The human voice is produced when a pressurized column of air is expired through the glottic space causing the vocal folds to vibrate. The laryngeal muscles adduct (close) the vocal folds, while the muscular and passive forces of exhalation increase subglottic pressure. Subglottic pressure eventually reaches a level sufficient to force the glottis to open. After the release of air, the subglottic pressure lowers, and as air travels between the folds, the pressure decreases in accordance with Bernoulli’s principle. The vocal folds then approximate to begin a new cycle.
Phonation is produced by vibration of the vocal folds. The regularity and periodicity of vibration of the vocal folds determines vocal quality. Pitch, measured in hertz, is determined by the frequency, or number of cycles of vibration of the vocal folds per second. Loudness, measured in decibels, is determined by the amplitude of each vibration. Pitch and loudness can be modified through the fine motor controls of the length and tension of the vocal folds and the pressure of the air stream. Modification of phonation by the oropharyngeal and nasal cavities is known as resonance. Articulation is controlled by the interface between the tongue and the palate, teeth, and lips. Hoarseness can result from a disorder that changes the surface characteristics of the vocal cords or the vibratory capabilities of the vocal folds.
The voice changes throughout the life cycle. Physical mutation during puberty involves development of the secondary sex characteristics, of which one of the most prominent and generally noticeable is differentiation of the adult voice into male and female types. At puberty the larynx grows rapidly and alters the voice. The restricted infantile vocal range expands in both directions of the higher and lower tones until it reaches the adult range. A well-known sign of voice change among boys is the sudden change between a soprano register and that of the developing deeper vocal quality.
VOICE EVALUATION
Vocal quality is assessed from the first moment of contact between physician and patient. Overall vocal quality, degree of nasality, and sharpness of articulation are immediately noted during the routine history. Terms such as harshness, breathiness, pitch breaks, fatigue, and tension are used to characterize the quality. Diagnosis of vocal disorders emphasizes a thorough medical history that includes questions about the onset, duration, and nature of the voice change and about vocal fluctuation and fatigue. Questions should concern the patient’s general habits, including use of tobacco, dietary intake, and vocal demand within the occupational setting, especially if extensive voice use or loud vocal intensity is required.
Other factors that can contribute to voice disorders include postnasal drip from allergic rhinitis or sinusitis, vocal abuse and misuse, exposure to secondhand smoke, gastroesophageal reflux disease (GERD), and respiratory disorders. Associated symptoms such as dysphagia, odynophagia, hemoptysis, or painful phonation may help to categorize the nature of the lesion. Questions related to previous operations involving endotracheal intubation should be explored. Surgical procedures on the neck, cervical spine, chest, or thyroid may result in injury to the recurrent laryngeal nerves. The presence of underlying medical illnesses should be ascertained, as should use of medications that can have a drying effect on the vocal folds, such as antihistamines and anticholinergic agents.
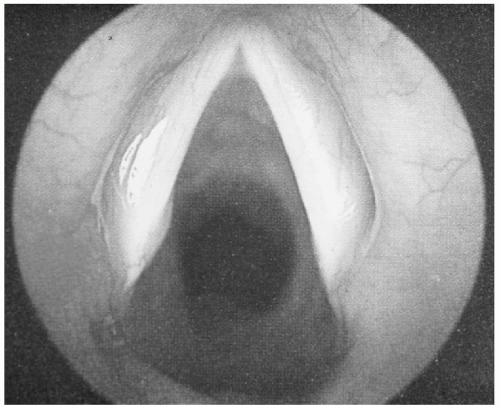
Most vocal disorders can be readily diagnosed by means of listening to the voice, obtaining a history, and performing laryngoscopy in the office. Fiberoptic laryngoscopy greatly facilitates examination of the larynx (Fig. 27-1). The examiner must be familiar with the normal anatomy of the larynx at rest, during quiet breathing, and during phonation when the glottic structures are in motion. In addition, videostroboscopy of the larynx allows examination of the mucosal wave of the vibrating vocal fold and can be used to aid in the diagnosis of vocal disorders. The vocal folds vibrate at approximately 125 Hertz (Hz) in men, 185 Hz in women, and 225 Hz in children. Stroboscopy is used to study the phases of motion of the vocal folds using a light source that is periodically interrupted or pulsed. The intervals between the flashes are regulated, and multiple exposures are taken. Through a series of rapidly changing still images, the optical illusion of apparent slow motion of the vocal folds is created. Factors such as symmetry, periodicity of the vocal fold wave, amplitude of movement, and degree of glottic closure are evaluated during a variety of voicing tasks.
FIG. 27-1. Normal larynx.
VOCAL DISORDERS
The pathophysiologic mechanisms, presentation, and management of vocal disorders are outlined in Table 27-1.
Spectrum of Abuse and Misuse Disorders
Vocal abuse is the result of inappropriate, excessive voluntary tension or strain applied to the vocal cords. An example is the child engaged in constant screaming or shouting. Misuse differs in that the subject is often unaware of the incorrect vocal mechanism. An untrained singer who has developed poor skills to increase vocal volume and a child who phonates by using the neck muscles to “squeeze” the voice are two examples. These improper habits result in a variety of laryngeal changes, which constitute chronic laryngitis (Fig. 27-2). Factors often associated with this process are smoking, exposure to environmental inhalants, and chronic rhinosinusitis with postnasal drip. Reflux of gastric contents can also contribute to laryngeal inflammation, even despite a lack of GERD symptoms (i.e., heartburn, sour taste, dyspepsia). Therapy consists of avoiding foods that increase gastric acid, and raising the head of the bed while sleeping. Pharmacotherapy includes the use of acid neutralizers, H2 blockers, or proton pump inhibitors.
The clinical picture of chronic laryngitis can range from a normal appearing larynx to the presence of mucosal and submucosal edema in the early stages. More advanced findings are those of prenodules. Prenodules are generally no more than submucous hemorrhage and may resolve with voice rest. Hyalinization and organization occur after long-term vocal abuse and produce mature nodules that are hard, white, thickened, and fibrosed. These nodules, also called singer’s nodules or screamer’s nodules (Fig. 27-3), tend to arise bilaterally at the junction of the anterior and middle thirds of the true vocal cords. They are more common among women and children, and their presence implies chronic, severe vocal abuse or misuse. Nodules are the most common cause of hoarseness in the pediatric age group. Primary treatment of patients with vocal nodules is voice therapy in which the patient is taught to prevent vocal abuse and misuse. Further instruction in vocal hygiene, relaxed voicing, and respiration-phonation coordination may also be indicated. Refractory nodules may require surgical excision.
Endotracheal Intubation
Endotracheal intubation can cause direct injury to the larynx. A granuloma forms initially because the endotracheal tube acts as a foreign-body irritant on the larynx. Resolution occurs after extubation; however, treatment with steroids or antireflux pharmacotherapy may be warranted in severe cases. If the granuloma matures and becomes persistent, stenotic lesions can develop, and surgical intervention is necessary followed by a period of strict voice rest.
TABLE 27-1. Pathophysiology, presentation, and management of vocal disorders
Disorder
Pathophysiologic mechanism
Physical examination finding
Treatment
Comments
Trauma related
Chronic laryngitis
Vocal abuse or misuse, reflux, allergies, tobacco use
Inflammation with edema
Avoid causative factors, speech therapy
Nodules
Chronic vocal abuse or misuse
Submucosal hemorrhage (early)
White hard thickened vocal cords (late)
Avoid causative factors, speech therapy
Surgical removal (as last resort)
Children, women
Polyps
Vocal abuse or misuse, reflux, allergies, tobacco use
Fleshy mass on cord
Surgical therapy, avoid causative factors
Old men, smokers
Intubation trauma
Foreign body reaction that produces granulation tissue
Granulation tissue on larynx
Consider steroids, antireflux medications
Recent operation
Neck trauma
Injury or compression of the recurrent laryngeal nerve