In this article, computed tomography and magnetic resonance imaging anatomy and pathology of sinus disease is discussed, specifically relating to facial pain, rhinogenic headache, and sinus outflow obstruction. Findings commonly seen in acute, chronic, infectious, and inflammatory sinusitis are illustrated, with additional examples of secondary intracranial and orbital involvement, and more aggressive infectious and neoplastic processes.
Key points
- •
Computed tomography is the primary modality for imaging the paranasal sinuses, as it optimally delineates bony anatomy and can provide an accurate roadmap before surgery.
- •
Magnetic resonance imaging is superior in assessing the extent of involvement of intracranial, intraorbital, or deep fascial soft tissues in complicated cases.
- •
Basic knowledge of the primary sinus outflow tracts is crucial to understanding the pathology of sinus disease.
- •
Though relatively rare, aggressive infectious and neoplastic processes can occur within the paranasal sinuses, which may initially present with rhinogenic headache.
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| OMC | Osteomeatal complex |
| FESS | Functional endoscopic sinus surgery |
Introduction and overview
When patients referred to otolaryngologists with headaches of suspected rhinogenic or paranasal sinus–related origin are imaged, the neuroradiologist’s job is to define anatomy, characterize any potential obstructive abnormality, screen for underlying neoplasm or destructive process, and evaluate for associated involvement of adjacent orbital, intracranial, and deep facial structures. Although radiographic imaging of the paranasal sinuses is generally not necessary for patients who meet clinical criteria for uncomplicated rhinosinusitis, imaging proves useful in defining the anatomy of the sinuses before surgery and in aiding the management of chronic or recurrent rhinosinusitis.
Introduction and overview
When patients referred to otolaryngologists with headaches of suspected rhinogenic or paranasal sinus–related origin are imaged, the neuroradiologist’s job is to define anatomy, characterize any potential obstructive abnormality, screen for underlying neoplasm or destructive process, and evaluate for associated involvement of adjacent orbital, intracranial, and deep facial structures. Although radiographic imaging of the paranasal sinuses is generally not necessary for patients who meet clinical criteria for uncomplicated rhinosinusitis, imaging proves useful in defining the anatomy of the sinuses before surgery and in aiding the management of chronic or recurrent rhinosinusitis.
Basic imaging anatomy and standard imaging techniques
Understanding the normal anatomic and physiologic outflow pathways of mucociliary clearance from the paranasal sinuses is essential to identifying and accurately delineating the pathogenesis of rhinosinusitis, and ultimately to restoring physiologic drainage patterns via functional endoscopic sinus surgery (FESS). Key to this are the frontal recess, sphenoethmoid recess, and the ostiomeatal complex (OMC), which refers to the maxillary sinus ostium, the infundibulum, the uncinate process, hiatus semilunaris, the ethmoid bulla, and the middle meatus. Together, the components of the OMC provide the common drainage pathway of the frontal sinuses, maxillary sinuses, and anterior ethmoid air cells.
Drainage from the maxillary sinuses is directed superomedially toward the maxillary infundibulum, located lateral to the uncinate process and inferomedial to the orbit, through the hiatus semilunaris and posteromedially through the middle meatus to the back of the nasal cavity and into the nasopharynx. There is a strong correlation between opacification of the osteomeatal complex and the presence or development of sinusitis, with inflammatory changes of the maxillary sinuses seen in approximately 80% of patients with infundibular opacification and in 82% of patients with middle meatus opacification.
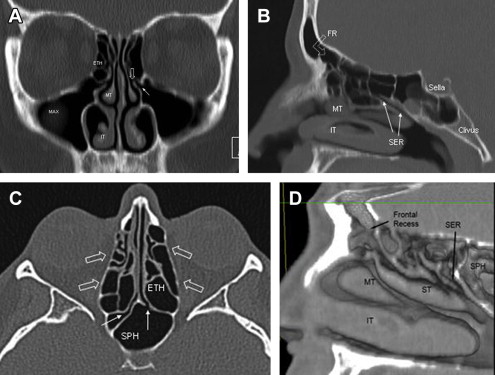
The frontal sinuses and anterior ethmoid air cells drain inferomedially via the frontal recess (or frontoethmoidal recess) down to the middle meatus. The posterior ethmoid air cells are located behind the basal lamella or lateral attachment of the middle nasal turbinate to the lamina papyracea of the orbit. Drainage from the posterior ethmoid air cells and sphenoid sinuses is via the sphenoethmoidal recess down into the nasopharynx. These key structures and the major anatomic outflow tracts are illustrated in Fig. 1 .
When imaging the paranasal sinuses, computed tomography (CT) without intravenous contrast is the imaging modality of choice. CT provides optimal delineation of osseous anatomy and, using multidetector helical CT acquisition techniques, can acquire thin, high-resolution axial scans with 0.75-mm collimation and 1-mm slice thickness with sagittal, coronal, or oblique reconstructions in less than a minute. These shorter scan times help limit motion artifact, reduce radiation exposure, and make CT more tolerable for patients who have difficulty lying prone or supine. Given the substantially different density of the aerated sinus, dense osseous margins of the paranasal sinus chambers and lower-density fat-containing tissues of the adjacent orbits, iodinated intravenous contrast is generally not necessary for most routine examinations. However, in cases of suspected early subperiosteal abscess or orbital involvement, contrast-enhanced images can better define small, peripherally enhancing abscess collections or extent of orbital involvement. Renal dysfunction is a relative contraindication to administering intravenous contrast, and should be avoided if the glomerular filtration rate (GFR) is less than 30.
Although magnetic resonance imaging (MRI) is limited with regard to bony detail, for those patients in whom neoplasm is suspected, or when there is need to further define the extent of orbital or intracranial involvement, MRI provides superior definition of the mucosa, adjacent soft tissues, and brain parenchyma. Particularly when osseous dehiscence is identified along the frontal, sphenoid, or ethmoid paranasal sinuses in a patient with altered mental status and sinusitis, MRI is essential to evaluate for findings of secondary subdural empyema or intracranial abscess, which may not be as apparent on CT alone. Sinonasal secretions and areas of mucosal thickening will demonstrate varied signal characteristics on MRI depending on protein content, thereby providing additional insight into chronicity of inflammation (see later discussion). Major limitations of MRI are increased cost and longer scan times, which can prove difficult for patients who are in discomfort and unable to keep still. Certain patients with non–MRI-compatible implanted devices are also unable to safely undergo MRI.
Anatomic variants that may predispose to rhinogenic headache
Any anatomic variant that obstructs 1 or more of the 3 major sinus outflow tracts can potentially predispose to obstructive sinus inflammation. The most common of these are discussed here. As CT now frequently serves as a roadmap for surgeons before functional endoscopic surgery, identification of certain specific anatomic variants, such as localized osseous dehiscence along the osseous margins of the posterior ethmoid or sphenoid sinuses underlying the optic nerves, nasofrontal, nasoethmoidal, and nasoorbital encephaloceles, is of utmost importance preoperatively to prevent potentially devastating intraoperative complications such as inadvertent orbital or intracranial entry.
Septal Variants
The nasal septum is the midline structure separating the right and left superior, middle, and inferior nasal turbinates. Bowing or deviation of the nasal septum is very common, often with bony spurring at the apex of deviation, which may compromise the OMC outflow tracts. In rare cases a portion of the nasal septum can be aerated, termed septum bullosa.
Concha Bullosa
When one or both of the nasal turbinates is aerated, this is termed a concha bullosa ( Fig. 2 ). Concha bullosa most commonly occur within the middle nasal turbinates, seen in approximately 34% to 53% of patients, with significant pneumatization of the inferior or superior nasal turbinates seen in fewer than 10%. When large enough, concha bullosa may obstruct the middle meatus, maxillary infundibulum, or any number of sinus outflow pathways. The mucous membrane lining the concha bullosa is no different from the rest of the sinuses and may also display inflammatory changes, including development of fluid-fluid levels.
Uncinate Variants
The free edge of the uncinate process has a variable course. Lateral deviation narrows the infundibulum. Medial deviation may narrow or obstruct the middle meatus. Occasionally, the free edge of the uncinate is fused to the orbital floor or lamina papyracea, described as an atelectatic uncinate process. Inflammation or hypoplasia of the ipsilateral maxillary sinus may be present, related to partial or complete obstruction of the infundibulum. Occasionally the uncinate may be aerated.
Ethmoid Variants
Ethmoid air cells extending along the inferior margin of the orbit are termed Haller cells ( Fig. 3 ), which are seen in 10% to 45% of patients. When large enough, Haller cells can cause narrowing or obstruction of the infundibulum. The anteriormost ethmoid air cells are termed agger nasi cells, which are immediately anterior and inferior to the frontal recess, and can thus narrow or potentially obstruct drainage from the frontal sinuses if large enough. Agger nasi cells are also in close proximity to the nasolacrimal ducts as they course inferiorly from the medial canthus, and can be a source of epiphora when inflammatory changes are present. Onodi cells are rare, posteriormost ethmoid air cells overlying the sphenoid sinuses, which are important to note given their close proximity to the optic nerves.
Rhinogenic Headache in the Absence of Sinusitis
In 1948, Wolff demonstrated that traction on different regions of the meninges and stimulation of various areas in the sinuses produced facial pain and headache. Over the past several decades, numerous studies have documented overall subjective improvement of headaches and facial pain following surgery directed at various contact points between 2 opposing mucosal surfaces within the nasal cavities, most commonly occurring between an osseous spur along a deviated nasal septum and the adjacent middle or nasal turbinate, or between a large concha bullosa and the uncinate process or lateral nasal wall. Certain patients with refractory headaches who have failed medical treatment directed at migraine and have no signs of underlying sinonasal inflammatory change, but demonstrate contact points on CT or endoscopy, may thus benefit from directed nasal surgery. Although mucosal contact points may be present in normal, asymptomatic patients who are scanned for other reasons, these anatomic variants can be another potential cause for rhinogenic headache, and are thus important to identify ( Fig. 4 ).
Infectious or inflammatory
Findings of Acute Versus Chronic Sinusitis
CT findings do not always correlate with severity of suspected rhinogenic or sinus-related symptoms, with incidental mucosal thickening noted on the CT scans of asymptomatic patients in as many as 5% to 40% of cases. Furthermore, the location of mucosal thickening within the paranasal sinuses may be more important than the extent. In other words, a subtle area of opacification within the infundibulum, sphenoethmoidal, or frontal recess may cause more discomfort for the patient than near complete opacification of the maxillary sinus with a mucous retention cyst or polyp. Nonetheless, CT imaging without intravenous contrast can establish the presence of inflammation in the paranasal sinuses, and thereby provides an objective means of monitoring the extent of disease.
The mucosal surface of the normal paranasal sinus approximates the bone so closely that it is not visualized on CT, thus any soft-tissue attenuation seen along the mucoperiosteal surfaces of the paranasal sinuses is abnormal. The presence of air-fluid levels has traditionally been associated with acute sinusitis, although the mere presence of fluid within the sinuses does not prove infection. Fluid from diagnostic or therapeutic lavage may remain for up to 2 weeks, and changes following a bout of acute sinusitis, even with successful therapy, may be seen for up to 6 to 8 weeks. In addition, acute sinusitis may be superimposed on chronic changes. Circumferential mucosal thickening without air-fluid level is nonspecific and can be seen in both the acute and chronic settings.
Classic findings of chronic sinusitis include polyposis, bony remodeling and thickening, and sclerosis related to osteitis from adjacent chronic mucosal inflammation ( Fig. 5 ). As sinonasal secretions become chronically entrapped and the mucosa resorbs free water, the initially thin serous secretions transition to a thicker mucus with higher protein content, eventually forming a desiccated plug. Thinner secretions with higher water content will be hypodense on CT, whereas more viscous secretions with higher protein content will have gradually higher densities. This transition is even more strikingly apparent on MRI, where initially serous secretions with high water content will be T1-hypointense and T2-hyperintense; then, as protein concentration increases within the trapped, inspissated secretions, the T1 signal will increase while the T2 signal decreases ( Figs. 6 and 7 ). As free water content further diminishes, the desiccated mucous plug will ultimately appear hypointense on both T1-weighted and T2-weighted images, nearly mimicking the normal aerated sinus.



