Purpose
To investigate the incidence and prevalence of nonarteritic anterior ischemic optic neuropathy (NAION), and to extrapolate the risk of cerebrovascular events following NAION.
Design
Retrospective cohort study.
Methods
We identified NAION patients first, and then looked for the diagnosis of stroke after the diagnosis of NAION. Setting : The study group was composed of patients diagnosed with NAION seeking ambulatory care from 2000 to 2011. The control group was extracted from a database by randomly selecting 2 patients for every NAION patient, matched by age and sex. Main Outcome Measures : Cox proportional hazards regression analysis was performed to calculate adjusted hazard ratio (aHR) of stroke for the 2 groups. Subgroup analysis of subjects with or without comorbidities was also investigated.
Results
Four hundred and fourteen patients were included in the study group and 789 in the control group. The mean follow-up period was 5.9 years. The incidence of NAION was 3.72/100 000 person-years in Taiwan, and the prevalence of NAION was 48.18/100 000 persons. The study group was more likely to have ischemic stroke (aHR = 2.03, P = .003), but not hemorrhagic stroke (aHR = 1.24, P = .696), than the control group. Among the subgroup with comorbidities, the risk of ischemic stroke among the subjects with NAION was 3.35 times higher than those without NAION (95% confidence interval: 1.67, 6.70).
Conclusions
Patients with NAION have an increased risk of ischemic stroke. Physicians should refer all patients with NAION for systemic survey of vasculopathy and control of modifiable risk factors to prevent irreversible neurological sequelae.
Nonarteritic anterior ischemic optic neuropathy (NAION) is the second most common optic neuropathy in adults and the most common acute optic neuropathy in patients over 50 years of age, with an estimated annual incidence in the United States of 2.3-10.2 per 100 000 persons. NAION is a multifactorial disease and is characterized by visual loss and acute ischemia affecting the optic nerve head. Although the pathogenesis of NAION is unclear, the most commonly associated systemic risk factors include diabetes mellitus, nocturnal hypotension, arterial hypertension, acute blood loss, atherosclerosis, sleep apnea, cardiovascular disorders, migraine, arteriosclerosis, and type A personality.
Stroke is the second-leading cause of mortality worldwide, resulting in approximately 6 million deaths every year, and it is a major cause of long-term disability. Sixteen million people had suffered from first-ever strokes in 2005, and in the absence of any clinical interventions, it is estimated that 23 million first-ever strokes will occur by 2030. Stroke occurs when blood flow to the brain is interrupted by embolic or thrombotic occlusion of a cerebral artery (ischemic stroke) or by bleeding from a ruptured blood vessel (hemorrhagic stroke). Known risk factors for stroke include hypertension, diabetes, dyslipidemia, cardiovascular disorders, carotid artery stenosis, smoking, poor diet, physical inactivity, obesity, alcohol and drug abuse, sleep apnea, and hyperhomocysteinemia.
NAION is claimed to be pathogenetically different from stroke. Stroke is essentially caused by thromboembolism, whereas NAION is neither a thrombotic nor an embolic disease. In a prospective study of 406 patients with NAION, no increased risk of cerebrovascular disease or cardiac disease was reported. However, Hayreh found an increased risk of cerebrovascular disease developing only in those patients with NAION who had both hypertension and diabetes mellitus, which is attributable to the basic vascular changes caused by these 2 systemic diseases. Previous studies reported inconsistent results regarding the comparative risk of stroke following NAION. Guyer and associates reported that patients with idiopathic NAION and patients with systemic hypertension who developed NAION had a statistically significantly increased risk of experiencing cerebrovascular events and myocardial infarctions compared with appropriately matched control groups. Hasanreisoglu and associates concluded that following NAION, the incidence of cerebrovascular events in patients taking aspirin was not significantly higher than in risk factor–matched and age-matched controls. In addition, a literature review revealed that the systemic prognosis of patients who develop NAION remains controversial.
The aim of this study was to investigate the incidence and prevalence of NAION in Taiwan, and to extrapolate the risk of cerebrovascular events following NAION episodes, compared with the age sex matched and risk factor-medication-habits adjusted control group. In addition, we investigated whether comorbid medical disorders affected the results or not.
Methods
Data Source
The National Health Insurance (NHI) program was initiated in 1995 in Taiwan and currently covers more than 23 million enrollees, representing more than 99% of the entire population of Taiwan. This study used data from 2000 to 2011 from the Longitudinal Health Insurance Database 2005, provided by the National Health Research Institutes of Taiwan. This dataset contains the original claims data of 1 000 000 beneficiaries randomly sampled from the National Health Insurance Research Database (NHIRD) in 2005. There were no statistically significant differences in age, sex, or average insured payroll-related amount between the sample group and all enrollees. To protect privacy, individual and hospital identifiers are anonymized in the research database and therefore cannot be used to trace individual patients or health service providers. Moreover, regular cross-checks and validation of the medical charts and claims are performed by the Bureau of NHI to ensure the accuracy of diagnostic coding in the NHIRD. This study was approved by the Institutional Review Board of Tzu Chi Medical Center (IRB No.: IRB102-121).
Study Cohort and Identification of the Study Groups
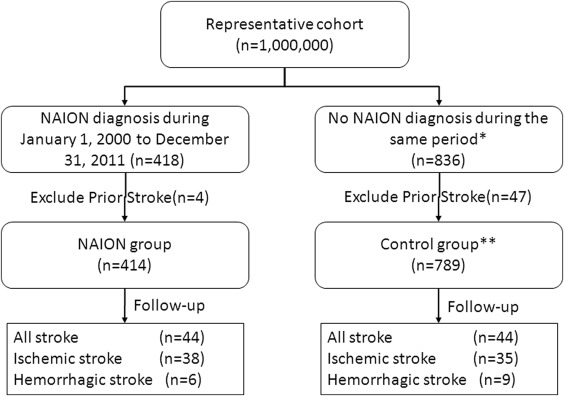
A study cohort without a previous diagnosis of NAION or history of stroke was extracted from the representative cohort. Patients with a diagnosis of NAION (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 377.41 excluding code 446.5, giant cell arteritis) from 2000 to 2011 were enrolled. The first visit with a diagnosis of NAION was defined as the index ambulatory care visit. Patients who had previously suffered any type of stroke (ICD-9-CM codes 430-438) were excluded. The control group was extracted from the subset of the NHIRD by randomly selecting 2 patients for every NAION patient, matched by exact age and sex ( Figure 1 ). Each patient was individually tracked until the end of 2011 to identify whether or not they had a stroke during the follow-up period. As there is no specific ICD-9-CM code for posterior ischemic optic neuropathy (PION), the possibility of including PION cases could not be ruled out. However, the reported relative frequencies of NAION and PION are 96% and 4%, respectively. We hypothesized the outcomes could be viewed as the effect of NAION for the most part.
Ascertainment of Covariates and Outcomes
Comorbidities including hypertension (ICD-9-CM code, 401-5.x), diabetes mellitus (code 250.x), hyperlipidemia (code 272.x), coronary heart disease (code 410-4.x or 492.2), and carotid artery disease (code 433.1) were used as covariates. These comorbidities were identified by the presence of either diagnostic codes in the outpatient records or discharge codes in the hospitalization records 6 months before the index date to the date of the outcome event or the end of follow-up. The use of statins, antithrombotics, or beta blockers for more than 1 month during the follow-up period was also included as a covariate.
The study endpoint was a stroke-related hospitalization determined by the hospitalization records with a discharge diagnostic code of stroke (ICD-9-CM code 430-5.x). All stroke events were further categorized as hemorrhagic (code 430-2.x) and ischemic (code 433-5.x) strokes in the analysis of stroke characteristics. We censored time of follow-up when the subjects died on the date of an outcome event or at the end of the study (December 31, 2011).
Statistical Analysis
All data were linked using SAS statistical software (version 9.3 for Windows; SAS Institute, Cary, North Carolina, USA) and analyzed using SPSS software version 17.0 (SPSS Inc, Chicago, Illinois, USA). Pearson χ 2 tests were used to explore differences between the study and control groups in terms of comorbid medical disorders and medications. The Kaplan-Meier method and log-rank test were used to estimate and compare the incidence rates of hospitalizations for stroke. Cox proportional hazards regression analysis was used to compute adjusted hazard ratios (aHR) for the 2 groups. A confidence level of 95% was used for this study.
Results
After exclusion of patients who had stroke history before the episode of NAION (4 in NAION group and 47 in control group), there were 414 patients (239 men, 175 women) who were diagnosed with NAION and were included in the study group. The mean age was 55.9 ± 18.6 years, and 279 patients (67%) were older than 50 years at the time of diagnosis. Seven hundred and eighty-nine subjects (461 men, 328 women) were included in the control group, with a mean age of 55.1 ± 18.4 years. The mean follow-up period was 5.9 years ( Table 1 ). Significantly more patients in the study group had comorbid medical disorders (diabetes [ P < .001], hypertension [ P = .001], coronary heart disease [ P = .001], hyperlipidemia [ P = .003]) and used medications (antithrombotics [ P < .001] and beta blockers [ P = .015]) compared with the control group ( Table 1 ).
| Variable | NAION (n = 414) | Controls (n = 789) | P Value |
|---|---|---|---|
| Follow-up period (y) | 5.7 ± 3.5 | 5.9 ± 3.4 | .155 |
| Age (y) | 55.9 ± 18.6 | 55.1 ± 18.4 | .469 |
| Male, n (%) | 239 (57.7%) | 461 (58.4%) | .854 |
| Baseline diseases, n (%) | |||
| Hypertension | 130 (31.4%) | 176 (22.3%) | .001* |
| Diabetes | 86 (20.8%) | 81 (10.3%) | <.001* |
| Hyperlipidemia | 64 (15.5%) | 76 (9.6%) | .003* |
| Coronary heart disease | 57 (13.8%) | 60 (7.6%) | .001* |
| Carotid artery disease | 0 (0.0%) | 1 (0.1%) | >.999 |
| Medication use, n (%) | |||
| Antithrombotics | 114 (27.5%) | 90 (11.4%) | <.001* |
| Statins | 40 (9.7%) | 55 (7.0%) | .115 |
| Beta blockers | 58 (14.0%) | 73 (9.3%) | .015* |
The incidence and prevalence rates of NAION were 3.72/100 000 person-years and 48.18/100 000 persons, respectively, and increased with age. The incidence and prevalence rates increased to 14.79/100 000 person-years and 235.07/100 000 persons, respectively, for those aged ≥60 years ( Table 2 ).
| Age Group (y) | Incidence (per 100 000 Person-Years) | Prevalence (per 100 000 Persons) |
|---|---|---|
| <10 | 0.55 | 6.21 |
| 10-19 | 1.32 | 17.27 |
| 20-29 | 0.82 | 10.35 |
| 30-39 | 2.30 | 28.49 |
| 40-49 | 5.22 | 65.02 |
| 50-59 | 9.44 | 117.35 |
| ≥60 | 14.79 | 235.07 |
| Total | 3.72 | 48.18 |
We first used ischemic stroke as the study outcome. The risk of ischemic stroke among the subjects aged 40-55 years was 9.8 times higher than for those aged <40 years (95% confidence interval [CI]: 1.26, 75.78), and the risk of ischemic stroke among the subjects aged >55 years was 22.5 times higher than for those aged <40 years (95% CI: 3.09, 163.31). The risk of ischemic stroke among the subjects with NAION was 2.0 times higher than in those without NAION (95% CI: 1.26, 3.25) ( Figure 2 A and B, and Supplementary Table 1 ; Supplemental Material available at AJO.com ).
Next, hemorrhagic stroke was used as the study outcome. In both study and control groups, hemorrhagic stroke was found to be rare (6 of 414 patients in the study group and 9 of 789 patients in the control group). The risk of hemorrhagic stroke among the subjects with NAION was not statistically different from those without NAION (95% CI: 0.43, 3.57). Given the low number of hemorrhagic strokes, the statistics were unstable and of limited value for reference ( Supplementary Table 1 ).
We then used all strokes as the study outcome. The risk of all strokes among the subjects with NAION was 1.9 times higher than in those without NAION (95% CI: 1.26, 2.96). The risk of all strokes among the subjects aged >55 years was 9.2 times higher than for those aged <40 years (95% CI: 2.85, 29.44) ( Supplementary Table 1 ).
Subgroup analysis was done by dividing all study subjects (study group, n = 414; control group, n = 789) into subjects without comorbidities (study group, n = 214; control group, n = 536) and subjects with comorbidities (study group, n = 200; control group, n = 253). The mean age of the subjects without comorbidities (48.8 ± 20.4 years) was statistically significantly younger than those with comorbidities (63.6 ± 12.6 years) ( P < .0001, Pearson χ 2 test). Among the subgroup without comorbidities ( Table 3 , Figure 2 C), the risk of ischemic stroke among the subjects with NAION was not statistically different from those without NAION (95% CI: 0.69, 2.80). The risk of ischemic stroke among the subjects aged >55 years was 21.0 times higher than those aged <40 years (95% CI: 2.86, 154.25). Among the subgroup with comorbidities ( Table 4 , Figure 2 D), the risk of ischemic stroke among the subjects with NAION was 3.35 times higher than in those without NAION (95% CI: 1.67, 6.70).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


