Purpose
To present 4 patients that developed hemorrhagic retinal infarction attributable to inadvertent overdose of cefuroxime after cataract surgery.
Design
Case series.
Subjects and Methods
Surgery in 4 patients was complicated—the posterior capsule was absent or torn—and anterior vitrectomy was performed. Cefuroxime was inadvertently injected at a dose higher than recommended in all 4 cases.
Results
Case 1 had hemorrhage in the central and inferior retinal regions, as well as optic atrophy. Case 2 had hemorrhage in the peripapillary and macular regions, as well as optic atrophy. Case 3 had hemorrhage in the peripapillary and inferior retinal regions, as well as macular pucker attributable to fibrovascular formation in the central retinal region. Case 4 had hemorrhage in the peripapillary, macular, and inferior retinal regions. The cefuroxime doses administered to the presented patients were much higher than reported in other cases and resulted in a higher concentration in the vitreous. Consequently, the severity of toxicity was much higher than in other reported cases of cefuroxime-induced toxicity.
Conclusion
In cases of intracameral cefuroxime overdose, hemorrhagic retinal infarction can develop after cataract surgery.
Cefuroxime is a semisynthetic second-generation cephalosporin. Administered via intracameral injection, cefuroxime is frequently used as a prophylaxis for postoperative bacterial endophthalmitis in patients undergoing cataract surgery, because it inhibits gram-positive cocci, gram-negative bacilli, anaerobes, and some spirochetes. The European Society of Cataract and Refractive Surgeons (ESCRS) published the results of a large prospective randomized multicenter study, in which intracameral cefuroxime injection (concentration: 1 mg/0.1 mL) during cataract surgery reduced the risk of postoperative endophthalmitis. When no intracameral cefuroxime was used the risk of endophthalmitis was 5- to 6-fold higher. Intracameral cefuroxime injection has been used routinely by many surgeons during cataract surgery, including in patients with posterior capsular tear and vitreous loss.
In the present retrospective case series we describe 4 eyes in 4 patients that developed retinal and/or optic nerve infarction owing to inadvertent intraocular cefuroxime overdose. The Institutional Review Board of Batman State Hospital (Batman, Turkey) approved the study. The tenets of the Declaration of Helsinki were followed. Patient consent was obtained for use of figures accompanying this paper. The patients did not have any systemic diseases, such as diabetes or hypertension. Cefuroxime was diluted with Ringer’s lactate, prepared in a concentration of 1 mg/0.1 mL, and put in a 10-mL syringe (as a procedural mishap), and ≥5 mL was injected into the eyes. Doubtless, cefuroxime reached the vitreous quite easily, and thus the retina was exposed to an overdose. We use the term hemorrhagic retinal infarction herein because retinal hemorrhage resulting in rapid optic atrophy proves the existence of ischemic changes or infarction.
Case Reports
Case 1
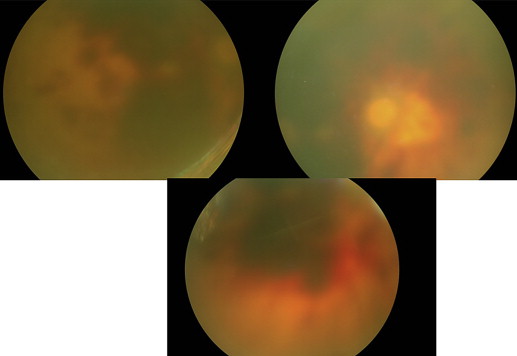
An 80-year-old male patient had corneal haze attributable to trachoma and grade 3 nuclear cataract. Fundus examination showed a normal retina and his preoperative visual acuity was counting fingers from a distance of 1 m. Surgery was complicated because the posterior capsule was torn during the procedure; therefore, anterior vitrectomy was performed and an anterior chamber intraocular lens was implanted. In total, ≥7 mL (70 mg) of cefuroxime (concentration: 1 mg/0.1 mL) was injected. On postoperative day 1 the patient complained of a decrease in vision and could only perceive light. Corneal edema and haze were significant, although development of hemorrhage in the central and inferior retinal regions was noted. Optic atrophy developed 2 weeks post surgery ( Figure 1 ).
Case 2
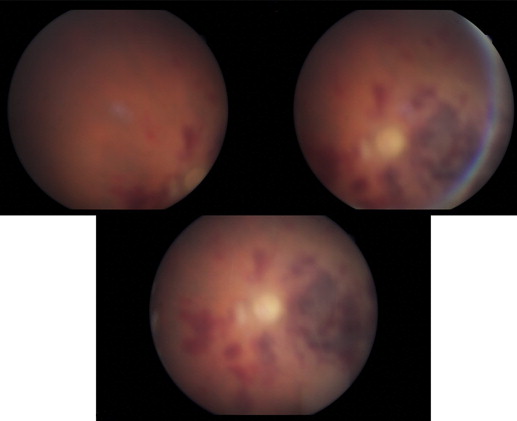
A 70-year-old male patient had an accident involving cow horn backlash 2 years earlier. The patient then underwent limbocorneal suturation and anterior vitrectomy, which resulted in aphakia. The eye lost a large quantity of vitreous during perforation. Funduscopic examination showed a normal retina and the patient’s preoperative visual acuity with a pinhole in the operated eye was 6/10. The surgical procedure was implantation of a secondary scleral-fixated intraocular lens. In total, ≥6 mL (60 mg) of cefuroxime (concentration: 1 mg/0.1 mL) was injected. Postoperatively the patient complained of lack of vision—he could only perceive hand motion. Corneal edema cleared 2 weeks post surgery, but hemorrhage in the peripapillary and macular regions occurred, and optic atrophy was observed ( Figure 2 ).
Case 3
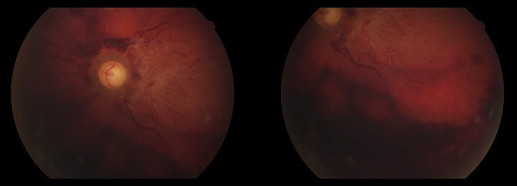
A 60-year-old male patient had subcapsular cataract. Fundus examination showed a normal retina. Preoperative visual acuity was 6/60. During surgery the posterior capsule was torn, and anterior vitrectomy was performed and an anterior chamber intraocular lens was implanted. In total, ≥5 mL (50 mg) of cefuroxime (concentration: 1 mg/0.1 mL) was injected. Corneal edema cleared 4 weeks post surgery, but the patient complained of lack of vision—he could only perceive hand motion. Fundus examination showed hemorrhage in the peripapillary and inferior retinal regions. Additionally, macular pucker attributable to fibrovascular formation was noted ( Figure 3 ).
Case 4
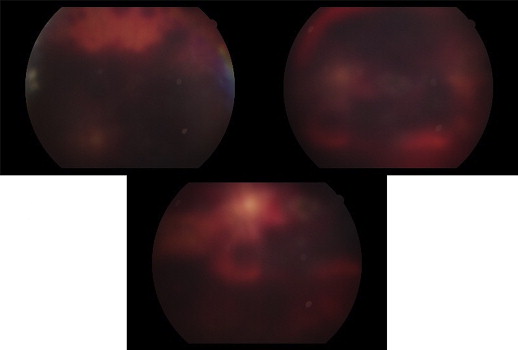
A 75-year-old male patient had brunescent cataract and compromised zonules. Fundus examination was precluded because of cataract and B-mode ultrasound of the eye was normal. Preoperative visual acuity was hand motion. During surgery a large quantity of zonular dialysis occurred, and anterior vitrectomy was performed and a scleral-fixated intraocular lens was implanted. In total, ≥6 mL (60 mg) of cefuroxime (concentration: 1 mg/0.1 mL) was injected. Corneal edema cleared 2 weeks post surgery, but the patient still complained of lack of vision—he could only perceive hand motion. Fundus examination showed hemorrhage in the peripapillary, macular, and inferior retinal regions ( Figure 4 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


