Purpose
To image the cortical vitreous, determine the prevalence of the bursa premacularis and space of Martegiani, and measure the dimensions of the bursa using the new 1050-nm swept-source deep range imaging optical coherence tomography (DRI OCT-1 Atlantis).
Design
Retrospective cross-sectional study.
Methods
One hundred and nineteen consecutive patients (5-100 years) underwent an OCT scan using 1050-nm swept-source deep range imaging optical coherence tomography. Prevalence of the bursa premacularis and space of Martegiani and the stage of posterior vitreous detachment (PVD) were determined. The horizontal (width) and anteroposterior (depth) dimensions of the bursa were recorded along with the patient’s age.
Results
A bursa was detected in 57.1% (136/238) of eyes. The bursa and space of Martegiani coexisted in 97.8% of eyes. Prevalence of detected bursa was 84.5% in eyes with either no PVD or perifoveal PVD only; the prevalence fell with further increases in the extent of PVD. Prevalence of detected bursa was 75.4% in patient group aged 0-60 years and 38% in the group aged 60-100 years. Mean width was 7001 μm (range: 3354-10 316 μm, SD: 1412 μm). Mean depth was 416 μm (range: 31-1189 μm, SD: 187 μm). Width and depth of the bursa did not correlate with age (R 2 width = 0.0316; R 2 depth = 0.0108). Bilateral bursa tended to be symmetrical in width but less so in depth (R 2 width = 0.63, P < .001; R 2 depth = 0.33, P < .001).
Conclusion
Swept-source OCT has allowed us to demonstrate the almost invariable coexistence of the bursa premacularis and space of Martegiani. Swept-source OCT can image both in patients from as early as the first to as late as the tenth decade of life.
Detailed biomicroscopic examination of the posterior vitreous gel is severely compromised by bright, diffuse light reflected from the fundus and the low optical density of vitreous structures. Indeed, the renowned biomicroscopist Vogt stated that, in his view, clinical observations in the posterior part of the vitreous are “illusory rather than real” (quoted by Hruby ). These limitations do not apply so forcibly to examination of dissected postmortem eyes, but artefacts abound from fixation (and especially from dehydration and manipulation) of the gel.
In 1814, Martegiani reported a funnel-shaped gel-free area immediately in front of the optic disc, and his identification of this posterior remnant of the primary hyaloid system (Cloquet canal) has withstood the test of time. Remarkably, however, a larger gel-free “cisterna” located within secondary vitreous in front of the macula only came to light in the 1970s. By applying white India ink to the cut vitreous surface of the posterior hemispheric calotte of fixed or unfixed globes from young adults, Worst discovered that the “heavy liquid” tended to follow selective routes or channels through the vitreous structure and entered the bursa premacularis and space of Martegiani “in a highly typical manner.” The pear-shaped bursa premacularis had a round or oval outline, centered on the fovea and extending almost to the major temporal vascular arcades; a gel septum separating the bursa premacularis from the space of Martegiani was sometimes perforated by a short channel.
That the bursa premacularis and space of Martegiani represent points of structural weakness in the cortical vitreous was confirmed in postmortem eyes by Sebag and Balazs, who suspended the vitreous body in a Lucite chamber after dissecting the gel from its scleral, choroidal, and retinal vestments. In most eyes (including from children less than 10 years of age), slit-beam biomicroscopy revealed gel herniation posteriorly through a large hole and an adjacent smaller hole in the cortical vitreous that otherwise enveloped and retained the spherical shape of the vitreous body; these holes represent artefactual ruptures in the base of the bursa premacularis and space of Martegiani, respectively. Kishi and Shimizu were later to use fluorescein staining of the gel in postmortem eyes to demonstrate the bursa premacularis and reported that this dome-shaped “pocket” was a consistent finding in individuals >65 years of age.
The presence of bursa premacularis is seen during vitrectomy procedures using triamcinolone. Spaide measured the dimension of the bursa premacularis using contact B-scan ultrasonography. Mojana and associates assessed posterior vitreous detachment (PVD) using biomicroscopy, spectral-domain optical coherence tomography/scanning laser ophthalmoscope (SDOCT/SLO), and ultrasonography. Itakura and Kishi reported that an optically empty pocket or posterior precortical vitreous pocket (PPVP) in front of the macula cannot always be imaged using Fourier-domain optical coherence tomography (FDOCT). From their series of 51 individuals aged between 8 and 65 years (in whom PVD had earlier been excluded), FDOCT failed to demonstrate a bursa premacularis in 5 people unilaterally and in another 6 bilaterally. In agreement with Itakura and Kishi, we regard the PPVP and the bursa premacularis as being the same anatomic structure.
Hence, we have undertaken a pilot study to determine whether swept-source deep range imaging optical coherence tomography will provide improved in vivo anatomic characterization of the cortical vitreous and vitreoretinal interface, and allow better insights into the dimensions and prevalence of the bursa premacularis and space of Martegiani.
Methods
This is a retrospective cross-sectional study conducted according to the tenets of the Declaration of Helsinki. All patients gave informed consent to being imaged and for the collected data to be used for publication. The Manchester Royal Eye Hospital Steering Committee did not require for this retrospective study to undergo Internal Review Board (IRB) approval as all the imaging tests carried out were part of the routine care of patients.
Two hundred forty-seven consecutive patients attending Manchester Royal Eye Hospital for the swept-source OCT examination between May 1, 2012 and December 21, 2012 were considered for entry into the study. Patients with evidence of vitreoretinal traction or myopic staphyloma, or with clear evidence of intraretinal pathology distorting the smooth concavity of the retinal surface in the posterior pole in 1 or both eyes, were excluded, as were patients in whom only 1 eye was imaged or the imaging protocol was not followed. One hundred nineteen patients (238 eyes) were thus included with age range 5-100 years. These were patients undergoing scans that met the inclusion-exclusion criteria described. Refraction and ocular axial length data were not recorded.
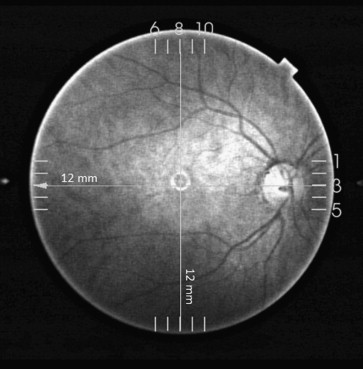
All scans were performed at Manchester Royal Eye Hospital using the new Topcon swept-source deep range imaging optical coherence tomography system (DRI OCT-1 Atlantis; Topcon). This system operates at a speed of 100 000 A-scans/second using a wavelength of 1050 nm produced by a wavelength-tunable laser as a light source. The claimed axial resolution is 8 μm, the lateral resolution is 20 μm, and the imaging depth in tissue is 2.3 mm. Scans are averaged to reduce noise. The system is equipped with a tracking system to improve reproducibility. The 12-mm-long 5-raster-line cross pattern (5 lines vertical and 5 lines horizontal) default setting was used in a vitreous focal mode ( Figure 1 ) to identify the presence or absence of a bursa premacularis and space of Martegiani in each eye for the purpose of calculating the prevalence of these features.
Contrast and brightness of the images were digitally enhanced post collection to aid the delineation of anatomic features of the cortical vitreous.
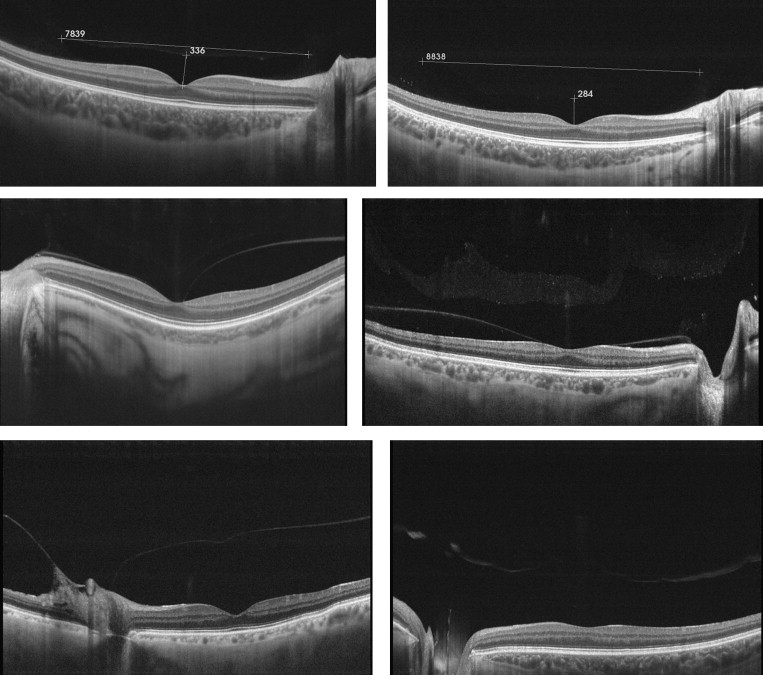
A 12-mm-long horizontal single-line scan passing through the fovea and optic disc was chosen to measure the dimensions of the bursa premacularis using the system’s caliper function at the deepest foveal point ( Figure 2 , Top left and Top right). The degree of PVD over the macula was classified using a modified version of the method of Uchino and associates, as shown in the Table .
| Stage | Stage Definition | Percentage (Eyes) in Each Stage | Prevalence of Bursa Premacularis, % (Eyes) |
|---|---|---|---|
| 0 | No PVD | 47.5% (113) | 84.3% (118/140) |
| 1 | Focal perifoveal PVD, limited to either the temporal or nasal side of the fovea, with persistent attachment to the fovea and optic nerve head | 1.7% (4) | |
| 2 | Focal perifoveal PVD, involving both the temporal and nasal side of the fovea, with persistent attachment to the fovea and optic nerve head | 9.7% (23) | |
| 3 | PVD over the fovea with persistent attachment to the optic nerve head | 10.5% (25) | 52% (13/25) |
| 4 | Complete PVD over the macula and optic nerve head | 5% (12) | 25% (3/12) |
| 5 | PVD not gradable | 25.6% (61) | 4.9% (3/61) |
Linear regression model was used to analyze the relationship between the dimensions of the bursa premacularis and age.
Results
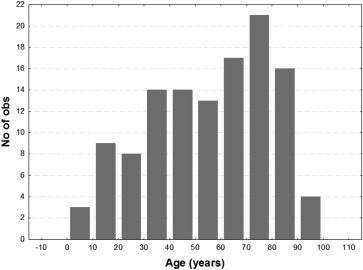
The age distribution of the patients is shown in Figure 3 . A bursa premacularis was detected in 136 out of 238 eyes (57.1%), while a bursa premacularis accompanied by a space of Martegiani was detected in 133 eyes (55.8%). The bursa premacularis and space of Martegiani coexisted in 97.8% (133/136 eyes). In the 3 eyes in which we detected a bursa premacularis with no space of Martegiani, the cortical vitreous appeared to be apposed to the surface of the optic nerve head. The bursa premacularis was detected in eyes of patients as young as 5 years of age and as old as 100 years.