Sleep-disordered breathing is a growing public health concern and an integral part of head and neck surgery. Multichannel home sleep testing is a cost-effective, patient-friendly, scientifically valid technique of evaluating patients who present with symptoms of sleep-disordered breathing, typically snoring or daytime sleepiness. Home sleep tests can be dispensed from the physician’s office. They have a 95% successful recording rate. Scoring can be autoscore or manual score. There are several protocols that can be followed based on diagnostic outcomes.
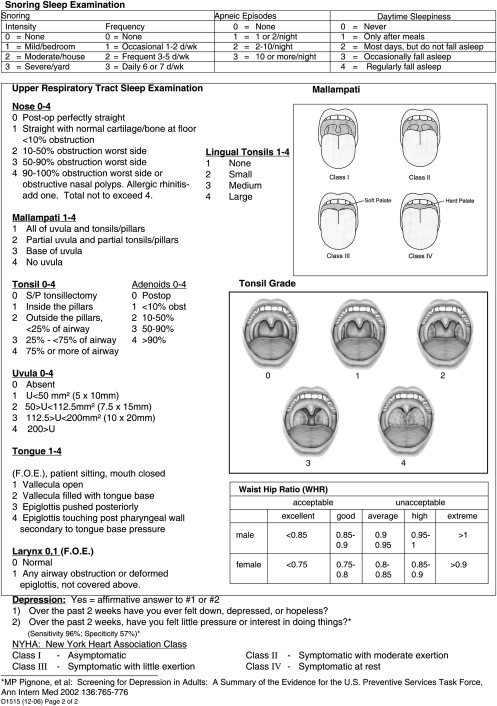
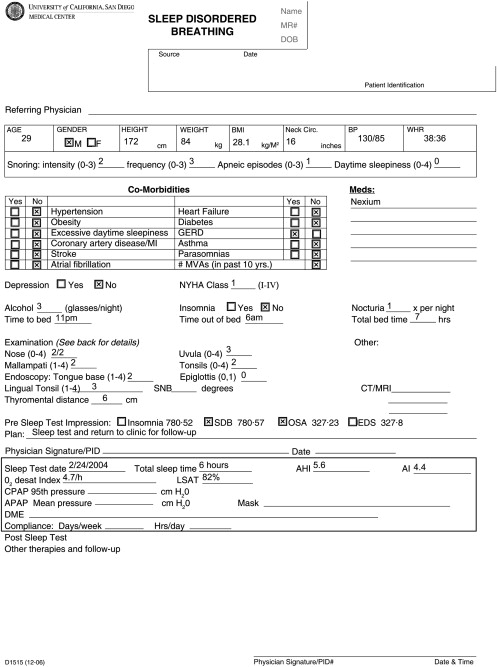
A 29-year-old male patient presents because his wife complains his snoring is keeping her awake at night. As with many patients who snore, he has been forced to leave the conjugal bed. In self-reporting his symptoms on the following scale: 1 = mild, 2 = moderate, and 3 = severe ( Fig. 1 ), the patient rates snoring as a 2, his apneic episodes with a 1, and daytime sleepiness with a 0. The patient denies other symptoms of sleep disordered breathing (SDB) and requests a surgical procedure to correct his snoring. The authors’ evaluation is shown in Fig. 2 . His body mass index (BMI) is 28, neck circumference is 16 in, waist circumference is 38 in, Mallampati is II, tonsil grade is 2, nose is 2/2, and uvula is 3. Fiberoptic endoscopy shows a tongue base score of 2, a lingual tonsil of 3, and an epiglottis of 0. A multichannel home sleep test was performed. The results are seen in Fig. 3 .
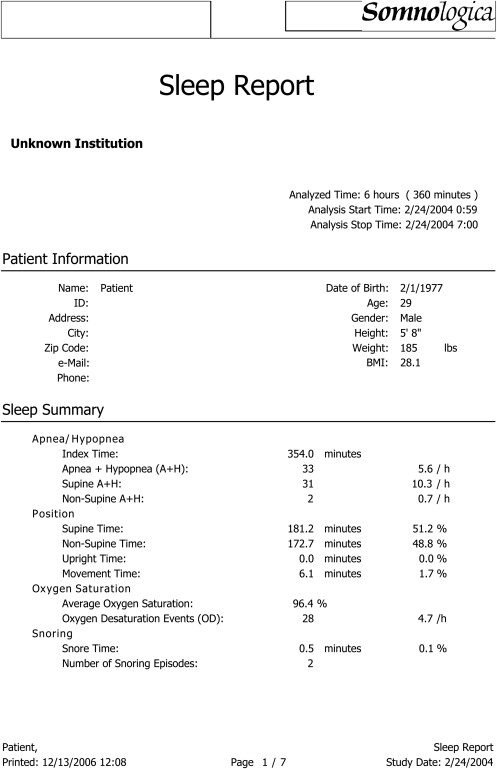
The patient was diagnosed with mild SDB; however, absent other symptoms and greater severity, the primary problem was snoring. The patient was recommended for a continuous positive airway pressure (CPAP) trial at his own expense, but he declined. He was then offered two different surgical options. The first was palatal implants; the second was septoplasty, uvulectomy, palatal implants, and coblation of his lingual tonsils. The patient opted to proceed with palatal implants and would only consider the more extensive surgery if this option failed. Surgery was performed in the office. Six weeks later, the patient reported that his snoring was dramatically reduced, and he had been invited back to his bed.
SDB includes primary snoring, obstructive sleep apnea, and several other diagnoses. A sleep test is an important tool in the evaluation of any patient who has SDB, be it mild, moderate, or severe. Although some believe they can separate snorers from sleep apneics, or mild from severe SDB by history and physical examination, objective evaluations have not supported this practice . Regardless, insurance companies require an objective measure of the severity of SDB before authorizing CPAP, surgery, or other treatments. Sleep testing originated with the electroencephalogram (EEG) and then added respiratory metrics, oximetry, leg movement sensors, chest and abdominal movement, and eye movement. Respiration has been the single most important measure and is the only measure necessary to objectively document disease severity . Respiration is typically measured with a nasal cannula and/or an oral thermistor measuring mouth breathing. The nasal cannulae are most accurate; they measure pressure and calculate nasal flow. Adult criteria define an apneic event as a 90% or greater decrease in respiratory flow for 10 or more seconds . Hypopneas are variably defined; some define a hypopnea as a 50% decrease in airflow for 10 or more seconds, whereas others require a 75% or greater decrease in airflow for 10 or more seconds . Some criteria even require an oxygen desaturation of 2%, 3%, or even 4% before grading it as a hypopnea . The apneas and hypopneas are typically summed and reported as events per hour. Children have a faster respiratory rate; therefore, the duration of an apnea or hypopnea is typically shortened and, depending on the age of the child, can be anywhere from 6 to 8 seconds . Time courses for adolescents have not been particularly looked at or evaluated but are presumably somewhat intermediate. For adults, an Apnea Hypopnea Index (AHI) of five or more events per hour is considered abnormal; however, most insurance companies do not cover treatment unless the AHI is 15 or more or if the AHI is 5 or more with at least two comorbidities. The most common comorbidities are cardiovascular disease, obesity, daytime sleepiness, and hypertension . Table 1 lists common SDB comorbidities and their prevalence. Premenopausal women may have significant SDB with much lower severity. Christian Guilleminualt from Stanford University’s Sleep Medicine Program describes a syndrome called the upper airway resistance syndrome, in which there is an increased resistance to airflow in the throat with a decrease in airflow measured at the nose, but not severe enough to be measured as a hypopnea . These can result in cortical arousal, disrupt sleep, and cause many or all symptoms of SDB. Women are more prone to upper airway resistance syndrome and significant, symptomatic SDB with lower AHIs.
| Category | Condition | References | |
|---|---|---|---|
| Cardiac | Hypertension | 30% | |
| Drug-resistant hypertension | 83% | ||
| Congestive heart failure | 76% | ||
| Ischemic heart disease | 38% | ||
| Dysrhythmias | 58% | ||
| Atrial fibrillation | 49% | ||
| Respiratory | Pulmonary hypertension | 77% | |
| Asthma | 18% | ||
| Neurologic | Stroke | 90% | |
| Metabolic | Type II Diabetes | 15% | |
| Metabolic syndrome | 50% | ||
| Morbid Obesity (Male) | 90% | ||
| Morbid Obesity (Female) | 50% | ||
| Gastrointestinal | Gastroesophageal reflux disease | 60% | |
| Genitourinary | Nocturia | 48% |
Oximeters are typically used for most home sleep tests. They are not the highly sensitive oximeters physicians use in the operating room and intensive care units. Nonetheless, the data derived are viewed as sacrosanct. An individual who desaturates throughout their sleep study is viewed as having more significant SDB. Some report the lowest oxygen saturation, commonly referred to as the lowest oxygen saturation. The authors are not convinced this is a useful tool. If the oximeter slips on the finger, the oxygen saturation can fall, and the lowest oxygen saturation can inaccurately be reported as low as 60% or 70%. Regardless, looking at the oxygen tracing is useful in assessing SDB. Hypoxemia, a drop in oxygen levels below 90%, is also associated with daytime sleepiness and cerebral dysfunction .
Chest and abdominal belts are often used to measure obstructive versus central events. The authors do not find this useful for the typical patient consulting a head and neck surgeon. Virtually everyone who snores, which is the premier symptom of SDB, has obstructive sleep apnea. The only people who have significant central SDB are those who have advanced heart failure or a history of stroke.
Often, central sleep apnea is described in individuals who have more common SDB. For some individuals, this may be an artifact. Upon sensing the obstructive event, the respiratory effort is stopped. Abdominal and thoracic effort stops. This would then be recorded as a central event when it actually was an obstructive event. Regardless, for an initial sleep test, the obstructive and central events are summed, and whether or not they are viewed as obstructive or central is irrelevant.
Home sleep tests are easy to administer. Patients typically come to the physician’s office; a trained technician reviews any questions the patient has about the nature of the test and why they are taking it. The patient is then shown how to apply the various recording devices to their body and how these are connected to the sleep machine. They are then shown how the recording is initiated when going to bed, how it is managed should one arise during the night, and how the recording is stopped upon arising in the morning. The machine is then returned to the physician’s office where the information is downloaded into a computer and the data are analyzed. For most machines, autoscore capability is available, and where autoscore matches the patient’s history and physical examination, it is sufficient. Where the autoscore is borderline and the patient’s history or examination are questionable, manual score capability is important and easily learned. Figs. 4 and 5 demonstrate the steps of administering, downloading, and evaluating a typical patient suspect for SDB. To better describe this process, several cases are presented.


Case one
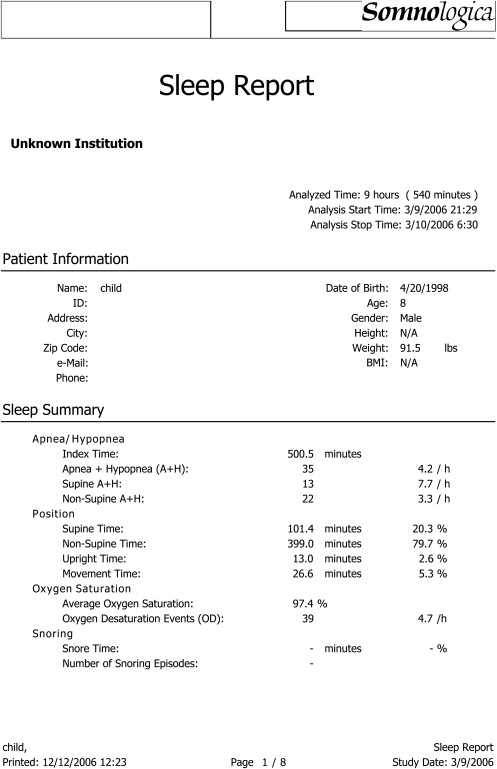
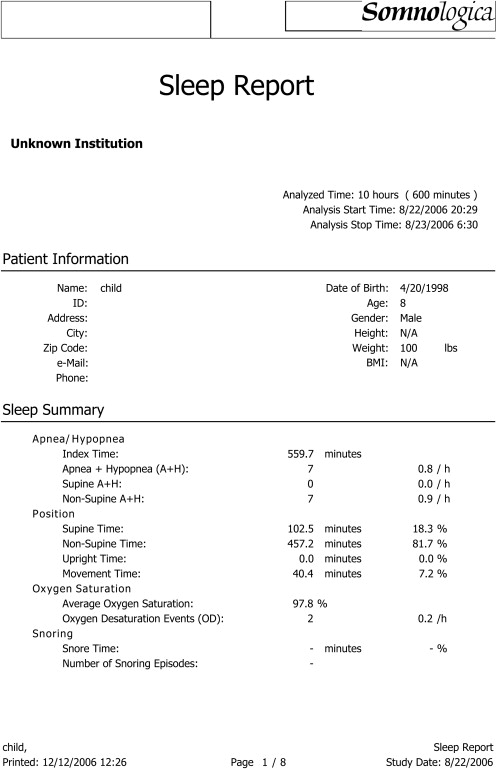
An 8-year-old boy is referred for surgical evaluation for snoring. Physical examination shows the child has normal height, weight, and BMI; tonsil grade is 3 plus. He is without allergic rhinitis and breathes through his nose at night. The child’s mother had previously sought surgical consultation for him. The physician had recommended that tonsillectomy be performed, but the parents, afraid of the risks and complications, had elected not to proceed. The patient now presents for a second opinion. Before rendering an opinion on history and examination alone, a multichannel home sleep test was administered. The child wearing the sleep unit is seen in Fig. 6 . While an ongoing study looking at the neuropsychologic consequences of sleep apnea in children was underway, the child enrolled into the research study whereby a neuropsychologic battery was also administered. Given the abnormalities seen in the neuropsychologic evaluation and an abnormal sleep test, namely an AHI of 4.2 events per hour, a recommendation for tonsillectomy was made, and the parents agreed. The procedure was uneventful, and the child made a normal recovery. Three months later, the sleep test and neuropsychologic evaluation were repeated. The results of the home sleep test and the neuropsychologic data before and after surgery are shown in Figs. 7 and 8 and Table 2 . In children, an abnormal AHI has not yet been determined. However, current opinion for prepubescent children is that an AHI of 1 or more is in fact abnormal. The authors’ experience has been that an AHI of 5 or more will most likely not only show improvement in snoring following tonsillectomy, but will also show improvement in behavioral and cognitive functioning.

| Test | Domain | Presurgery | Postsurgery |
|---|---|---|---|
| Statue | Attention/executive function | 29 | 27 |
| Visual attention | Attention/executive function | 34 | 37 |
| Knock–tap | Attention/executive function | 28 | 28 |
| Finger tapping PH | Sensorimotor function | 6 | 9 |
| Finger tapping NPH | Sensorimotor function | 9 | 11 |
| Sequential tapping PH | Sensorimotor function | 20 | 19 |
| Sequential tapping NPH | Sensorimotor function | 32 | 36 |
Assuming that 10% of children snore and 1% or 2% have sleep apnea, it seems that there is no documented benefit to operating on the 10%. The only documented benefit is operating on the 2%, a group that presumably has an AHI of 5 or more. The home sleep test seems to be an excellent tool for determining who may or may not benefit from surgical procedures in correcting SDB. The authors’ experience is that current home sleep tests are accurate in children no younger than 4 years of age. Less than age 4, children simply do not have enough respiratory volume to accurately drive the respiratory meters.
Case two
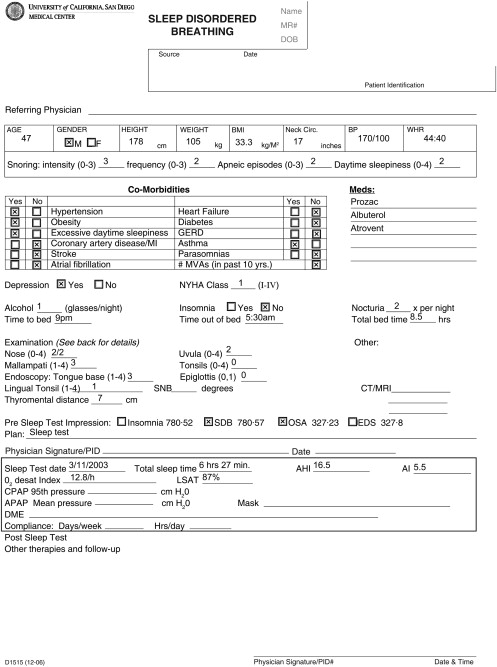
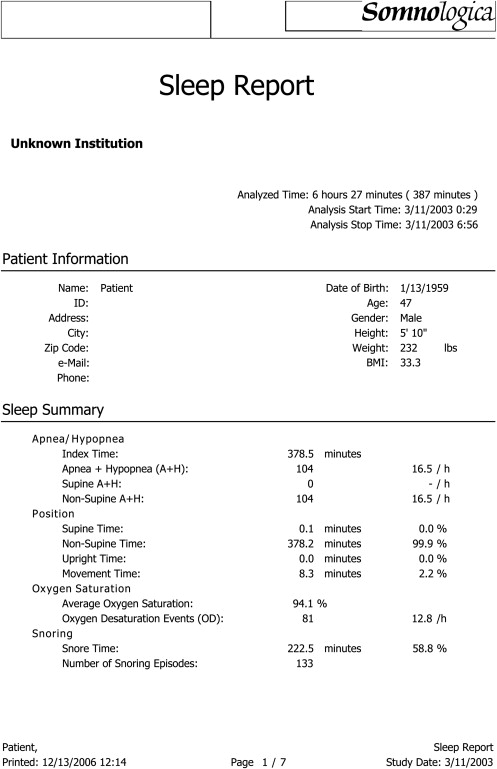
A 47-year-old male presents with a primary complaint of snoring. He had been snoring for most of his life, but with a recent 10-pound weight gain, the frequency and the loudness of his snoring had increased. His wife complained that, not only did he snore, but he occasionally stopped breathing at night. The patient was a hard-working executive. He had some daytime sleepiness, but believed that this was simply a function of age, work intensity, and lack of regular exercise and normal sleep. On a self-report of his symptoms based on the aforementioned scale in case one (see Fig. 1 ), he reported his snoring to be a 3, frequency of snoring to be 2, apneic episodes were 2, and daytime sleepiness was 2. History and physical examination are shown in Fig. 9 . His neck circumference is 17 in, nose is 2/2, Mallampati is 3, tonsil grade is 0, uvula is 2, and his comorbidities are obesity and hypertension. His endoscopic measurements indicated tongue is 3, lingual tonsils are 1, and epiglottis is 0. The patient underwent a multichannel home sleep test. The results are shown in Fig. 10 . The AHI is 16, which is abnormal. In this case, oxygen desaturations are seen, which is associated with deeper stages of sleep. One could argue that this is a milder case of sleep apnea. However, the patient has daytime sleepiness; elevated BMI; elevated AHI; oxygen desaturations; and on physical examination, this is a Friedman Stage III, based primarily on the Mallampati examination. This is sleep apnea. This individual is recommended for CPAP. Nasal surgery and palatal surgery would be unlikely to provide benefit. This individual should not be confused as a snorer but, instead, has sleep apnea, and, absent significant weight loss, he will continue to have sleep apnea and needs to be treated effectively with CPAP.
Case two
A 47-year-old male presents with a primary complaint of snoring. He had been snoring for most of his life, but with a recent 10-pound weight gain, the frequency and the loudness of his snoring had increased. His wife complained that, not only did he snore, but he occasionally stopped breathing at night. The patient was a hard-working executive. He had some daytime sleepiness, but believed that this was simply a function of age, work intensity, and lack of regular exercise and normal sleep. On a self-report of his symptoms based on the aforementioned scale in case one (see Fig. 1 ), he reported his snoring to be a 3, frequency of snoring to be 2, apneic episodes were 2, and daytime sleepiness was 2. History and physical examination are shown in Fig. 9 . His neck circumference is 17 in, nose is 2/2, Mallampati is 3, tonsil grade is 0, uvula is 2, and his comorbidities are obesity and hypertension. His endoscopic measurements indicated tongue is 3, lingual tonsils are 1, and epiglottis is 0. The patient underwent a multichannel home sleep test. The results are shown in Fig. 10 . The AHI is 16, which is abnormal. In this case, oxygen desaturations are seen, which is associated with deeper stages of sleep. One could argue that this is a milder case of sleep apnea. However, the patient has daytime sleepiness; elevated BMI; elevated AHI; oxygen desaturations; and on physical examination, this is a Friedman Stage III, based primarily on the Mallampati examination. This is sleep apnea. This individual is recommended for CPAP. Nasal surgery and palatal surgery would be unlikely to provide benefit. This individual should not be confused as a snorer but, instead, has sleep apnea, and, absent significant weight loss, he will continue to have sleep apnea and needs to be treated effectively with CPAP.



