Obstructive sleep apnea (OSA) is the result of upper airway obstruction during sleep. Hypopharyngeal airway obstruction can be caused by the prominence or relaxation of the base of the tongue, lateral pharyngeal wall, and occasionally, the aryepiglottic folds or epiglottis. Although nasal continuous positive airway pressure (CPAP) is considered as the first treatment for obstructive sleep apnea, surgery has been shown to be a viable option for patients who are intolerant of positive pressure therapy. This article presents the current state of hypopharyngeal surgery for sleep apnea. Preoperative airway evaluation with fiberoptic nasopharyngoscopy, the use of lateral cephalometric radiograph, and the formulation of a surgical plan with selection of procedures to address hypopharyngeal obstruction are discussed.
Obstructive sleep apnea (OSA) is the result of upper airway obstruction during sleep. Hypopharyngeal airway obstruction can be caused by the prominence or relaxation of the base of the tongue, lateral pharyngeal wall, and occasionally, the aryepiglottic folds or epiglottis . Compromised maxillofacial anatomy in the form of a narrowed maxillomandibular arch or maxillomandibular deficiency can also be a significant factor leading to hypopharyngeal obstruction . The complex interplay of the soft and hard tissues that contribute to hypopharyngeal obstruction, the importance of the hypopharynx to speech and swallowing, and the subsequent edematous response after surgical intervention present formidable challenges to the surgeon. This article presents the current state of hypopharyngeal sleep apnea surgery. Preoperative airway evaluation with fiberoptic nasopharyngoscopy and lateral cephalometric radiograph, and the formulation of a surgical plan with selection of procedures to address hypopharyngeal obstruction are discussed.
Preoperative assessment
It is well-accepted that successful surgical outcome depends on proper patient selection as well as the choice of surgical procedure. Therefore, a logical and systematic approach to clinical evaluation, treatment planning, surgical execution, and perioperative management is necessary to maximize safety and improve outcomes. Surgical success can be defined by
Quality of life improvement with reduction of OSA symptoms
Achieving respiratory disturbance index (RDI) of less than 20, and reduction of RDI greater than 50%
Improvement of oxygen nadir to 90%, with few desaturations to below 90%
Clinical evaluation must include the overall body habitus (height, weight, and neck circumference), because it has been shown that the surgical outcomes can be influenced by these factors . Obviously, a detailed examination should be focused in the head and neck region to identify the potential sites of upper airway obstruction, including the nose, soft palate, lateral pharyngeal walls, and tongue base. The clinical examination of the hypopharyngeal airway includes assessment of the tongue size and position . Additionally, examination of the size and position of the maxilla and mandible must also be included, because narrowed or deficient maxilla and mandible are common findings in patients who have OSA. By using fiberoptic nasopharyngoscopy and lateral cephalometry, along with direct visual examination, the hypopharyngeal airway can be completely assessed for anatomic abnormalities that may be contributing to OSA.
Fiberoptic nasopharyngolaryngoscopy
Airway examination by a fiberoptic scope is highly recommended in patients who have OSA. This evaluation enables the examiner to directly visualize the entire upper airway, from the nose to the larynx. The dimension of the nasal, velopharyngeal, and hypopharyngeal airway can be fully assessed. Furthermore, the prominence of the tongue base and the lateral pharyngeal wall, as well as their collapsibility, can be evaluated with Mueller’s maneuver ( Fig. 1 ) .

Lateral cephalometric radiograph
Many airway imaging methods are currently available. CT or MRI can precisely assess the dimension of the upper airway ; however, because of cost constraints, none can be widely used in clinical practice except the lateral cephalometric radiograph. Although the lateral cephalometric radiograph is only a static two-dimensional method of evaluating a dynamic three-dimensional area, it is a valuable study to identify abnormal facial skeletal anatomy that may contribute to airway obstruction, as well as the relation of the hard and soft tissues of the airway ( Fig. 2 ). Furthermore, the lateral cephalometric radiograph provides useful information on the posterior airway space behind the soft palate and the tongue base. The posterior airway space measurement on lateral cephalometric radiograph has been shown to correlate with the volume of hypopharyngeal airway on three-dimensional CT scans .

Surgical procedures
Genioglossus advancement
The mandible and the tongue are major determinants of the airway dimension. Anterior positioning of these structures has been shown to improve OSA. The genioglossus advancement (GA) procedure is limited to moving the geniotubercle with the genioglussus insertion forward without moving the mandible ( Fig. 3 ). This advancement places tension on the tongue musculature, and thus limits the posterior displacement during sleep. The GA procedure consists of a rectangular osteotomy on the symphysis of the mandible intraorally. The rectangular segment is advanced the thickness of the mandible, and partially rotated to prevent retraction back into the floor of the mouth. Incorporation of the geniotubercle during the procedure has been shown to be quite successful with this technique . In general, GA is performed with other sleep apnea surgical procedures such as uvulopalatopharyngoplasty (UPPP) and hyoid advancement to maximize the improvement. The success rates of the procedures have been variable, ranging from 23% to 77% . The variable results underline the difficulty in accurately predict success rate. Clearly, anatomic factors, body habitus ,and OSA severity are all factors that influence the surgical success. In general, the potential risks associated with GA are quite limited, but include infection, hematoma, injury to the genioglussus muscle, and paresthesia of the lower teeth.
Hyoid advancement
The hyoid bone is in intimate relationship with the tongue base and pharyngeal musculatures, and thus is an integral aspect of the upper airway anatomy. The hyoid bone may be surgically repositioned anteriorly, by attaching it to the thyroid cartilage to expand the airway ( Fig. 4 ) . Hyoid advancement (HA) is usually performed in conjunction with GA to improve OSA ; however, some surgeons elect to combine it with UPPP alone . An inherent problem with HA is the requirement for an external incision on the neck, which may not be readily accepted by all patients. As with other sleep apnea surgical procedures, the success rates of hyoid advancement can be variable, ranging from 17% to 65% . In general, the associated surgical risks are low, but include infection, seroma formation, and dysphagia.
Maxillomandibular advancement
Maxillomandibular deficiency results in diminished airway dimension, which leads to nocturnal obstruction. Maxillomandibular advancement (MMA) expands the skeletal framework that encircles the airway, thus enlarging the entire airway, including the nasal, pharyngeal, and hypopharyngeal airway. Comparisons of pre- and postoperative airway appearance based on lateral cephalometric radiograph and fiberoptic nasopharyngoscopy have demonstrated that in addition to airway expansion by the forward movement of the maxillomandibular complex, the tension and collapsibility of the suprahyoid and velopharyngeal musculature may also be reduced, thus leading to the reduction of lateral pharyngeal wall collapse .
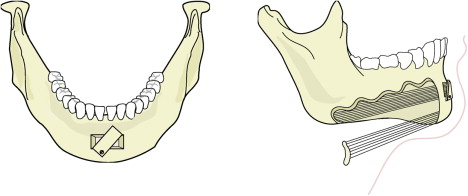
The procedure consists of mobilizing the maxilla and mandible to achieve anterior displacement of the maxillomandibular complex, after intraoral osteotomy of the maxilla and mandible ( Fig. 5 ). The maxilla and mandible are stabilized with titanium plates in the advanced position. To maximize the airway expansion, an advancement of 10 to 14 mm is usually recommended; however, it is important to achieve maximal advancement while maintaining a stable dental occlusion and a balanced aesthetic appearance. Interestingly, although many patients may be left with “prominent jaws,” very few patients are dissatisfied with their appearance .
MMA is the most effective sleep apnea surgical procedure currently available. The success rate is usually between 75% to 100% , with a long-term success approaching 90% . In addition, patient perception of the surgical outcome has been very favorable . Although MMA is considered a fairly invasive procedure, the associated surgical risks are low, but include bleeding, infection, malocclusion, and partial numbness of the lower lip, chin and palate.
Tongue base suspension suture
The rationale of tongue base suspension suture is similar to GA, in that both procedures are aimed at reducing the collapsibility of the tongue during sleep. The suspension suture is looped from the anchor screw on the inner surface of the mandible to the base of the tongue. The suture is tightened down with some tension to create a hammock effect for the tongue. The procedure is simple to perform and can be completed within 20 minutes. The tongue base suspension suture is routinely performed with UPPP to maximize outcomes. The reported success rates have been variable, ranging from 20% to 82% . Associate risks of the procedure are low and are limited to infection, injury to tooth roots, and detachment of the anchor screw. As with GA and HA, the variable results underline the difficulty in accurately predicting success rate.
Temperature-controlled radiofrequency tongue reduction
The frictional heat generated by radiofrequency (RF) results in tissue injury, and leads to tissue volume reduction . The size of the lesion (area of tissue injury) created depends on the current intensity and the duration of energy delivery .
The first prospective study of RF tongue reduction demonstrated that after a mean of 8490 J delivered to the tongue in 18 patients, the mean RDI improved from 39.6 to 17.8, with an improved lowest saturation (LSAT) from 81.9% to 88.3% . There were no changes in speech or swallowing. Complications included a superficial tongue ulceration that resolved spontaneously, persistent pain on swallowing that resolved after several weeks, and a tongue abscess that required drainage. Long-term follow-up demonstrated that despite minimal weight gain (3.1 kg), there was a worsening of RDI from 17.8 to 28.7, with a worsening trend in the LSAT from 88.1% to 85.8%; however, there was no significant deterioration of the quality of life measurements by SF-36, or daytime sleepiness by the Epworth Sleepiness Scale (ESS) .
Multiple other reports have shown RF tongue reduction to be efficacious in improving OSA . Furthermore, comparison of RF airway treatment to CPAP demonstrated that patients treated with RF alone achieved higher results in outcomes metrics . Currently, RF airway treatment is often performed as an adjunctive procedure, along with other hypopharyngeal airway surgical procedures.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


