year-old patient with pain and limited abduction of left eye. In contrast, Graves orbitopathy usually does not involve the tendinous attachment of the muscle to the globe. B: Coronal magnetic resonance T1-weighted scan shows enlargement of left medial rectus muscle (arrow). |
Figures 19.8,19.9,19.10,19.11,19.12 from the file of Mayo patients illustrate some of the salient histopathologic features.
In the study of large specimens of tissues of this inflammatory tumor removed at the time of biopsy, Farrow, in the mid 1960s, noted that intensity of the inflammatory response varied from the periphery to the center of the specimen. The inflammatory response was acute at the periphery of the specimen merging gradually into the subacute phase, and at the center of the specimen, to a chronic stage of fibrosis. The end-stage of this inflammatory process, in cases in which exenteration of the orbit was performed for relief of pain, was an eyeball encased by a mass of fibrosis and dense connective tumor that contained shrunken aggregates of lymphocytes (see Fig. 19.13). However, most biopsy tissue specimens did not show the full range of acute to chronic inflammatory stages. Instead, the inflammatory process sometimes lingered at an acute or subacute stage, or the disease process clinically came to a halt, with or without treatment, without showing features of advanced fibrosis. We found no correlation of the degree of inflammation with other clinical features of idiopathic orbital inflammation.
Alper, a retired ophthalmologist from Washington, DC (quoted by Jakobiec et al., 1984) studied a fresh surgical specimen from an orbit with this inflammatory tumor and found a predominance of B-cell lymphocytes producing the immunoglobulin that was found in the orbital tissue. If circulating immune complexes are responsible for some of these pathophysiologic changes in orbital tissues, in the manner of an Arthus reaction, these immune complexes may also be multifocal and occur in extraorbital sites such as those noted in the next section.
Immunostaining was also performed on some cases of idiopathic inflammatory tumor from our collection of cases seen in the 1990s. Most tissue specimens showed a more advanced stage of the progressive inflammatory process, that is, a subacute inflammatory stage admixed with bands of fibrous tissue replacing the stromal cellular elements, and other specimens showing a more advanced stage consisting of residual lymphoid follicles with germinal centers entrapped in a dense mass of fibrous connective tissue. All tissues, regardless of their inflammatory stage, were encompassed predominantly by B cells showing polyclonality of both κ and λ light chains. A rim of T-cell lymphocytes with predominant subsets of T cells encircled the follicle-like aggregates in the cases studied.
The presence of eosinophils in tissue specimens of idiopathic orbital inflammatory tumor has been known for many years. Noguchi et al. (1991) conducted a controlled study wherein eosinophil infiltration and extracellular major basic protein deposition were evident in all tissue specimens. The eosinophil granule is composed of several toxic cationic proteins (Gleich and Adolphson, 1986). Noguchi et al. also noted that extracellular major basic protein deposition predominated over intact eosinophil infiltration, especially in areas of fibrous connective tissue. In fact, intact eosinophils were not observed in areas of dense fibrosis. This suggests that degranulation of the
eosinophil and release of the toxic granule proteins is the major factor that contributes to fibrosis. This activation of fibrosis by extracellular deposition of eosinophil major basic protein is also seen in patients with end-stage WG and some inflammatory lesions with a major component of vasculitis.
eosinophil and release of the toxic granule proteins is the major factor that contributes to fibrosis. This activation of fibrosis by extracellular deposition of eosinophil major basic protein is also seen in patients with end-stage WG and some inflammatory lesions with a major component of vasculitis.
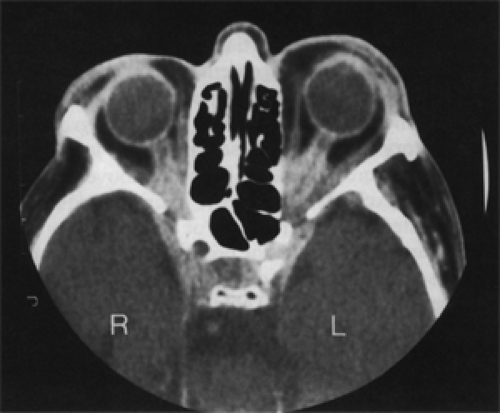 Figure 19.5 Idiopathic orbital inflammation: Bilateral, total loss of vision over a period of 1 year in a 68-year-old man. Initial, bilateral temporal artery biopsies were negative for arteritis. Axial orbital computed tomography scan shows enhancing, infiltrative masses in the apex of both orbits with extension into the adjacent cavernous sinuses. Note the “tram-track”—like enhancement of optic nerve sheath, particularly on the left side. This imaging feature may also be seen in optic nerve meningioma (compare with Fig. 18.11). Surgically proved diagnosis of inflammatory lesion on the left side. |
Management and Course
A detriment to an objective discussion of the management of this benign inflammatory tumor is lack of knowledge of the natural, untreated course of the disorder. Most of our cases were treated in some manner, but the duration of the inflammatory disease varied widely. A second problem is formulating a controlled management protocol that would include all the variables in the clinical features of the tumor: Does the tumor differ in children versus adults (considering the wide age range in adults, 21 to 89 years of age)? Can we assume the immune system is the same in individuals at these age extremes? Does the intensity of the inflammatory process differ or does it affect individual structures in the orbit (muscle, lacrimal gland, fat, dural sheath of the optic nerve, etc.) in the same way? Will it recognize differing stages of the inflammatory process (acute, subacute, or chronic)? Can it require a long follow-up (5 years) so as to include many cases that respond favorably to initial therapy with a period of assumed arrest, only to have the inflammatory process recur some months later? This is a statistical dilemma.
Table 19.1 is reproduced from our third edition published in 1994. The table lists the management and follow-up of 45 patients in the 40-year period 1948 to 1987. The size of the group of patients studied and length of follow-up time were probably unique in the literature over the 40-year period. We kept track of these 45 patients over the 40-year period and found the disease subsided in this period of observation.
 Figure 19.6 Idiopathic orbital inflammation: Axial computed tomography (CT) scan shows an enhancing mass (arrow) with an irregular border encasing the posterior wall of the eyeball, obscures the ocular optic nerve junction, and extends posteriorly along the left optic nerve in a 44-year-old woman. The same process is present along the lateral wall of the right orbit. |
The list includes nine categories of management, which, for the most part, were based on favorable reports in the literature and our own experience in any given year. There was no standard protocol. Resolution was judged by the disappearance of proptosis, eyelid swelling, and erythema, and pain, or headache. Although the orbital disease became inactive, many patients suffered permanent sequelae. If there were no sequelae or fewer residual signs of the disease when compared with presenting symptomatology, the patient was listed as “improved.” If the sequelae were roughly equal to the presenting symptomatology, excluding the above signs of resolution, the patient was listed as “unchanged.” In the “worse” category were those patients who had severe loss of both ocular motility and vision.
The patients who showed the best percentage of improvement, considering the size of the sample, were those managed either by a combination of biopsy and steroid therapy or complete excision. Complete excision of the lesion was the preferred treatment in the 1950s and 1960s, before steroid therapy came into general use. Total excision was possible if the tumor was located in the anterior orbit. Those tumors located just behind the orbital
septum, in particular, were often lobulated, circumscribed, and shelled out with careful dissection. This brought about immediate relief of proptosis and lid swelling, and these patients had no sequela. It is possible that complete excision also ablated the antigenic focus responsible for the tumor. In the one patient with visual loss, in this category, who got worse with treatment, the lesion was located in the orbital apex and was thought to be an optic nerve glioma. Accordingly, the orbital optic nerve was removed.
septum, in particular, were often lobulated, circumscribed, and shelled out with careful dissection. This brought about immediate relief of proptosis and lid swelling, and these patients had no sequela. It is possible that complete excision also ablated the antigenic focus responsible for the tumor. In the one patient with visual loss, in this category, who got worse with treatment, the lesion was located in the orbital apex and was thought to be an optic nerve glioma. Accordingly, the orbital optic nerve was removed.
Table 19.1 Idiopathic Inflammatory Tumor (N = 44) (1948–1987): Management and Residual Status of Patients with a Limited Course | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Biopsy supplemented with steroid therapy also brought early resolution of the inflammatory process and was particularly efficacious in patients having pain or headache. Biopsy and steroid therapy in the 6 patients showing improvement were effective regardless of the age of the patient, the orbital location, or the histologic stage of the lesion.
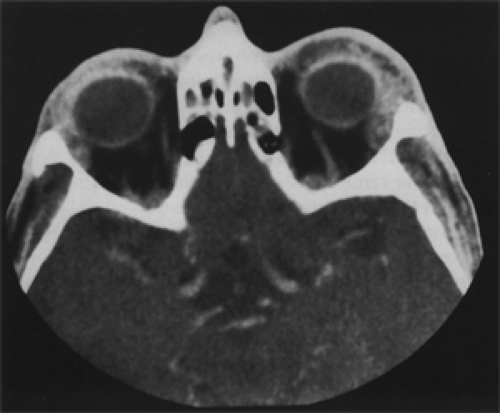 Figure 19.7 Idiopathic orbital inflammation: Axial computed tomography scan shows bilateral, diffuse, nonhomogeneous, enhancing lesions involving soft tissues of the superior orbits and lacrimal glands in a 39-year-old man. There is also some scleral enhancement. |
In less surgically accessible orbital locations, a debulking procedure (subtotal, partial, or incomplete excision) was about the only management we could offer the patient in the 1950s and 1960s. Approximately 25% (11/45) of the patients are in this group. The inflammatory tumors in these cases were less circumscribed and more infiltrative than the above cases that were totally excised. Later,
in the temporal sequence of patients, steroid therapy and/or radiotherapy were added in an effort to quiet the postoperative reaction and hurry resolution of some of these cases. Overall, in the several groups of patients whose management option included subtotal excision, the sequelae were more severe when compared to other patient subgroups that did not include the surgical debulking option. In retrospect, it is possible that incomplete removal of the orbital inflammatory focus only reactivated the immune response that was responsible for the initial lesion. The intensity of the inflammatory response and the orbital location of the tumor were also probable factors in the less favorable resolution of the disease in these patients.
in the temporal sequence of patients, steroid therapy and/or radiotherapy were added in an effort to quiet the postoperative reaction and hurry resolution of some of these cases. Overall, in the several groups of patients whose management option included subtotal excision, the sequelae were more severe when compared to other patient subgroups that did not include the surgical debulking option. In retrospect, it is possible that incomplete removal of the orbital inflammatory focus only reactivated the immune response that was responsible for the initial lesion. The intensity of the inflammatory response and the orbital location of the tumor were also probable factors in the less favorable resolution of the disease in these patients.
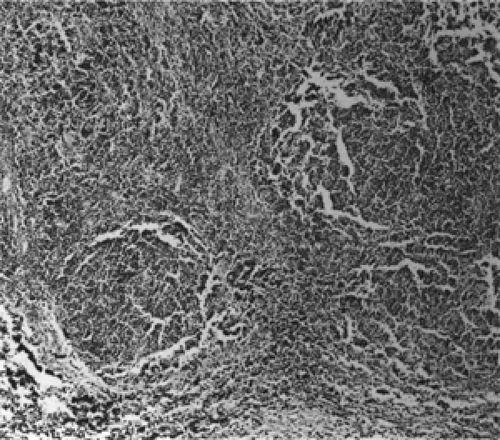 Figure 19.8 Idiopathic orbital inflammation: Diffuse, predominantly lymphocytic infiltration of orbital tissue with rounded cellular aggregates (× 64). |
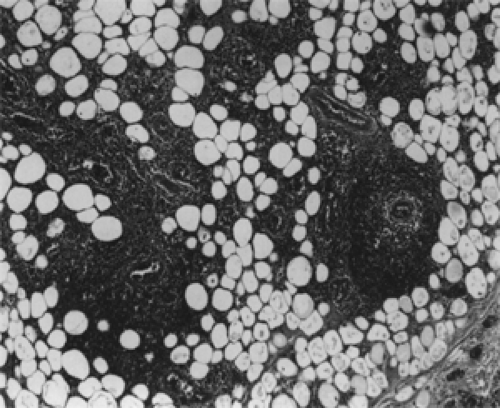 Figure 19.9 Idiopathic orbital inflammation: Dense infiltration of lymphocytes into orbital fat with marked vascular proliferation and some perivascular cellular cuffs. Fibrous tissue trabeculae lower right (× 64). |
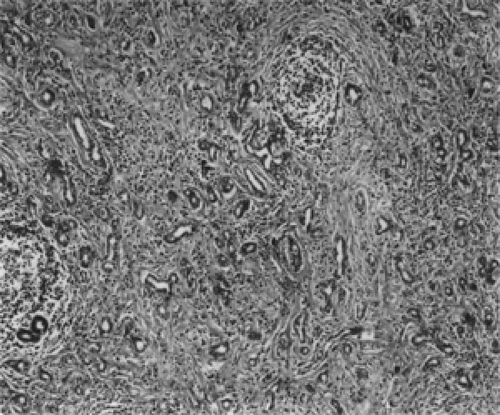 Figure 19.10 Idiopathic orbital inflammation: Fibrous tissue replacement of lacrimal gland components. Note focal lymphoid aggregates upper right and lower left (× 64).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|