Purpose
To compare effective phacoemulsification time in cataract surgery performed by manual phacoemulsification vs femtosecond laser-assisted lens fragmentation.
Design
Retrospective, consecutive, nonrandomized, comparative case series.
Methods
The setting was the Department of Ophthalmology, Goethe-University, Frankfurt, Germany. The study population included 150 eyes of 86 patients with senile cataract. In the intervention, 88 eyes (group 1) underwent femtosecond laser-assisted surgery (corneal incisions, capsulotomy, lens fragmentation) using the LenSx platform (Alcon) and residual lens work-up with pulsed ultrasound energy (Infiniti Vision System; Alcon). In 62 eyes (group 2), complete cataract removal was performed with phacoemulsification only, using pulsed ultrasound energy with the same device (Infiniti). Nucleus staging (Pentacam nucleus staging; PNS) was evaluated using Pentacam HR (Oculus); endothelial cell density was measured using specular microscopy (NonCon Robo). The main outcome measures were as follows. Mean preoperative PNS staging was assessed using an automatic ordinal scaling (PNS-O, grades 0–5) and a manually defined density grid derived from Scheimpflug imaging (PNS-P [%]). Effective phacoemulsification time and endothelial cell loss were evaluated in both groups.
Results
Preoperative PNS-O and PNS-P showed no significant difference between groups ( P = 0.267). Overall mean effective phacoemulsification time was significantly lower in group 1 (1.58 ± 1.02 seconds) compared to 4.17 ± 2.06 seconds in group 2 ( P = 0.001). Effective phacoemulsification time was significantly lower in group 1 for all PNS-O stages ( P < 0.001). With increasing preoperative PNS-P, effective phacoemulsification time increased in both groups; however, this gain was noticeably, but not significantly, lower in group 2. Endothelial cell loss was significantly lower in group 1 ( P = 0.02).
Conclusions
Femtosecond laser-assisted cataract surgery allows a significant reduction in effective phacoemulsification time, which correlates positively with the preoperative lens opacity.
Femtosecond lasers are capable not only of cutting the corneal surface as in femtosecond laser-in-situ keratomileusis, keratoplasty or inlay implantation, but also of cutting into deeper structures, such as the crystalline lens and the anterior and posterior lens capsule to facilitate lens fragmentation and capsulotomy in cataract surgery and refractive lens exchange.
Standard capsulotomy is performed by using forceps or needles. Ensuring predictability and repeatability in the centration and diameter of the capsulotomy can be a challenge when using this method. The following manual phacoemulsification is performed using ultrasound to emulsify and aspirate the crystalline lens. The ultrasound energy can damage surrounding structures such as corneal endothelial cells.
Recent trials indicate that a precise and well-performed capsulotomy by a femtosecond laser can improve lens surgery by means of lens fragmentation, capsulotomy or lens positioning. In clinical trials it has been demonstrated that the general reduction of ultrasound energy in phacoemulsification, depending on the stage of lens opacity, can reduce the risk for lens capsule complications and corneal endothelial injury.
Preoperative cataract staging in these trials is performed primarily using the subjective Lens Opacities Classification System III. This grading shows a positive correlation between phacoemulsification time and power.
The aim of this study was to assess preoperative cataract grades in manual and femtosecond laser-assisted cataract surgery and to evaluate its influence on effective phacoemulsification times. Secondary endpoints were the evaluation of endothelial cell loss and intraoperative complications during femtosecond laser-assisted cataract surgery.
Methods
One hundred fifty eyes of 68 patients with senile cataract were enrolled in this retrospective, nonrandomized cases series between September 2012 and May 2013. This retrospective review of patient data was approved by the ethics committee of the Goethe-University Frankfurt, Germany, and was conducted according to the Declaration of Helsinki.
Exclusion criteria were a history of pseudoexfoliation syndrome, past glaucoma filtration surgery, optic atrophy, ocular tumors, prior vitrectomy, or cataract/refractive lens surgery and central corneal scarring.
Cataract Grading
The Pentacam HR Scheimpflug imaging was used for cataract grading (Pentacam nucleus staging [PNS]) (Pentacam; Oculus, Wetzlar, Germany). The Pentacam densitometry software evaluates the lens’s optical densities by analyzing backward scatter. An automatic alignment of the Pentacam nucleus staging was performed in all preoperative cases after instillation of mydriatic eye drops (tropicamide 5 mg/mL) (Mydriatium Stulln UD; Pharma Stulln, Stulln, Germany). To guarantee comparability we analyzed distinctive images: for the right eye 90°–270° and for the left eye 270°–90°. The software allows an automatic export of the average opacity of a 3-dimensional reference block with fixed positions and fixed curvature within the Scheimpflug image of the lens. The software then evaluates automatically a grade between 0 and 5. We refer to this grading as PNS-O because it uses an ordinal scale.
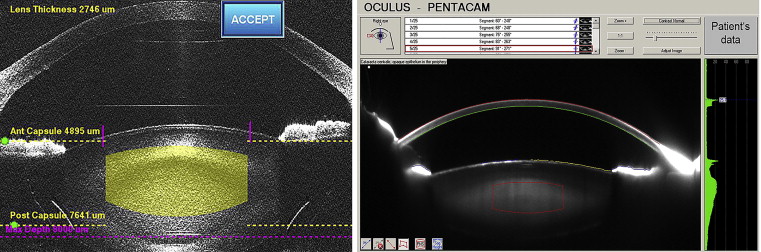
Additionally, a region of interest was manually selected in the preoperative Scheimpflug images to encompass as much of the lens nucleus as possible without including the cortex. ( Fig. 1 , left) This region of interest was centralized in the Scheimpflug lens imaging and was set in all cases to a diameter of 2500 μm, a height of 1500 μm, and an anterior/posterior curvature of 4 dimensions. By applying these default values postoperatively to the preoperative Scheimpflug images, it was ensured that the dimensions of the region of interest was within the planned lens fragmentation zone in femtosecond-laser assisted surgery (group 1), as well as being measured and verified by the implemented optical coherence tomography (OCT) system ( Fig. 1 , right). The measured density of the region of interest is expressed as a percentage, with 100% as the maximum of lens opacification. We refer to this staging as PNS-P because percentages are given.
Surgery
All surgeries were performed by the same surgeon (T.K.) under topical anesthesia with oxybuprocainhydrochloride (Conjucain, 4.0 mg/mL unit dose ampules) eye drops (Dr. Mann Pharma, Berlin, Germany).
In group 1 (88 eyes of 55 patients) femtosecond laser-assisted cataract surgery was performed using the LenSx femtosecond laser (Alcon Laboratories, Fort Worth, TX, USA). The LenSx laser is a 50 kHz infrared laser with a pulse width of 600–8002 femtosecond, a central laser wavelength of 1030 nm and a maximum pulse energy of 15 μJ. Corneal applanation was performed using the SoftFit interface (Alcon Laboratories, Fort Worth, TX, USA), consisting of a curved interface and a contact lens. The interface surface had a diameter of 10.8 mm and a curvature of 8.3 mm. Once limbal suction was confirmed, alignment of the procedural settings, ie, corneal incisions, capsulotomy and lens fragmentation parameters, were visualized by spectral domain OCT. After manual verification of each procedural step, laser treatment was performed. Primary corneal incisions were set between 2.2 and 2.4 mm; the attempted capsulotomy diameter was 5.0 mm in all cases. A standardized lens-softening pattern (3 cross-sections with a chop diameter of 4.8 mm and 1 central chop cylinder with a diameter of 2 mm) was used. The laser pulse energy was set to 7 μJ for corneal incisions and 5 μJ for capsulotomy and lens fragmentation ( Table 1 ).
| Parameters | Value | |
|---|---|---|
| Corneal incisions | Incision width (mm) | 2.2 or 2.4 |
| Pulse energy (mJ) | 7.0 | |
| Spot separation (μm) | 4.0 | |
| Layer separation (μm) | 4.0 | |
| Capsulotomy | Capsulotomy diameter (mm) | 5.0 |
| Pulse energy (mJ) | 5.0 | |
| Spot separation (μm) | 4.0 | |
| Layer separation (μm) | 3.0 | |
| Lens softening | Chop diameter (mm) | 4.8 |
| Cylinder diameter (mm) | 2.0 | |
| Number of cuts/cylinders | 3/1 | |
| Pulse energy (mJ) | 5.0 | |
| Spot separation (μm) | 10.0 | |
| Layer separation (μm) | 12.0 |
Group 2 (62 eyes of 31 patients) underwent conventional cataract surgery with continuous curvilinear capsulorrhexis using rhexis forceps before phacoemulsification.
In both groups, after hydrodissection, phacoemulsification was performed using the same machine (Infiniti; Alcon), and the same-sized phacoemulsification tip (45° Kelman, 0.9 mm Turbosonics Mini-Flared ABS Tip; Alcon). The anterior chamber was filled with a viscoelastic solution (Provisc; Alcon), and lens segmentation was undertaken in both groups using a divide-and-conquer approach.
Finally, both groups underwent foldable intraocular lens implantation in the capsular bag after successful removal of the lens cortex. Intraoperative complications such as capsulotomy tags, anterior capsule tears, posterior capsule tears, and posterior capsule ruptures were recorded.
The effective phacoemulsification time is determined by multiplying the total phacoemulsification time by the average percentage power used and represents how long the phacoemulsification time would have been if 100% power in continuous mode had been used (effective phacoemulsification time = phacoemulsification time in seconds multiplied by the average phacoemulsification power in percentage points).
Furthermore, central endothelial cell count was measured preoperatively and 1 month after surgery using specular microscopy (NonCon Robo CA, Konan Medical USA, Irvine, CA, USA).
Statistical Analysis
Statistical analysis was performed using SPSS (v 21.0; IBM Corporation, New York, USA) and BiAS for Windows (Epsilon Verlag, Mannheim, Germany). A Fisher exact test was used for a comparison of the baseline demographics and the clinical characteristics between groups. The t test and the Wilcoxon signed rank test were used to compare the sample means of PNS-O and PNS-P. Associations between effective phacoemulsification time and PNS-P were evaluated using Spearman correlation and regression analysis. Regressions were then compared. A P value of less than 0.05 was considered statistically significant.
Results
The baseline study population characteristics were similar in the 2 groups ( Table 2 ). PNS-P at baseline was not significantly different in the groups ( P = 0.267). A maximum PNS-P of 30% was measured. No intraoperative adverse complications were documented in either group. In group 1, the mean lens fragmentation thickness, measured by OCT implemented in the laser system, was 3401.48 ± 401.12 μm.
| Variable | fs-Laser-Assisted Cataract Surgery (group 1) | Manual Cataract Surgery (group 2) | P Value |
|---|---|---|---|
| Eyes (male/female) | 88 (45/43) | 62 (24/38) | – |
| Age | 67.75 ± 11.29 | 69.42 ± 12.56 | ns |
| Cataract staging (PNS mean) | 1.89 ± 0.64 | 2.02 ± 0.98 | ns |
| BCVA (logMAR) | 0.6 ± 0.21 | 0.6 ± 0.18 | ns |
| Intraocular pressure | 14.75 ± 1.38 | 13.80 ± 1.67 | ns |
| Keratometry | 44.33 ± 1.45 | 45.86 ± 1.32 | ns |
| Axial length | 23.33 ± 1.32 | 23.08 ± 1.05 | ns |
| Anterior chamber depth | 3.15 ± 0.49 | 3.04 ± 0.35 | ns |
| Endothelial cell count (cells/mm 2 ) | 2444.65 ± 307.87 | 2548.48 ± 280.87 | ns |
a Cataract stages were assessed before surgery using the Pentacam Nucleus staging method of the Pentacam device to compare effective phacoemulsification time between groups. No significant differences in baseline data between groups were shown.
The mean overall effective phacoemulsification time was significantly lower in the femtosecond group when compared with the manual group (1.58 ± 1.02 vs 4.17 ± 2.06 seconds), P = 0.001 ( Fig. 2 ). The reduction in mean effective phacoemulsification time was significant for all PNS-O grades between groups ( P = 0.01) ( Fig. 3 ). There was a relatively strong positive correlation between cataract grade assessed by PNS-O evaluation and effective phacoemulsification time (r = 0.527, P = 0.0001, Spearman rank correlation; Fig. 3 ). The analyzed region in Scheimpflug images also showed a significant correlation between PNS-P and effective phacoemulsification time (r = 0.492) ( Fig. 4 ). There were 15 (17%) cases in group 1 with effective phacoemulsification times lower than 0.5 seconds compared with no cases in group 2 ( P = 0.0001).



