Purpose
To report the technique, timing, and outcomes of the Ahmed glaucoma drainage device in eyes with the modified osteo-odonto-keratoprosthesis (MOOKP) and the role of an additional stage 1A to the Rome-Vienna protocol.
Design
Retrospective interventional case series.
Methods
Case records of 22 eyes of 20 patients with high intraocular pressure at various stages of the MOOKP procedure performed in 85 eyes of 82 patients were studied. Stage 1A, which includes total iridodialysis, intracapsular cataract extraction, and anterior vitrectomy, was done in all eyes as the primary stage.
Results
Seventeen Ahmed glaucoma drainage devices were implanted in 15 eyes of 14 patients (chemical injury in 9 [10 eyes] and Stevens-Johnson syndrome in 5 patients). Implantation was performed during and after stage 1A in 2 and 7 eyes, respectively, after stage 1B+1C in 1 eye, and after stage 2 in 6 eyes. Eleven of 15 eyes (73.3%) remained stable with adequate control of intraocular pressure over a mean follow-up period of 33.68 months (1–90 months). Complications related to the drainage device were hypotony in 1 eye and vitreous block of the tube in 1 eye.
Conclusion
It is ideal to place the Ahmed glaucoma drainage device prior to the mucosal graft when the anatomy of the ocular surface is least altered with best outcomes. The technique of placement of the drainage device during the various stages of the MOOKP procedure has been described. The intraocular pressure stabilized in three quarters of the eyes with pre-existing glaucoma.
The modified osteo-odonto-keratoprosthesis (MOOKP) procedure is performed to restore sight in end-stage ocular surface disorders where conventional penetrating keratoplasty would have a high risk of failure. The most common indications for the procedure include chemical injuries and Stevens-Johnson syndrome (SJS). Glaucoma is one of the most common comorbid factors in these eyes and occurs more often with chemical injuries. Management of glaucoma forms an important concern in eyes undergoing any form of keratoprosthesis surgery. Detection of and monitoring the progression of glaucomatous damage in these eyes is challenging. However with the newer techniques of optic disc imaging and nerve fiber layer analysis, as well as Humphrey visual field testing, progression can be documented reliably in these eyes. Since available tonometers are not reliable to measure the intraocular pressure (IOP) in eyes with keratoprosthesis, the mainstay of measuring the IOP in these eyes is by digital tonometry (the pressure is measured using finger tension). The conventional antiglaucoma procedure of trabeculectomy is not an option with MOOKP. Diode transscleral and endocyclophotocoagulation have been described earlier with their risks and shortcomings. Drainage devices therefore form the mainstay of glaucoma management in these eyes. However, details regarding the technique of shunt procedures using these devices at various stages of the MOOKP surgery have not been described earlier in literature. In this paper we have described the technique and timing as well as analyzed the outcomes of the Ahmed glaucoma drainage device for glaucoma in eyes undergoing the MOOKP procedure. The role of an additional primary stage 1A procedure in contributing toward lowering of IOP as well as deciding the need for an Ahmed glaucoma drainage device has also been highlighted.
Patients and Methods
The approval of the Institutional Review Board of Vision Research Foundation, Chennai, India was obtained for this study, which adhered to the tenets of the Declaration of Helsinki. Case records of patients who underwent Ahmed glaucoma drainage device implantation for glaucoma prior to, during, or following the various stages of the MOOKP procedure were analyzed retrospectively. Based on the digital tension, the need for maximum systemic acetazolamide, and the optic disc features noted intraoperatively during stage 1A of the MOOKP procedure, the timing of the Ahmed glaucoma drainage device placement was decided. Preoperative evaluation included a complete ophthalmologic evaluation, including ultrasound biomicroscopy, if possible, to evaluate anterior chamber and angle details. The MOOKP at our center broadly follows the guidelines and stages described in the Rome-Vienna Protocol. In addition, we routinely perform stage 1A prior to the other 2 stages described in the protocol.
Stages of Modified Osteo-odonto-keratoprosthesis Procedure
Stage 1A, the additional primary stage routinely performed at our center, includes total iridodialysis, intracapsular cataract extraction, and anterior vitrectomy. A tectonic penetrating keratoplasty is performed in eyes with corneal thinning or perforation. Fundus evaluation by means of indirect ophthalmoscopy is performed prior to removal of the crystalline lens to assess the status of the retina as well as the optic nerve head. Stage 1B+C, done 1 month following stage 1A, includes placing the mucous membrane graft over the ocular surface, fashioning the osteo-odonto-alveolar lamina, and placing it in the subcutaneous pouch in the cheek. Stage 2 is performed 3 months later. The lamina is placed in the eye and the mucous membrane is placed back, allowing the cylinder to protrude through a central opening made in the mucosa. The placement of the Ahmed glaucoma drainage device can be performed along with or following any of the above-mentioned stages.
Definition of Glaucoma
Glaucoma was diagnosed based on 1 or more of the following factors: a vertical cup-to-disc ratio of 0.7 or more and/or any notching noted during stage 1A; the preoperative digital tension; and the preoperative need for use of systemic acetazolamide.
Post stage 2, glaucoma was defined based on the structural appearance as mentioned above and the visual field defect corresponding to the optic nerve changes. Assessment of cup/disc asymmetry is usually not possible in these bilateral end-stage disorders, owing to nonvisualization of the disc in the other eye, and hence cannot be used as a criterion to define glaucoma. Progression was defined as an increase in the cup-to-disc ratio by 0.2 or more with an increase in the visual field defect, with raised digital tension. In eyes with advanced cupping, only the visual field changes and digital tension provided a clue toward progression.
Surgical Technique
Placement of ahmed glaucoma drainage device before or after stage 1A
A 360-degree conjunctival peritomy is performed. The superior and lateral rectus muscles are tagged to expose the superotemporal quadrant. The limbus is usually identified in most cases. The plate of the Ahmed glaucoma drainage device is placed deep in the superotemporal fornix and is secured 8 mm from the limbus using 8-0 nylon sutures. The tube length is adjusted to protrude3–4 mm beyond the limbus and cut accordingly in a bevel-up fashion. The anterior chamber is entered at the limbus using a 23 or 24 gauge needle and the tube is inserted into the anterior chamber through the entry site. The tube is secured midway to the sclera using 8-0 nylon sutures. The tube is covered using a scleral patch graft that is secured to the sclera using fibrin glue. The conjunctival edges are opposed to each other (in cases of severe forniceal shortening) or secured at the limbus using 8-0 vicryl sutures. Tarsorrhaphy sutures using 5-0 mersilk are placed laterally and/or medially to prevent retraction of the conjunctiva in eyes with shortened fornices.
Placement of ahmed glaucoma drainage device following stage 1B
A full-thickness curvilinear incision is placed on the mucosa extending on either side of the superior rectus and the lateral rectus for 4–5 clock hours. Hemostasis is achieved with constant suction and judicious use of cautery. The buccal mucosa is dissected off the sclera and reflected back to expose the limbus. The superior and lateral rectus muscles are tagged. The superotemporal quadrant is exposed adequately for placement of the Ahmed glaucoma drainage device as described above until placement of the scleral patch graft to cover the tube. The buccal mucosa is reflected back over the scleral graft and the incised edges are sutured using 7-0 vicryl absorbable sutures.
Placement of ahmed glaucoma drainage device following stage 2
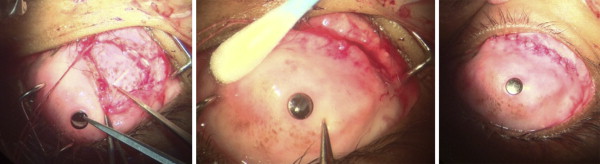
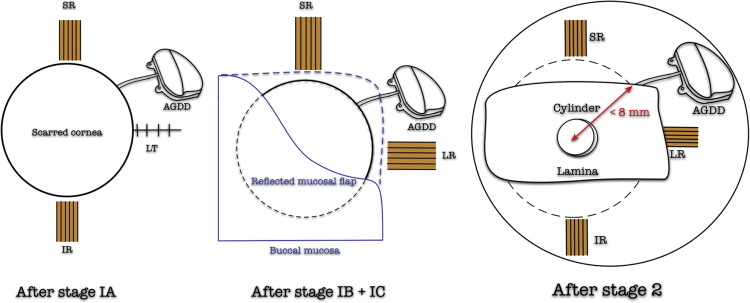
A full-thickness curvilinear incision is placed on the mucosa extending from medial to the superior rectus to inferior to the lateral rectus for 4–5 clock hours. Hemostasis is achieved with constant suction and cautious use of cautery. The buccal mucosa is dissected off the sclera and reflected back to expose the lamina edge. The superior and lateral rectus muscles are tagged if required. The distance of the lamina edge from the center of the cylinder is measured and the anterior chamber entry is made flush along or just anterior to the edge of the lamina. The entry site is made within 9 mm from the center of the lamina so as to be anterior to the pars plana. The superotemporal quadrant is exposed adequately for placement of the device plate as described above until placement of the scleral patch graft to cover the tube. The presence of the tube in the eye is confirmed by visualizing the tube edge beneath the cylinder if possible. The buccal mucosa is reflected back over the scleral graft and the incised edges are sutured using 7-0 vicryl absorbable sutures ( Figure 1 ). A schematic representation of the Ahmed glaucoma drainage device following the 3 stages is shown in Figure 2 .
Post–Modified Osteo-odonto-keratoprosthesis Follow-up Protocol
Topical lubricants and antibiotic ointment were continued indefinitely. Systemic acetazolamide was used based on need for up to 6 months after the surgery. The eye was subjected to a thorough clinical examination, posterior segment evaluation with a 90-diopter lens, Humphrey visual field testing every 6 months, B-scan ultrasound, and spiral computed tomography of the lamina once a year. All patients had a descriptive record of the disc details at every visit. A photographic documentation at each visit was not possible. Humphrey visual fields 24-2 and 10-2 were performed in all eyes once every 6 months.
Results
Demographics
Eighty-five eyes of 82 patients underwent the MOOKP procedure at our center between March 2003 and March 2013. Of the 85 eyes that underwent the MOOKP procedure, 44 belonged to the SJS group and 37 to the chemical injury group, with a mean (range) follow-up of 36.93 months (1–90 months) and 30.42 months (1–80), respectively. Four eyes belonged to other etiologies. Twenty-one eyes of 19 patients had glaucoma as defined. One patient was referred to our center for second shunt placement surgery and was included in the study. Of these 20 patients, 15 eyes of 14 patients underwent the Ahmed glaucoma drainage device procedure (17 devices) at various stages of the MOOKP procedure. These included 10 male and 4 female patients with ages ranging from 23 to 54 years. The primary etiology was chemical injury in 9 patients and Stevens-Johnson syndrome in 5 patients. Among the SJS group, 3 had prior intraocular surgeries for corneal perforation and 1 was the patient operated elsewhere for the MOOKP procedure. The Ahmed glaucoma drainage device was implanted in the eye during stage 1A in 2 eyes, following stage 1A in 7 eyes, after stage 1B+1C in 1 eye, and after stage 2 in 6 eyes (twice in 1 eye, accounting for 7 valves). The other eye of the same patient had 2 devices implanted: 1following stage 1A and the other subsequent to stage 2. Clinical features, the timing of Ahmed glaucoma drainage device placement, and their outcomes have been listed in the Table .
| S. No | Age/Sex | Etiology | Prior Intraocular Procedures/Duration at Which AGV Done | Best BCVA | Final BCVA | Disc Status a —Progression | Follow-up in Months | Comments |
|---|---|---|---|---|---|---|---|---|
| With stage 1A | ||||||||
| 1 | 31/M | Chemical | None | 20/50 | 20/50 | 0.9 | 36 | Hypotony—tube ligated 2 m later |
| 2 | 24/F | Chemical | Bulbar mucosal graft done elsewhere for ocular surface reconstruction | 20/40 | 20/40 | 0.6 | 24 | UBM—angle closed |
| After stage 1A | ||||||||
| 1 | 24/M | Chemical | PK + KLAL 3 m after 1A | 20/30 | 20/30 | 0.9 | 72 | Stable UBM—angle closed |
| 2 | 35/M | Chemical | 9 m after 1A | 20/50 | 20/400 | 0.6 | 36 | Thick RCM plastered to iris as seen during stage 1A RD following YAG |
| 3 | 33/M | Chemical | Diode CPC 12 m after 1A | 20/40 | 20/40 | 0.9 | 72 | Anterior segment formed on slit-lamp evaluation Diode CPC 1 m before 1A |
| 4 | 41/M | Chemical | 12 m after 1A | 20/30 | 20/30 | Adv cupping | 67 | Stable UBM—angle closed |
| 5 | 28/M | SJS | Diode CPC – twice; 3 m after 1A | PL | PL | 36 | High myopia—RD 3 m after stage 2—refused intervention | |
| 6 | 33/F | SJS | 1 m after 1A | PL | PL | Adv cupping | 1 | Well-formed anterior segment noted during 1A GOA noted at 1A |
| 7 | 34/F | Chemical | PK 2 years prior/11 m after 1A | PL | 20/30 | PL | 63 | ?endophthalmitis-related phthisis |
| After stage 1B+C | ||||||||
| 1 | 54/M | SJS | PK for corneal perforation 6 m prior to 1B+C/2 m after 1B+C | 20/150 | 20/150 | 0.8 | 48 | Stable |
| After stage 2 | ||||||||
| 1 | 33/M | Chemical | Diode CPC/18 m after stage 26 y after stage 2 | 20/30 | 20/60 | Adv | 84 | Progression 6 y after 1st valve/stable 1 y after 2nd |
| 2 | 33/M | Chemical | Diode CPC/6 y after stage 2 | 20/30 | 20/40 | Adv | 72 | Progression 6 y after 1st valve/stable 1 y after 2nd |
| 3 | 29/M | Chemical | 3 y after stage 2 | 20/30 | PL | 0.9 | 60 | Sterile vitritis with laminar resorption—lamina removed |
| 4 | 40/F | SJS | Stage 1A done for leaking cystoid cicatrix 3 y prior/3 y after stage 2 | 20/80 | 20/120 | 0.7–0.9 | 74 | Stable |
| 5 | 25/M | Chemical | 2 m after stage 2 | 20/150 | 20/150 | 0.6 | 48 | Stable fibrous band from disc cause for reduced BCVA |
| 6 | 50/M | SJS | 2nd valve placed 6 m after stage 2 | 20/30 | 20/30 | Adv cupping | 24 | Stable 1st valve placed prior to stage 2—MOOKP surgery done elsewhere |
| AGV not done | ||||||||
| 1 | 40/M | Chemical | 20/30 | NPL | 0.6 | 5 | Uncontrolled IOP on acetazolamide developed endophthalmitis in 5 m—removed lamina | |
| 2 | 24/M | Chemical | 20/20 | NPL | Adv cupping | 24 | NPL owing to absolute glaucoma—same lamina shifted to the other eye | |
| 3 | 33/M | Chemical | Diode CPC | 20/60 | PL | 0.8 | 60 | Laminar resorption—removed |
| 4 | 44/M | Chemical | PK-twice; once for corneal perforation | 20/130 | 20/130 | 12 | Stable | |
| 5 | 40/M | Chemical | 20/400 | 3/60 | Adv cupping | 36 | Stable | |
| 6 | 23/M | Chemical | 20/30 | PL | 0.8 | 48 | Laminar resorption—removed | |
| 7 | 30/M | Chemical | 20/400 | 20/400 | Disc pallor | 12 | Stable | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


