Purpose
To evaluate integration of amniotic membrane into the corneal stroma using laser scanning in vivo confocal microscopy and anterior segment optical coherence tomography (AS-OCT).
Design
Prospective noncomparative interventional case series.
Methods
Twenty-two eyes of 22 consecutive patients (mean age 53.9 ± 9.2 years) presenting with noninfectious corneal ulcers and stromal thinning unresponsive to medical treatment were enrolled. Multiple layers of amniotic membrane were applied over the ulcer bed to fill the ulcer crater and held in place with an overlying amniotic membrane patch, which was anchored to the surrounding cornea with 10-0 nylon interrupted sutures. Outcome measures were healing of the corneal ulcers, corneal morphology and stromal thickness changes at the ulcer site as measured by AS-OCT and surface epithelialization, stromal repopulation, and structural modifications of the amniotic membrane grafts as evaluated by confocal microscopy.
Results
Follow-up extended to 12 months. Successful result was observed in 20 of 22 eyes (90.9%). AS-OCT showed that the mean residual stromal thickness at the ulcer bed was 222 ± 70 μm before surgery. The mean thickness of amniotic membrane layers at the same site was 394 ± 80 μm while the mean total corneal thickness was 623 ± 51 μm at day 1 post surgery. Thereafter a progressive reduction in thickness to 420 ± 61 μm at 6 months occurred, after which the thickness stabilized. Confocal microscopy showed that integration of the amniotic membrane tissues with corneal stroma was preceded by epithelialization over the amniotic membrane covering the ulcer. This occurred 15 ± 5 days post surgery in the successful cases. Confocal microscopy also showed that the amniotic membrane patch was degraded during the first few weeks after surgery, while the integrated amniotic tissues underwent progressive modifications characterized by early loss of amniotic epithelial cells, changes in fibrillar structure, and migration into the amniotic stroma by corneal stroma–derived cells.
Conclusions
Multiple layers of amniotic membrane can integrate into the corneal stroma with resulting increase in corneal thickness. This appears to be related to re-epithelialization of the transplanted membrane. Integrated amnion within the stromal defect undergoes progressive changes including contraction of tissue and repopulation by corneal stroma–derived cells.
The amniotic membrane has been used in the treatment of several ophthalmic diseases. It is composed of a thick avascular, hypocellular stromal layer and an overlying basement membrane with a single layer of epithelial cells. The biological properties attributed to amniotic membrane tissues include lack of immunogenicity; promotion of epithelialization; and inhibition of fibrosis, angiogenesis, and inflammation. The rationale of amniotic membrane transplantation onto the surface of the eye is based on the aforementioned mechanisms.
A variety of amniotic membrane grafting techniques have been proposed for the surgical treatment of different corneal and ocular surface conditions. When the membrane is used as an overlay or patch (epithelial side in contact with the corneal surface), it serves as a temporary bandage to cover inflamed or exposed areas and favorably influences epithelial healing beneath it. It also significantly reduces ocular discomfort and pain. The amniotic tissue degrades over time or may be lost as its holding sutures cut through and loosen. Alternatively, if amniotic membrane transplantation is performed with the epithelial side up (as a graft), it can act as a substrate or scaffold for corneal epithelial cells that may migrate on the amniotic membrane.
The application of multiple layers of amniotic tissue has been successfully used in patients with persistent epithelial defects, deep corneal ulcers, and perforations. Small pieces of amniotic membrane are trimmed to appropriate size and shape and stacked in layers to fill a stromal defect or facet. These may be covered by an overlying larger piece, which serves as a patch. Re-epithelialization occurs on the anterior-most layer of the stack, which then becomes incorporated into the stroma. Besides facilitating re-epithelialization, a major purpose of multilayer amniotic membrane transplantation is to achieve a stable increase in stromal thickness. Various studies in which a multilayer technique was used to treat corneal ulcers with stromal thinning reported that a stable stromal thickness at the transplant site could be restored. However, all these studies relied on slit-lamp biomicroscopy, which is very subjective and does not allow quantification or detection of subtle thickness variations. In addition, it is thought that amniotic membrane undergoes progressive modification after integration because of biological interactions between the membrane itself and the surrounding resident stromal cells. These interactions may influence tissue healing and the scar formation at the site where the amniotic membrane is transplanted. Histologic examination has revealed that the amniotic stroma becomes repopulated with corneal stroma–derived stromal cells.
The aim of the present study was to investigate, with the help of in vivo confocal microscopy and anterior segment optical coherence tomography (AS-OCT), wound healing and the integration of amniotic membrane into the corneal stroma after multilayer amniotic membrane transplantation performed for noninfectious deep corneal ulcers.
Patients and Methods
Patient Selection
Twenty-two consecutive patients (22 eyes) requiring amniotic membrane transplantation (10 male and 12 female; aged between 22 and 77 years) who attended the Cornea and Ocular Surface Division of the Ophthalmic Clinic (University “G. d’Annunzio – Chieti-Pescara, Italy) because of persistent epithelial defect with stromal ulceration, nonresponsive to conventional treatment, with progressive worsening of the ulcer, were enrolled. Conservative treatment included preservative-free lubricants, therapeutic bandage contact lenses, and autologous serum eye drops. Cases with clinical or microbiologic signs of active corneal infection were not included in this study. A detailed clinical history was recorded.
The indication for multilayer amniotic membrane transplantation was persistent corneal epithelial defect with stromal ulceration associated with the following diseases: 9 patients had immune-mediated corneal ulcerations, 9 had neurotrophic keratitis, and 4 had keratoconjunctivitis sicca.
Underlying causes for immune ulcerations were ocular graft-versus-host disease (n = 4), rheumatoid arthritis (n = 4), and vernal keratoconjunctivitis (n = 1). The neurotrophic ulcerations were secondary to herpes simplex keratitis (n = 3), diabetes mellitus (n = 4), and trigeminal nerve damage following removal of acoustic neuroma (n = 2). Persistent epithelial defects were unresponsive to conventional treatment for at least 3 weeks before amniotic membrane transplantation (average 4.04 ± 0.84 weeks). The demographic and clinical data are summarized in Table 1 . None of the patients showed signs of limbal stem cell disease as determined by clinical examination and by impression cytology.
| Patient | Gender | Age | Causes of Ulcer | Eye | Duration ofUlcer (Weeks) | Associated Ocular Surface Problems | Depth of Ulcer (%) a | Number of AMT Layers | Epithelial Healing (Days) | Complications | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 47 | KCS | OS | 4 | Inflammation | 50 | 3+1 | 15 | − | Success |
| 2 | Male | 46 | GVHD | OD | 5 | Dry eye | 80 | 5+1 | 21 | − | Success |
| 3 | Female | 22 | VKC | OS | 3 | Inflammation | 50 | 3+1 | 7 | − | Success |
| 4 | Male | 50 | HSK | OD | 4 | Dry eye | 30 | 2+1 | 15 | Patch lost | Success |
| 5 | Female | 46 | KCS | OD | 5 | Inflammation | 50 | 3+1 | 21 | − | Success |
| 6 | Female | 48 | RA | OD | 3 | Trichiasis | 50 | 4+1 | 15 | − | Success |
| 7 | Male | 55 | GVHD | OS | 4 | Dry Eye | 70 | 5+1 | 28 | − | Success |
| 8 | Male | 46 | HSK | OD | 4 | Keratouveitis | 40 | 3+1 | 21 | − | Success |
| 9 | Female | 42 | AN | OS | 5 | Lagophthalmos | 40 | 3+1 | 15 | − | Success |
| 10 | Female | 60 | RA | OD | 3 | Episcleritis | 80 | 5+1 | 7 | − | Success |
| 11 | Male | 55 | DM | OD | 6 | Stromal scar | 50 | 4+1 | 15 | − | Success |
| 12 | Female | 53 | RA | OS | 3 | KCS | 60 | 4+1 | 15 | − | Success |
| 13 | Female | 68 | DM | OS | 4 | KCS | 70 | 3+1 | 7 | − | Success |
| 14 | Male | 70 | GVHD | OS | 5 | Dry eye | 70 | 4+1 | − | AM detachment | Failure |
| 15 | Female | 63 | KCS | OD | 3 | − | 40 | 3+1 | 15 | − | Success |
| 16 | Female | 72 | RA | OS | 4 | Dry eye | 70 | 3+1 | 15 | − | Success |
| 17 | Male | 76 | DM | OD | 4 | Ectropion | 40 | 2+1 | 7 | − | Success |
| 18 | Male | 71 | GVHD | OD | 5 | Dry eye | 70 | 4+1 | 21 | − | Success |
| 19 | Male | 77 | DM | OS | 4 | Inflammation | 60 | 3+1 | 15 | − | Success |
| 20 | Female | 55 | KCS | OS | 3 | − | 70 | 4+1 | 15 | − | Success |
| 21 | Female | 59 | HSK | OD | 4 | Inflammation | 60 | 3+1 | − | Early recurrence | Failure |
| 22 | Female | 67 | AN | OD | 4 | Lagophthalmos | 80 | 5+1 | 15 | − | Success |
| Mean | 56.72 | 4.04 | 55.45 | 4.45 | 15.25 | ||||||
| SD | 13.25 | 0.84 | 15.65 | 1 | 5.46 |
a The depth of the ulcer in percentage was calculated by anterior segment optical coherence tomography scan, measuring the residual stroma at the bottom of the ulcer, as compared to normal corneal thickness in adjacent healthy areas.
Amniotic Membrane Transplantation
Cryopreserved amniotic membrane was obtained from either National L’Aquila Eye Bank or Rome Eye Bank (Italy). Human amniotic membrane was prepared and preserved by a previously described method, with minor modifications. In brief, human placenta was obtained from women undergoing elective cesarean section. All donors were screened for HIV, hepatitis B and C viruses, and syphilis. Under a lamellar flow hood the placental blood clots were washed off with sterile saline solution and the amniotic membrane was separated from the chorion by blunt dissection and samples taken for microbiology to assess sterility. The amnion with epithelial side up was flattened onto a nitrocellulose paper and then stored in sterile vials containing RPMI media (Sigma-Aldrich, St. Louis, Missouri, USA) at -80°C. All operations were performed by 1 surgeon (M.N.) using peribulbar anesthesia.
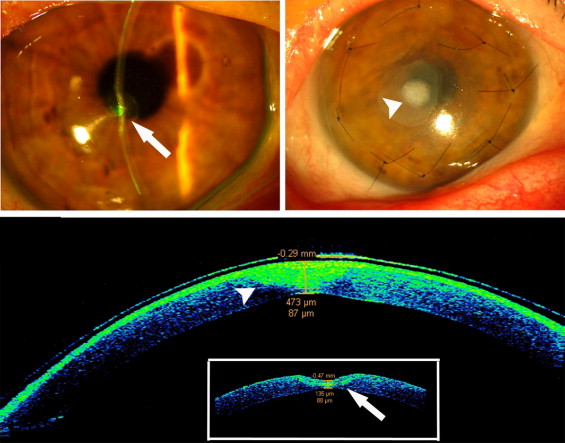
Multilayer amniotic membrane transplantation was performed in all cases following a previously described method, with minor modifications. Briefly, necrotic debris from the base and wall of the ulcers was removed with a cellulose swab. Loose epithelium from the ulcer rim was removed with a blunt spatula and fine forceps. A 1- to 2-mm zone around the ulcer was also denuded of epithelium to expose the Bowman zone, which provided a firm base for attachment of the amniotic membrane. With a Vannas scissors, amniotic membrane pieces were tailored to size and shape to fit the ulcer base and stacked in the ulcer crater, epithelial side up, to completely fill the defect (amniotic filling). Depending on the depth and configuration of the ulcer, 2 or more (up to 5) amniotic membrane pieces were required. A larger piece of membrane graft was placed on the filling layers. This was trimmed to be just smaller than the de-epithelialized area and left unsutured ( Figure 1 ) in selected cases where the de-epithelialized zone surrounding the ulcer was larger than 1 mm, or sutured with 6 interrupted 10-0 nylon sutures. An additional amniotic membrane layer, larger than the de-epithelialized zone, with the epithelial side up, was used to cover the entire area and was secured to the healthy corneal tissue surrounding the ulcer with 6 or more interrupted 10-0 nylon sutures. At the end of surgery a soft therapeutic contact lens was applied onto the surface of the eye. All patients received topical dexamethasone 0.15% and ofloxacin 0.3% 4 times daily until complete epithelialization was noted. After healing and suture removal, topical antibiotics were discontinued and the topical steroid was tapered over a 4-week period.
Postoperative Examinations and Outcome Measures
The clinical healing after amniotic membrane transplantation was estimated by slit-lamp biomicroscopy including standard photography performed on all eyes before surgery and at 1, 7, 15, 21, and 30 days and 3, 6, and 12 months postoperatively. Surgical success was defined as the complete epithelialization of the cornea and stabilization of stromal thickness. Failure was defined as persistence or recurrence of the ulcerative lesion, premature dissolution of the amniotic membrane, or the lack of epithelial or stromal healing.
At the same time points, morphologic analyses using laser scanning in vivo confocal microscopy and AS-OCT were also performed. AS-OCT was also used to assess preoperative worsening of the corneal ulcerations, therefore defined as “nonresponding” to conventional therapy in the cases enrolled (data not shown). AS-OCT examinations were carried out by 2 expert examiners masked to the details of the surgical procedures.
In Vivo Confocal Microscopy
The entire area of the stromal defect treated with amniotic membrane transplantation in each eye was examined with a digital corneal confocal laser-scanning microscope (HRT II Rostock Cornea Module, diode-laser 670 nm; Heidelberg Engineering GmbH, Heidelberg, Germany) at each follow-up date as indicated above. All confocal microscopy examinations were performed through the bandage contact lens on the cornea. The confocal laser scanning device is equipped with a water immersion objective (Zeiss, Jena, Germany; 63×/N.A. 0.95 W) and allows for an automatic z-scan determination of depth of focus within the cornea, enabling the collection and storage of high-contrast digital images, 300 × 300 μm in size, of all corneal layers. The theoretical confocal section thickness is approximately 10 μm. This is the volume (voxel), which is imaged by the confocal microscope to form a 2-dimensional pixel-based digital image. The lateral and transverse resolution is 4 μm each.
In vivo confocal microscopy was carried out under topical anesthesia with 0.4% oxybuprocaine. Proper alignment and positioning of the head was maintained with the help of a dedicated movable target red fixation light for the contralateral eye. A digital camera mounted on a side arm provided a lateral view of the eye and objective lens to monitor the position of the objective lens on the surface of the eye. A drop of 0.2% polyacrylic gel served as coupling medium between the polymethyl methacrylate contact cap of the objective lens and cornea (contact lens).
Sequential images derived from automatic scans and manual frame acquisition throughout the area of interest were obtained with emphasis on visualizing the amniotic membrane structures, stromal layers, and site of corneal re-epithelialization, according to a previously described protocol. The “section mode” function of the instrument helped to search for amniotic membrane tissues and corneal epithelium, enabling instantaneous imaging of a single area of the cornea at a desired depth. At least 30 images of the area of the cornea were obtained for each eye. At time points when epithelialization of the amniotic membrane was evident, corneal epithelial cell density was calculated using the analysis software of the instrument, by averaging numbers of cells from 5 images (randomly selected from the recorded images), counted manually within a region of interest of standardized dimensions (250 × 250 μm). Also, visible and discernable cells within the amniotic membrane tissue filling the ulcer were counted using the same method. Cell densities are given as cells per square millimeter (cells/mm 2 ).
Anterior Segment Optical Coherence Tomography
AS-OCT (Visante OCT; Carl Zeiss Meditec, Dublin, California, USA) was used to assess morphology and morphometry at the site of corneal ulcer both preoperatively and after multilayer amniotic membrane transplantation, using the high-resolution cornea mode of the instrument and digital micrometric calipers for distance measurements. The anterior segment OCT uses a wavelength of 1.3 μm, the high-resolution corneal scanning mode provides 512 A-scans per line sampling with a scan acquisition time of 0.25 seconds per line, and the reported axial resolution of 18 μm allows the accurate identification of tissue planes and measurement of lamellar thickness. Four equally spaced radial scans along the meridians of the ulcer were carried out for each eye and fixation monitored throughout. Attention was paid to preoperatively identify the ulcer profile and corresponding thinnest stromal area and to detect the amniotic membrane graft filling the ulcer cavity as presented in Figure 1 . In each scan the digital side camera of the instrument displaying the patient’s eye enabled such localization. By using dedicated calipers the identified thinnest point of the residual stromal thickness at the ulcer bed before surgery and the thickness of the amniotic membrane tissues filling the stromal defect, as well as the changes of the entire corneal thickness at the ulcer site over the healing period, were recorded.
Statistical Analysis
To assess the differences between preoperative and postoperative values we used paired Student t tests for means, and to assess differences of the parameters over time we used ANOVA test for repeated measures. The Tukey post hoc test was used to detect statistically significant differences between values at various time points. A P value less than .05 was considered statistically significant. Statistical analysis was performed with SPSS 11.5 for Windows (SPSS Inc., Chicago, Illinois, USA). Data were expressed as means ± standard deviation (SD) and P value of less than .05 was considered statistically significant.
Results
Slit-Lamp Examination
Surgical success was obtained in 20 out of the 22 cases enrolled in the study ( Table 1 ). We did not observe adverse effects or complications such as infection, perforation, hypopyon, or increased inflammation in any of the cases. Sutures and contact lens were removed between 3 and 5 weeks after surgery. The epithelial defect had healed in the 20 successful cases ( Table 1 ). In vivo confocal microscopy examination had already demonstrated complete re-epithelialization. By this time the external amniotic membrane had almost completely disintegrated in all cases. Stromal inflammation and edema had subsided within the first 2 to 3 weeks after surgery and an increase in stromal thickness, related to the integration of the transplanted amniotic tissue, at the ulcer site was observed in all successful cases. A stable stromal scar at the ulcer site where the amniotic membrane layers had integrated was noted starting from 3 months after surgery with progressive partial restoration of transparency up to 12 months after surgery.
Two representative clinical cases are depicted in Figures 2 and 3 .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


