Purpose
To analyze the vitreomacular interface in idiopathic full-thickness macular holes (MHs) using spectral-domain optical coherence tomography.
Design
Prospective cross-sectional case series.
Methods
Ninety-one eyes of 86 consecutive patients with a MH were examined by spectral-domain optical coherence tomography. The vitreomacular interface was assessed and the presence or absence of an operculum was analyzed.
Results
Fifty-two eyes had a stage 2 MH, 12 eyes a stage 3 MH, and 27 eyes a stage 4 MH. No posterior hyaloid membrane was detected in any eyes with a stage 4 MH. In 35 (54.7%) of the 64 eyes with an MH without a complete posterior vitreous detachment (PVD), we saw a perifoveal PVD with vitreofoveal adhesion and partial dehiscence of the raised inner retina with an outer retinal separation in the MHs. In 24 (37.5%) of the 64 eyes without a complete PVD, an operculum, which is a hyperreflective structure of the foveal retina, was in front of the MH. The posterior hyaloid membrane was separated completely but adhered to the optic disc. In 2 (3.1%) of the 64 eyes without a complete PVD, the posterior hyaloid membrane was separated from the macula without an operculum. In 3 (4.7%) of the 64 eyes without a complete PVD, vitreofoveal adhesion on both edges of the hole was connected to the taut posterior hyaloid membrane without an operculum.
Conclusions
The vitreomacular interface had 4 configurations in MHs without a complete PVD. Approximately 55% of cases with an open roof in the eyes without a complete PVD may be at risk for progression to operculum formation (loss of retinal tissue).
Although several hypotheses regarding the pathogenesis of idiopathic full-thickness macular hole (MH) formation have been suggested, the vitreous condition has been implicated in the initiation and progression of MHs. Two primary hypotheses have been forwarded regarding the association of vitreomacular traction with development of MHs; anteroposterior traction of the vitreous fibers from the vitreous base traditionally was thought to cause macular breaks. However, Gass as well as Johnson and Gass hypothesized that spontaneous tangential traction exerted by the prefoveolar cortical vitreous caused idiopathic MHs.
In the latter half of the 1990s, optical coherence tomography (OCT) became a useful biomedical vitreomacular imaging tool. Time-domain (TD) OCT has provided substantial clinicopathologic information about the vitreomacular interface in eyes with an MH. Many studies have used TD OCT and ultrasonography to show localized separation of the perifoveal posterior hyaloid membrane from the retina, but with persistent vitreous adherence to the fovea. This condition has been termed a perifoveal posterior vitreous detachment (PVD) and has been found in eyes with MHs and in fellow eyes. Therefore, idiopathic age-related MH formation has been attributed to a perifoveal PVD with vitreofoveal adhesion. Thus, the theory of tangential vitreous traction was replaced by the currently accepted hypothesis that idiopathic MHs arise from anteroposterior vitreofoveal traction because of a perifoveal PVD. However, the entire vitreomacular interface in eyes with a full-thickness MH is still not elucidated completely, and the incidence of full-thickness MH formation is unknown in eyes with an idiopathic MH resulting from tangential vitreous traction or anteroposterior vitreofoveal traction.
The recently developed high-resolution spectral-domain (SD) OCT devices have allowed detailed in vivo visualization of posterior intraretinal structures and the vitreomacular interface that approaches the histologic level and have identified pathologic changes in the vitreofoveal architecture in idiopathic MH formation with greater detail. In the current pilot study, we analyzed the morphologic features of the vitreomacular interface in idiopathic full-thickness MH using images obtained prospectively by SD OCT and evaluated the incidence of full-thickness MH development in eyes with an idiopathic MH resulting from tangential vitreous traction or anteroposterior vitreofoveal traction, particularly regarding the location of the posterior hyaloid membrane and an operculum.
Methods
We prospectively evaluated the SD OCT images from 91 consecutive eyes (86 patients; 39 men, 47 women; mean age, 67.1 years; range, 47 to 89 years) with an idiopathic full-thickness MH in this cross-sectional study performed from December 12, 2008, through January 28, 2011, at the Asahikawa Medical University Hospital. All patients underwent routine ophthalmic examinations, including measurement of the best-corrected visual acuity, slit-lamp biomicroscopy with a superfield noncontact lens, color fundus photography, and SD OCT examination.
High-resolution SD OCT examinations were performed with the Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany). The details of this technique have been reported previously. Briefly, Spectralis OCT with 7-μm axial resolution reduces speckle noise using a 3-dimensional eye-tracking system with precise multiple B-scan averaging. Multiple B-scan frames of the same location were obtained, and the images were averaged. The automatic real-time function was turned on, and 30 frames were acquired for each B-scan location to reduce noise and to improve image quality. To assess the faint reflectivity of the posterior hyaloid membrane and the foveal morphologic features, all scans were acquired in the high-resolution acquisition mode through dilated pupils. SD OCT images were obtained bilaterally for each patient, that is, numerous vertical and horizontal macular linear scans (scan length, 15, 20, and 30 degrees) and 12 radial scans centered on the MHs in each eye.
Vitreoretinal specialists diagnosed idiopathic full-thickness MHs based on the clinical features. Each full-thickness MH was classified according to the clinical criteria described by Gass. Briefly, a stage 2 MH was diagnosed in eyes with an eccentric oval, crescent, or horseshoe retinal defect or a central round retinal defect at the fovea. Stage 3 MHs corresponded to a central round defect exceeding 400 μm without a complete PVD. After separation of the vitreous from the macular surface and optic disc and biomicroscopic observation of a complete PVD with a complete or partial ring of glial tissue (Weiss ring) in front of the optic disc, an MH with a complete PVD was diagnosed as a stage 4 MH, regardless of diameter. Based on the updated Gass classification, we identified the following MH stages: stage 2, 52 eyes; stage 3, 12 eyes; and stage 4, 27 eyes.
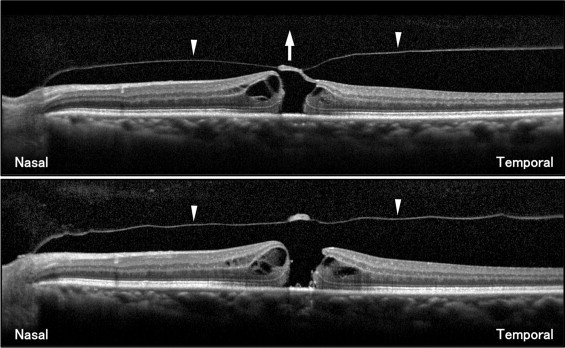
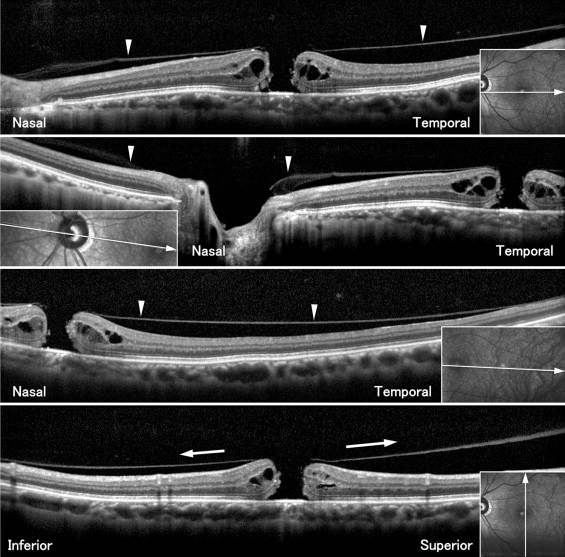
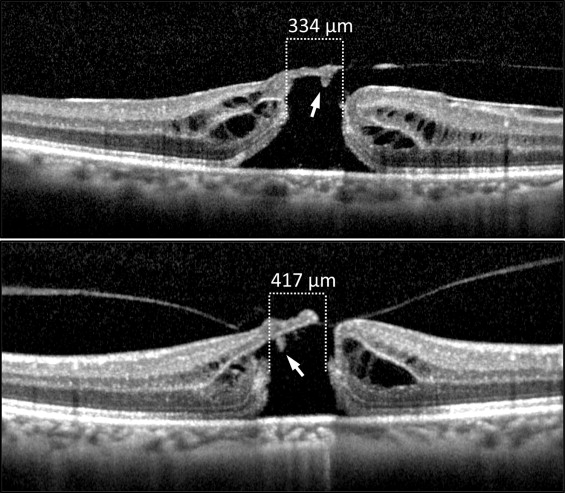
The term perifoveal PVD , which indicates a partially detached posterior hyaloid membrane with vitreofoveal adhesion, was defined as the reflectivity seen as a continuous thin line, that is, a precipitous posterior dip of the hyaloid face, attached to the fovea in a smooth biconvex curve on OCT. The MHs attributed to the anteroposterior vitreofoveal traction of a perifoveal PVD were defined as those with a concurrent operculum incompletely detached from the edge of the MH to which it seemed to belong like an open roof or flap with a perifoveal PVD, as seen in the SD OCT images ( Figure 1 ). We also used the definition that the MHs attributed to the anteroposterior vitreofoveal traction of a perifoveal PVD were those with a concomitant operculum in front of the MHs. A detached posterior hyaloid membrane with vitreopapillary adhesion, seen as a vitreomacular detachment, was observed in the SD OCT images. The operculum was in the posterior vitreous in the plane of the posterior hyaloid membrane ( Figure 1 ). These morphologic changes are thought to result from anteroposterior vitreofoveal traction associated with a perifoveal PVD. The MH that presumably was caused by the tangential vitreous traction of a posterior hyaloid membrane was defined as foveal dehiscence with vitreofoveal adhesion to both sides of the edges of a central, round, full-thickness MH in the SD OCT vertical and horizontal scans ( Figure 2 ). The vitreofoveal adhesions on the surface of both edges of the MH were connected to a taut posterior hyaloid membrane slightly detached from the macula. A histopathologic study reported similar morphologic features. High-speed OCT clearly showed a cone-shaped structure beneath the inner roof of the foveal pseudocyst with outer retinal separation in eyes with a stage 1B MH. We previously reported that the cone-shaped structure seemed to result from traction pulling away from the outer retinal layers seen on sequential SD OCT images. SD OCT also showed that the roof opened partially with a tiny cone-shaped structure under the roof. Therefore, the term cone-shaped structure under the open roof was defined as that observed in full-thickness stage 2 MHs seen in SD OCT images ( Figure 3 ).
The diameters of the MHs were measured manually on each scan using software calipers in the SD OCT image. The B-scan images were extracted from the radial lines scanned through the center of the MHs. Gass defined a stage 3 MH as centrifugal retraction of the foveolar retinal receptors that continues until the MH is fully formed and its diameter in all but a few cases reaches 400 μm. Therefore, the diameter was defined as the minimal distance measured at the level of the photoreceptor inner and outer segment (IS/OS) junction in the outer retinal layers from one margin to the other. We retained the MH with the smallest diameter in the SD OCT scans to avoid overestimating the size of the MHs. Spectralis OCT imaging facilitates effective measurements of MH diameters using a 3-dimensional eye-tracking system, because ocular motions affect the measurements and result in overestimation of the MH size. This evaluation of the MH diameter required numerous scans to ensure that the linear scan was performed exactly across the center of the MH.
We carefully excluded posttraumatic MHs and those developing in vitrectomized eyes from the study. Other exclusion criteria included MHs associated with degenerative myopia exceeding −6.0 diopters; eyes with macular or retinal diseases such as aged-related macular degeneration, diabetic retinopathy, and retinal detachment; and poor-quality OCT scans because of severe cataract. Seven patients were pseudophakic at the time of the SD OCT examination.
The primary end point in the current study was the percentage of MHs attributed to anteroposterior vitreofoveal traction or tangential vitreous traction in idiopathic full-thickness MHs, as seen on images obtained prospectively by high-resolution SD OCT. Therefore, we analyzed the initial morphologic features of the vitreomacular interface assessed by reflectivity of the continuous linear signal of the posterior hyaloid membrane, the presence or absence of an operculum in front of the MH, and the location of an operculum. We also analyzed the morphologic features of the foveal structures of the MHs, especially the presence or absence of cone-shaped structures under the open roof.
Results
In all eyes with stage 2 and 3 MHs, we observed a partially detached posterior hyaloid membrane with persistent attachment to the optic disc margin on the SD OCT scans as reflectivity of the continuous linear signal in the posterior vitreous. We did not detect the posterior hyaloid membrane and opercula in any eyes with a stage 4 MH.
In 35 (54.7%) of the 64 eyes with an MH without a complete PVD (age range, 51 to 79 years; mean ± standard deviation, 67.3 ± 7.3 years), 35 (67.3%) of the 52 eyes with a stage 2 MH, and none (0%) of the 12 eyes with a stage 3 MH, we saw a perifoveal PVD with vitreofoveal adhesion and partial dehiscence of the raised inner retina with an outer retinal separation in the MHs ( Table 1 ). The raised inner retina was attached to the edge of the MH and appeared as an open roof or flap with the posterior hyaloid membrane remaining attached. The open roof, which is seen as the presumed incompletely detached operculum, seemed to belong to the inner retina, because it had the same reflectivity and formed a continuous structure with the inner retina. We saw a cone-shaped structure under the open roof of a stage 2 MH less than 400 μm in diameter in 7 (25%) of 28 eyes at the level of the IS/OS junction in the outer retinal layers and in 1 (14.3%) of 7 eyes with a stage 2 MH with an open roof exceeding 400 μm at the level of the IS/OS junction.
| Stage | Eyes | Mean IS/OS Separation (Range), μm | A a | B b | C c | D d |
|---|---|---|---|---|---|---|
| 2 | 52 | 254 (82 to 564) | 35 of 52 (67.3%) | 14 of 52 (26.9%) | 1 of 52 (2%) | 2 of 52 (4%) |
| 3 | 12 | 517 (405 to 766) | 0 of 12 (0%) | 10 of 12 (83.3%) | 1 of 12 (8%) | 1 of 12 (8%) |
| 4 | 27 | 419 (90 to 1008) | — | — | — | — |
a Full-thickness hole with concurrent operculum remains incompletely detached from the hole edge as a open roof or flap with a perifoveal posterior vitreous detachment.
b Full-thickness hole with a concomitant operculum in front of the hole with a plane of a posterior hyaloid membrane with a vitreopapillary adhesion.
c Full-thickness hole without a concomitant operculum in front of the holes with the plane of a posterior hyaloid membrane with a vitreopapillary adhesion.
d Full-thickness holes with vitreofoveal adhesion to both sides of the hole edges in the vertical and horizontal scans without an operculum.
We observed an operculum in front of the central round MHs ( Table 1 ) in 24 (37.5%) of the 64 eyes with an MH without a complete PVD (age range, 47 to 77 years; mean ± standard deviation, 67.3 ± 6.7 years), 14 (26.9%) of 52 eyes with a stage 2 MH, and 10 (83.3%) of 12 eyes with a stage 3 MH. The posterior hyaloid membrane was separated completely from the posterior retina, except at the optic disc margin. The operculum was in the vitreous at the plane of the posterior hyaloid membrane and seemed to be detached completely from the retina and belonged to the inner retina, because it had the same reflectivity in the SD OCT images, which were sufficiently clear to observe the relationship between the operculum and the foveal retina. Therefore, the MHs in 59 (92.2%) of the 64 eyes without a complete PVD could be attributed to the anteroposterior vitreofoveal traction of a perifoveal PVD.
In 2 (3.1%) of the 64 eyes with an MH without a complete PVD (1 [2%] of 52 eyes with a stage 2 MH and 1 [8%] of 12 eyes with a stage 3 MH; age range 50 and 78 years; mean ± standard deviation, 64 ± 18.9 years), the plane of the posterior hyaloid membrane was in the vitreous with vitreopapillary adhesion and appeared as a vitreomacular detachment in the eyes. However, we did not see an operculum on the SD OCT images ( Table 1 ).
In 3 (4.7%) of the 64 eyes with an MH without a complete PVD (2 [4%] of 52 eyes with a stage 2 MH and 1 [8%] of 12 eyes with stage 3 MHs; age range, 56 to 67 years; mean ± standard deviation, 60.3 ± 5.9 years), we saw vitreofoveal adhesion on both sides of the edges of the MHs in the vertical and horizontal scans ( Table 1 ). Eccentric dehiscence of the inner retina and the open roof attached to the edges of the MHs were not seen. Vitreofoveal adhesion was seen on the surface of both edges of the MHs; these were connected to a taut posterior hyaloid membrane slightly detached from the macula. We did not observe a vitreofoveal separation in any case, that is, a local separation of the hyaloid face from the edge of the MH with persistent vitreomacular adherence around the MH. In these 3 eyes, the MHs presumably formed because of tangential vitreous traction. There was no significant difference in ages among the 4 groups ( P = .48, 1-way analysis of variance).
Results
In all eyes with stage 2 and 3 MHs, we observed a partially detached posterior hyaloid membrane with persistent attachment to the optic disc margin on the SD OCT scans as reflectivity of the continuous linear signal in the posterior vitreous. We did not detect the posterior hyaloid membrane and opercula in any eyes with a stage 4 MH.
In 35 (54.7%) of the 64 eyes with an MH without a complete PVD (age range, 51 to 79 years; mean ± standard deviation, 67.3 ± 7.3 years), 35 (67.3%) of the 52 eyes with a stage 2 MH, and none (0%) of the 12 eyes with a stage 3 MH, we saw a perifoveal PVD with vitreofoveal adhesion and partial dehiscence of the raised inner retina with an outer retinal separation in the MHs ( Table 1 ). The raised inner retina was attached to the edge of the MH and appeared as an open roof or flap with the posterior hyaloid membrane remaining attached. The open roof, which is seen as the presumed incompletely detached operculum, seemed to belong to the inner retina, because it had the same reflectivity and formed a continuous structure with the inner retina. We saw a cone-shaped structure under the open roof of a stage 2 MH less than 400 μm in diameter in 7 (25%) of 28 eyes at the level of the IS/OS junction in the outer retinal layers and in 1 (14.3%) of 7 eyes with a stage 2 MH with an open roof exceeding 400 μm at the level of the IS/OS junction.
| Stage | Eyes | Mean IS/OS Separation (Range), μm | A a | B b | C c | D d |
|---|---|---|---|---|---|---|
| 2 | 52 | 254 (82 to 564) | 35 of 52 (67.3%) | 14 of 52 (26.9%) | 1 of 52 (2%) | 2 of 52 (4%) |
| 3 | 12 | 517 (405 to 766) | 0 of 12 (0%) | 10 of 12 (83.3%) | 1 of 12 (8%) | 1 of 12 (8%) |
| 4 | 27 | 419 (90 to 1008) | — | — | — | — |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


