Purpose
To describe the intraoperative use of the Heidelberg Spectralis for ultra-widefield fundus fluorescein angiography in infants.
Design
Retrospective observational case series.
Methods
A modified Heidelberg Spectralis was used to perform ultra-widefield fundus fluorescein angiography in infants undergoing an examination under general anesthesia for a range of retinal vasculopathies. Peripheral angiographic findings, angiographic image acquisition time, and any complications were reviewed.
Results
A total of 22 eyes of 11 infants underwent intraoperative ultra-widefield fundus fluorescein angiography using the modified Heidelberg Spectralis. Ultra-widefield fundus fluorescein angiography was successfully performed in all infants and permitted capture of the posterior pole as well as the peripheral retina in a single shot centered on the macula. Peripheral retinal pathologies captured include neovascularization, capillary nonperfusion, and skip areas from previous laser treatment. Capturing of angiographic images took a mean time of 7.09 minutes. Image artifact from condensation of the ultra-widefield lens was noted during imaging of 1 infant.
Conclusions
The modified Heidelberg Spectralis is an effective and reliable imaging tool for performing ultra-widefield fundus fluorescein angiography in infants. It is capable of capturing wide-angle images of high quality. The technique has advantages as an alternative to RetCam fluorescein angiography in infants undergoing an examination under general anesthesia.
The importance of fundus fluorescein angiography (FA) of the peripheral retina in infants with retinal vasculopathies such as retinopathy of prematurity (ROP), familial exudative vitreoretinopathy (FEVR), and incontinentia pigmenti is well recognized for the diagnosis of neovascularization, capillary nonperfusion, and leakage. Infants are incapable of keeping their eyes open and steady for a long time, which is why conventional outpatient angiography is underused. Our group has shown that the Optos system (Optos PLC, Dunfermline, Scotland, UK) is fast enough to permit ultra-widefield fundus FA in outpatients in premature and term infants aged up to 6 months with or without oral sedation using the “flying baby” position. Beyond 6 months of age, infants are generally too heavy to hold still for such a technique to be effective. Fluorescein angioscopy under general anesthesia using a binocular indirect ophthalmoscope is an option, but it is not ideal as there is no permanent objective record generated for review.
RetCam (Clarity Medical System, Pleasanton, California, USA) is currently the only widely available imaging modality used to perform FA on a supine infant under general anesthesia. Peripheral sweeps and montage techniques are often necessary when information about the retinal periphery is required. These techniques are labor intensive, require highly skilled photographers, and do not permit the simultaneous capture of the posterior pole and periphery in a single frame, limiting the evaluation and comparison of the phases of the angiogram across different parts of the fundus.
The Heidelberg Spectralis ultra-widefield fundus FA imaging system (Heidelberg Engineering, Heidelberg, Germany) is said to capture a wider field of view of the fundus in a single photograph without ocular surface contact. This imaging modality has been used to evaluate an adult patient with Von Hippel-Lindau syndrome.
The Heidelberg Spectralis has been used previously in infants for spectral-domain optical coherence tomography (OCT). Since November 2012, we have been using the Heidelberg Spectralis ultra-widefield fundus FA imaging modality intraoperatively as part of our routine clinical care and management of infants with retinal vasculopathies.
The purpose of this report is to describe the findings of an audit that retrospectively reviewed all infants who underwent intraoperative ultra-widefield fundus FA with the Heidelberg Spectralis in a National Health Service tertiary center setting. The technique adopted for performing intraoperative ultra-widefield fundus FA and the utility, angiographic findings, and complications of ultra-widefield fundus FA were reviewed in our group of infants. In addition, the fundal field of view obtained with the Heidelberg Spectralis ultra-widefield lens was compared with the RetCam 130-degree lens using a schematic infant model eye.
Patients and Methods
Institutional board approval at the Oxford Eye Hospital was granted and logged permitting an audit that retrospectively reviewed all case records of infants who underwent an examination under general anesthesia with intraoperative ultra-widefield fundus FA with the Heidelberg Spectralis for routine clinical care over an 18-month period (November 1, 2012 to April 30, 2014). The review of infants was carried out in accordance with the Data Protection Act and the Declaration of Helsinki. Informed written parental consent for the angiography procedure had been obtained for all infants.
The ultra-widefield fluorescein angiographic imaging modality for the Heidelberg Spectralis was purchased by our hospital using charitable funds following a cost-neutral loan for 2 weeks in 2012.
Ultra-widefield fundus FA was performed with 10% fluorescein administered intravenously as a bolus at a dose of 0.1 mL/kg, followed by a 5 mL 0.9% saline flush. Mydriasis was obtained with 0.5% cyclopentolate and 2.5% phenylephrine. A Liebermann pediatric speculum (Duckworth & Kent, Hertfordshire, UK) was used to retract the eyelids.
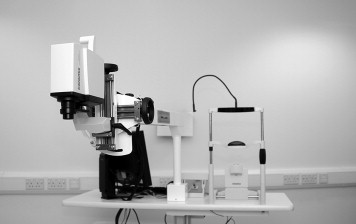
Infants were imaged with the Heidelberg Spectralis imaging system, consisting of a scanning laser ophthalmoscope (SLO) camera head connected, through a flexible fiberoptic cable, to a moveable cart housing the retinal viewing screen and the touch panel. To image infants in a supine position, the imaging system was modified by disassembling the SLO camera head from its mount by removing the Allen screw that secures it at the bottom of the arc guide. The SLO camera head was then mounted onto a multi-positional bracket at the end of a customized adjustable arm (Base Design Limited, Great Dunmow, Essex, UK) and secured tightly by a bolt ( Figure 1 ). Adjustable wheel handles on the bracket allowed 4 degrees of freedom of movement to enable adjustment and optimization of alignment of the SLO camera head to the infant’s eyes.
All images were obtained in the operating room with the photographer at the head of the bed. During image acquisition, the SLO camera head was stabilized by resting the hand on the adjustable arm to keep movement of the arm and the camera head to a minimum. An assistant operated the computer software while the photographer obtained the images. To obtain images of the highest quality, the high-resolution acquisition modality in the fluorescein angiography mode was used. Regular corneal hydration with a balanced salt solution was necessary to improve the clarity of images and to preserve the integrity of the corneal surface. Imaging of the retina up to the ora serrata was made possible by rotating the globe with a toothed forceps and indenting the sclera with a squint hook. The images obtained appeared upright on the retinal viewing screen as the computer software automatically corrected the orientation of the SLO camera head at the time of imaging.
For each infant, the data reviewed included age, sex, gestational age, age at imaging, birth weight, diagnosis, treatment, and any complications that occurred. All retinal images were reviewed on the Heidelberg Eye Explorer software. The duration of the imaging process was defined as the difference in time between the first and last image captured, which is automatically recorded. Peripheral angiographic findings and the presence of any artifacts were evaluated from the images.
Results
Over an 18-month period, a total of 22 eyes of 11 infants underwent intraoperative noncontact ultra-widefield fundus FA using the modified Heidelberg Spectralis. Of the 11 infants, 6 were male and 5 were female. Eight patients were premature infants diagnosed with ROP with a mean gestational age of 24.75 weeks (range 23–26 weeks) and a mean birth weight of 744.38 g (range 650–870 g). Mean postnatal age at imaging was 47.38 weeks (range 33–91 weeks). Three patients were term infants with diagnoses of incontinentia pigmenti and FEVR with a mean age of 7 months (range 3–12 months). Tables 1 and 2 summarize the demographics, diagnoses, angiographic findings, and the utility of ultra-widefield fundus FA in our group of infants.
| Infant | Gestational Age (Weeks) | Birth Weight (g) | Postnatal Age (Weeks) | Sex | Diagnosis | Peripheral Angiographic Findings | Utility of Ultra-widefield Fluorescein Angiography |
|---|---|---|---|---|---|---|---|
| 1 | 26 | 870 | 44 | Male | ROP | Peripheral leakage and nonperfusion | Targeted laser treatment |
| 2 | 26 | 665 | 41 | Male | ROP | Peripheral leakage and nonperfusion | Targeted laser treatment |
| 3 | 24 | 575 | 33 | Female | ROP | Peripheral leakage | Diagnosis |
| 4 | 24 | 790 | 41 | Male | ROP | Peripheral leakage and nonperfusion | Targeted laser treatment |
| 5 | 23 | 650 | 91 | Male | ROP | Peripheral nonperfusion | Targeted laser treatment |
| 6 | 25 | 850 | 49 | Male | ROP | Peripheral nonperfusion, laser skip areas | Targeted laser treatment |
| 7 | 24 | 785 | 36 | Male | ROP | Resolution of peripheral leakage | Assessment of previous treatment |
| 8 | 26 | 770 | 44 | Female | ROP | Peripheral leakage | Targeted laser treatment |
| Infant | Age (Months) | Sex | Diagnosis | Peripheral Angiographic Findings | Utility of Ultra-widefield Fluorescein Angiography |
|---|---|---|---|---|---|
| 1 | 3 | Female | Familial exudative vitreoretinopathy | Peripheral leakage | Targeted laser treatment |
| 2 | 12 | Female | Incontinentia pigmenti | Normal | Documentation |
| 3 | 6 | Female | Incontinentia pigmenti | Peripheral ischemia | Targeted laser treatment |
Ultra-widefield fundus FA was successfully carried out in all infants and permitted capture of the posterior pole as well as the peripheral retina in a single shot centered on the macula ( Figure 2 ). All infants had infrared reflectance images obtained with the ultra-widefield lens prior to the acquisition of ultra-widefield fluorescein angiographic images ( Figure 3 ).



