Glaucoma: Clinical Trials in Glaucoma Therapy
Daniel Warder MD
Robert J. Campbell MD, MSc, FRCSC
Glaucoma, with its characteristic optic nerve pathology and associated visual field (VF) defects, results from a heterogeneous group of eye disorders. While many risk factors have been identified for the development and progression of glaucoma, intraocular pressure (IOP) takes center stage as the only significant modifiable risk factor, and glaucoma management currently hinges on IOP reduction. The clinical armamentarium used to achieve IOP reduction includes numerous medications as well as laser and incisional surgery. This chapter first reviews the pivotal clinical trials addressing the efficacy of lowering IOP in the treatment of glaucoma. Subsequent sections describe studies reporting on specific medical, laser, and surgical therapies for glaucoma.
I. INTRAOCULAR PRESSURE REDUCTION IN THE PREVENTION AND TREATMENT OF GLAUCOMA
Overview
The studies reviewed in this section have been instrumental in defining the modern management of glaucoma. These large, multicentered prospective studies demonstrated that lowering IOP is an effective treatment strategy. Specifically, the Ocular Hypertension Treatment Study (OHTS)1,2,3,4,5,6,7 showed that lowering IOP can prevent the development of glaucoma in patients with ocular hypertension. The Early Manifest Glaucoma Trial (EMGT)8,9,10,11,12,13,14 and the Collaborative Normal-Tension Glaucoma Study (CNTGS)15,16,17,18,19,20 both demonstrated that lowering IOP decreases the risk of glaucoma progression. Finally, although the Advanced Glaucoma Intervention Study (AGIS)21,22,23,24,25,26,27,28,29,30,31,32,33,34,35 was designed to compare surgical versus laser therapies in advanced glaucoma patients, this study is discussed in this section because of its importance in demonstrating the relationship between IOP control and the risk of progression in advanced glaucoma.
Ocular Hypertension Treatment Study
Results published 2002
The OHTS was a multicenter, randomized, controlled clinical trial (RCT) assessing the risk of conversion from ocular hypertension to primary open-angle glaucoma (POAG) in patients with medically lowered IOP compared to patients observed with no treatment.
Study Population
Enrolled patients had moderate-risk ocular hypertension without evidence of glaucomatous optic neuropathy.
Major Inclusion Criteria
IOP in at least 1 eye ≥24 and ≤32 mmHg
IOP in fellow eye ≥21 and ≤32 mmHg
Normal and reliable Humphrey 30-2 Visual Filed VF (two consecutive)
Normal optic discs in both eyes on clinical exam and stereo photos
Major Exclusion Criteria
Sample Size and Baseline Characteristics
1,637 subjects were recruited. Mean age was 55 years. Mean baseline IOP was 24.9 mmHg.
Intervention
Patients were randomized to treatment using topical hypotensive medications (drug choice was at the discretion of the treating ophthalmologist; n = 817) or observation (n = 819). In the treatment arm, medications were added as needed to achieve an IOP that was both 20% below baseline and ≤24 mmHg. Follow-up was carried out every 6 months for a minimum of 5 years.
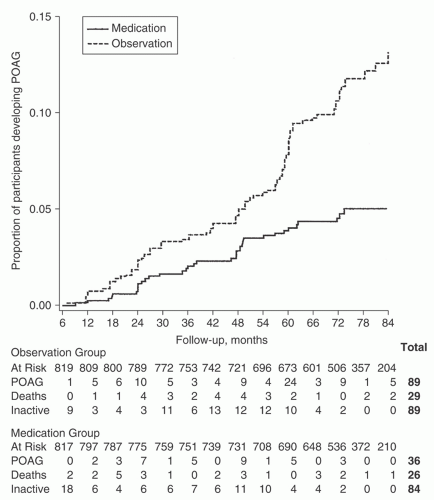 FIGURE 6.1 Kaplan-Meier plot of the cumulative probability of developing primary open-angle glaucoma (POAG) of the randomized group. The participants at risk were those who had not developed POAG at the beginning of each 6-month period. The number of participants classified as developing POAG is given for each interval. Participants who did not develop POAG and withdrew before the end of the study or who died are censored from the interval of their last completed visit. Reprinted with permission from Arch Ophthalmol. 2002;120:707. |
Outcome Measures
The primary endpoint was the conversion to POAG as defined by either a reproducible VF abnormality or reproducible optic disc cupping attributable to POAG. Adverse effects of treatment were also assessed.
Results
The cumulative probability of conversion to POAG was significantly lower in the treatment group versus the observation group during the course of the study (hazard ratio, 0.40; p < 0.0001; Fig. 6.1). Conversion to POAG
at 5 years was 4.4% in the treatment group versus 9.5% in the observation group.
at 5 years was 4.4% in the treatment group versus 9.5% in the observation group.
Baseline Factors Associated with Conversion to Primary Open-Angle Glaucoma
Baseline factors predictive of the development of POAG by both univariate and multivariate analysis included advanced age, higher IOP, greater pattern standard deviation, thinner central corneal thickness (CCT), and larger vertical cup-to-disc ratio. A subgroup analysis of the 25% of participants that self-identified as being African American found a higher rate of conversion to POAG in both study arms. The median follow-up for this subgroup was 78 months, with conversion to POAG occurring in 8.4% in the treatment group and 16.1 % in the observation group. However, race was not an independent predictor in multivariate analysis. This was explained by African American participants having larger baseline vertical cup-to-disc ratios and thinner CCTs, which when adjusted for in the multivariate model made race nonpredictive. CCT showed a striking predictive effect on the development of POAG (multivariate hazard ratio [HR] = 1.71 per 40 µm thinner). The OHTS also highlighted the compounded risk associated with decreasing CCT and increasing baseline IOP. For example, 36% of participants in the observation group with CCT ≤ 555 µm and baseline IOP > 25.75 mmHg developed POAG within 5 years (Fig. 6.2).
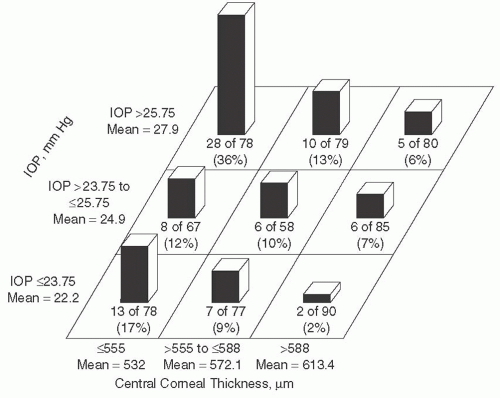 FIGURE 6.2 The percentage of participants in the observation group who developed primary open-angle glaucoma (median follow-up 72 months) grouped by baseline intraocular pressure (IOP) of ≤23.75, >23.75 to 25.75, and >25.75 mmHg and by CCT measurements of 555, >555 to 588, and >588 µm. These percentages are not adjusted for length of follow-up. Reprinted with permission from Arch Ophthalmol. 2002;120:718. |
Clinical Implications
The OHTS demonstrated that IOP reduction reduces the risk of conversion from ocular hypertension to POAG. However, the total number of patients developing glaucoma was quite small (9.5% in the untreated group at 5 years). This resulted in a large number needed to treat (NNT) of 20 to prevent one patient from developing early POAG. This study also highlighted some important risk factors that are predictive of conversion to POAG, such as thin CCT (especially when combined with higher
baseline IOP). Hence, using these predictive factors and risk calculations now allows clinicians to more accurately predict risk in individual patients in order to refine treatment decisions. Notably, while the OHTS found that increased pattern standard deviation and cup-to-disc ratio were predictive factors of conversion to POAG, patients with these findings at baseline may have already had early glaucoma. This would not be expected to alter the main findings of this trial, but could affect its generalizability.
baseline IOP). Hence, using these predictive factors and risk calculations now allows clinicians to more accurately predict risk in individual patients in order to refine treatment decisions. Notably, while the OHTS found that increased pattern standard deviation and cup-to-disc ratio were predictive factors of conversion to POAG, patients with these findings at baseline may have already had early glaucoma. This would not be expected to alter the main findings of this trial, but could affect its generalizability.
Early Manifest Glaucoma Trial
Results published 2002
The EMGT was a multicenter, randomized, unmasked, controlled clinical trial designed to determine if lowering IOP in newly diagnosed glaucoma patients decreases the risk of disease progression.
Study Population
The EMGT enrolled patients with early-stage OAG. In order to identify patients with glaucoma that had not yet received treatment for their disease, a screening program was undertaken at multiple sites in Sweden, ultimately screening over 44,000 people to accrue an appropriate number of patients for the study.
Major Inclusion Criteria
Newly diagnosed, untreated OAG
Diagnosis based on repeatable VF defects in at least one eye compatible with glaucoma (based on the Glaucoma Hemifield Test), not explained by other causes
Included POAG, normal-tension glaucoma, and exfoliative glaucoma
Major Exclusion Criteria
Advanced VF defects (mean deviation [MD] worse than -16 dB), or threat to fixation
Mean IOP > 30 mmHg or any IOP > 35 mmHg
Sample Size and Baseline Characteristics
A total of 255 patients were included in the study. The mean age was 68 years and 66% were females. Average IOP was 20.6 mmHg and median VF MD was -4 dB; 25 patients (10%) had pseudoexfoliation.
Intervention
Patients were randomized to treatment with topical betaxolol plus a single session of 360° argon laser trabeculoplasty (ALT; n = 129) or to observation (n = 126). There was no specific target IOP in this study; however, the protocol did specify the addition of latanoprost if IOP exceeded 25 mmHg in the treatment group. Follow-up was carried out every 3 months for a minimum of 4 years.
Outcome Measures
Progression of glaucoma was the primary outcome—defined as VF progression (at least three progressing test points in the same location in three consecutive VF tests compared to baseline) or optic disc changes (identified by flicker chronoscopy and confirmed by nonflicker side-by-side photo comparisons).
Results
In the treatment group, the mean IOP was reduced from 20.6 to 15.5 mmHg (25% reduction) and the reduction was maintained throughout the study period. IOP was not significantly changed in the observation group. The median follow-up times were 66 and 69 months for the treatment and control groups, respectively. Progression of glaucoma was more common in the control patients, occurring in 62% of patients (78/126) compared to 45% (58/129) of treated patients (p = 0.007). Figure 6.3 shows progression over time in all study patients and demonstrates an early separation between study arms that was maintained throughout. Median time to progression (Kaplan-Meier cumulative survival) was 48 months in controls compared to 66 months in treated patients, indicating a delay in progression with treatment. All except one patient that met the criteria for progression did so based on VF criteria (with or without optic disc changes).
Baseline Factors Associated with Progression
Baseline factors associated with progression in multivariate analysis included older
age (>67 years; HR 1.47), higher IOP (> 21 mmHg; HR 1.70), more negative MD (≤−4 dB; HR 1.58), and the presence of pseudoexfoliation (HR 2.22). Higher frequency of disc hemorrhages at follow-up visits was also associated with progression.
age (>67 years; HR 1.47), higher IOP (> 21 mmHg; HR 1.70), more negative MD (≤−4 dB; HR 1.58), and the presence of pseudoexfoliation (HR 2.22). Higher frequency of disc hemorrhages at follow-up visits was also associated with progression.
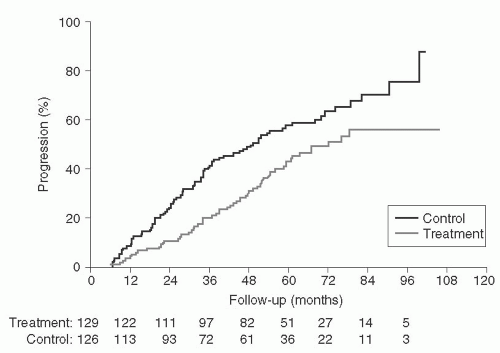 FIGURE 6.3 Progression across time in patients of the study group. The cumulative probability of patients with progression was larger in the control group than in the treatment group (p = 0.007). The number of patients at risk for progression of glaucoma in the treatment group and control group is shown below the x-axis. Reprinted with permission from Arch Ophthalmol. 2002;120:1272. |
Clinical Implications
The EMGT was the first large RCT (and likely the last) in which patients with manifest glaucoma and elevated IOP could be randomized to observation alone. This study showed that a pressure reduction of 25% in newly diagnosed glaucoma patients decreases the risk of progression, with an NNT of approximately 6 (over approximately 6 years). The EMGT enrollment protocol, which consisted of a population screening program, yielded a study patient sample that was highly reflective of the underlying population with glaucoma. This, combined with the high patient retention and rigorous study protocol, supports the validity and generalizability of the results. While the high rate of glaucoma progression observed may have resulted from overly sensitive VF progression criteria, these criteria were necessary from an ethical standpoint in order to detect the earliest progression in the observation group. Because this effect was nondifferential, it would not be expected to influence the overall study conclusions.
In contrast to the OHTS, which identified conversion to POAG in the majority of patients based on optic disc changes,3 the EMGT found progression by VF criteria in an overwhelming majority of the patients that progressed. This highlights differences between the studies in the relative sensitivity of the VF and optic nerve criteria used to define progression.
Collaborative Normal-Tension Glaucoma Study
Results published 1998
The CNTGS was a multicenter, randomized, controlled, unmasked trial designed to determine if lowering IOP decreases the risk of progression in normal-tension glaucoma.
Study Population
The target population for this study was patients with “normal-tension” glaucoma.
Major Inclusion Criteria
Glaucomatous optic disc and VF abnormalities based on three reliable static-perimetry VFs
Median untreated IOP (or IOP after a 4-week medication washout) ≤20 mmHg with no measurements >24 mmHg and not more than one measurement of 23 to 24 mmHg
Evidence of disease progression, a VF defect threatening fixation, or an optic disc hemorrhage
Major Exclusion Criteria
Use of a systemic beta-blocker or clonidine
Presence of a nonglaucomatous condition causing VF defects
Previous laser or intraocular surgery
Visual acuity less than 20/30
Sample Size and Baseline Characteristics
A total of 230 patients were enrolled in the evaluation for eligibility phase of the study; 145 eyes of 145 patients ultimately met the criteria for randomization. The mean baseline IOPs were 16.1 and 16.9 mmHg in the observation and treatment groups, respectively. The mean age of patients was 66 years.
Intervention
Patients were randomized to observation (n = 79) or a 30% IOP reduction (n = 61) using medical or surgical intervention, at the discretion of the treating clinician. Treatment was augmented as required in the latter group to maintain a 30% reduction from baseline throughout the study period, except in those undergoing filtration surgery, where a 20% IOP reduction was accepted in order to limit the number of procedures a patient would undergo. Patients were followed every 3 months for the first year and every 6 months thereafter. If the endpoint of disease progression was reached, therapeutic constraints were lifted and patients were treated at the discretion of the treating clinician.
Outcome Measures
The primary endpoint was disease progression as defined in the protocol by VF progression (scotoma deepening, expansion, or newly appearing) verified by two of three VFs done within 1 month, and two of three VFs done 3 months later, or optic disc change (stereophotographs agreed upon by two experts). An additional VF analysis was included, which defined progression as having occurred when four-of-five consecutive VFs showed deterioration relative to baseline (“four-of-five” criterion).
Results
During the study period, IOP was unchanged at 16.0 mmHg in the observation group and was reduced to an average of 10.6 mmHg in the treatment group (37% reduction). Using the primary VF endpoints, 35% of the control group and 12% of the treatment group progressed over 5 years (p = 0.0001). Using the “four-of-five” analysis of progression, the difference was smaller, however still significant, with 30% of the control group and 18% of the treatment group showing progression (p = 0.01). It is important to note that when an intent-to-treat analysis was performed, there was no significant difference in progression between the two groups, with 39% and 33% of the observation and treatment groups showing progression, respectively (p = 0.21; Fig. 6.4). However, after adjusting the VF data to account for cataract development, the difference in progression between the two groups in the intent-to-treat analysis became significant, with 27% and 13% of patients in the observation and treatment groups, respectively, showing progression at 5 years (p = 0.0018; Fig. 6.5). Indeed, cataract developed in 14% of the control group and 38% of the treatment group (p = 0.0011), which was attributable to the treatment patients who underwent glaucoma surgery.
Baseline Factors Associated with Progression
Female gender (adjusted risk ratio [RR] 1.85), history of migraine (adjusted RR 2.85), and baseline disc hemorrhage (adjusted RR 2.72) were positively associated with VF progression. Surprisingly, age and higher IOP were not predictive.
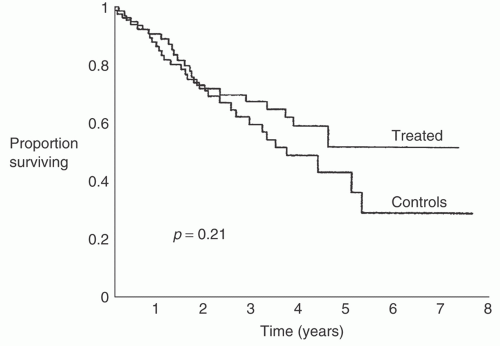 FIGURE 6.4 Survival curves of endpoints in untreated control subjects and treated patients from visual field baselines obtained at randomization using 4/5 defined endpoints. Reprinted with permission from Am J Ophthalmol. 1998;126:502. |
Clinical Implications
The CNTGS, like the EMGT, was an important study as it compared IOP reduction to no treatment in a group of patients with manifest glaucoma. The CNTGS conclusively demonstrated that there is an IOP-dependent component of disease progression in many patients with IOPs in the statistically “normal” range.
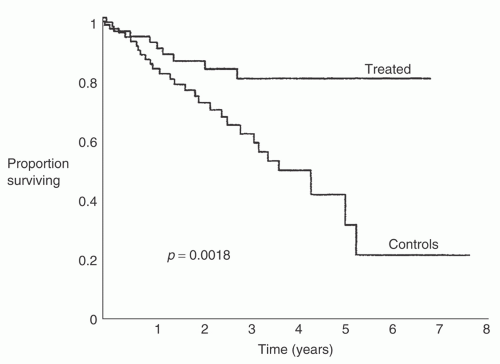 FIGURE 6.5 Survival curves of endpoints in untreated control subjects and treated patients from visual field baselines obtained at randomization using 4/5 defined endpoints with data on eyes developing cataracts, censored at the time of the diagnosis of the cataract. Reprinted with permission from Am J Ophthalmol. 1998;128:503. |
The findings of the CNTGS indicate that treating patients with normal-tension glaucoma to achieve an IOP reduction of 30% delays progression of disease, with an NNT of approximately 7 over a 5-year period. However, it is important to highlight that many patients in the observation arm of the CNTGS did not progress. Further, 85 of 230 patients (37%) initially assessed as having glaucomatous discs
and repeatable VF defects failed to show any change in VF and thus were never randomized. Hence, the NNT in standard clinical settings is, in reality, much higher. At the other end of the spectrum, several patients progressed in the treatment arm despite a 30% reduction in IOP, supporting the concept of IOP-independent mechanisms of disease progression in patients with normal-tension glaucoma. These findings highlight the importance of identifying patients at risk for progression to visual disability in order to tailor clinical management accordingly.
and repeatable VF defects failed to show any change in VF and thus were never randomized. Hence, the NNT in standard clinical settings is, in reality, much higher. At the other end of the spectrum, several patients progressed in the treatment arm despite a 30% reduction in IOP, supporting the concept of IOP-independent mechanisms of disease progression in patients with normal-tension glaucoma. These findings highlight the importance of identifying patients at risk for progression to visual disability in order to tailor clinical management accordingly.
Advanced Glaucoma Intervention Study
Results published 1998 to 2004
The AGIS was a multicenter, randomized, unmasked clinical trial, designed to determine the optimal steps in the management of patients with advanced glaucoma for whom medical therapy has failed. Specifically, the AGIS investigated whether ALT or trabeculectomy should be the next treatment in such patients. While the AGIS was designed to evaluate the optimal sequence of interventional treatment, the study is covered in this section as it ultimately provided important general information regarding the relationship between IOP control and VF deterioration in patients with advanced glaucoma.
Study Population
The target population for this study was patients with “advanced” OAG no longer controlled by maximal medical therapy.
Major Inclusion Criteria
Meeting the criteria for uncontrolled advanced OAG based on IOP, VF defect, and optic disc damage
Phakic status
Maximal medical therapy
VA ≥ 20/80
Major Exclusion Criteria
Secondary glaucoma
Previous laser (except iridotomy) or incisional surgery
Other eye pathology or VF defect not attributable to glaucoma
Sample Size and Baseline Characteristics
A total of 591 patients (789 eyes) were enrolled; 42% of the patients self-identified as white and 56% as black. The median age was 67 years, and the mean baseline IOP was 24.0 mmHg.
Intervention
Eyes were randomized to one of two treatment sequences:
TAT sequence: step 1—trabeculectomy; step 2—ALT (if trabeculectomy failed); step 3—trabeculectomy (if ALT failed)
ATT sequence: step 1—ALT; step 2— trabeculectomy (if ALT failed); step 3— trabeculectomy (if first trabeculectomy failed)
If both eyes of an individual were enrolled in the study, the first eye enrolled was randomized and the fellow eye assigned to the alternate treatment sequence. If eyes failed all three steps in their respective sequence, additional treatment was offered at the discretion of the treating clinician. Duration of follow-up was at least 4 years, with numerous analyses extending to longer periods.
Outcome Measures
The primary outcome assessed was visual function, including loss of VA or VF deterioration. VF defects were scored from 0 (no defect) to 20 (end stage) based on the number and depth of depressed test sites. Numerous AGIS publications report on additional outcomes including complications of surgery, cataract formation, bleb encapsulation, and filtration surgery failure.
Results
The AGIS reported primary results stratified by race. Overall, at the 10-year report, there was a trend toward more VF progression in the TAT sequence in the black subpopulation; however, this did not reach statistical significance. In contrast, the white subpopulation demonstrated greater VF loss with the ATT sequence, which became statistically significant at follow-up years 8 to 10. The proportion of eyes with decreased visual acuity was greater in the TAT sequence in both black
and white subpopulations in the early follow-up period but was not significantly different between the TAT and ATT groups from years 2 through 10.
and white subpopulations in the early follow-up period but was not significantly different between the TAT and ATT groups from years 2 through 10.
While the objective of AGIS was to compare different sequences of interventional surgical management in advanced glaucoma, the most often quoted and arguably the most sustainably useful data generated from this study relate to IOP control and its relationship to VF progression. AGIS addressed this relationship through two analyses. First, a predictive analysis investigated whether IOP level during early follow-up was predictive of subsequent VF deterioration over the next 7 years. A total of 738 patients were divided into three groups based on their average IOP during the first 18 months of follow-up, and rates of subsequent VF deterioration among each group were compared. Figure 6.6 demonstrates the results of this predictive analysis and shows a considerable difference in the rate of VF progression dependent on early IOP levels. Second, an associative analysis (Fig. 6.7) was designed to determine the effect of elevated IOP measurement frequency on VF progression. Specifically, 586 eyes were divided into four groups defined by the percent of visits with an IOP less than 18 mmHg, and the rates of VF progression were compared. A striking relationship between IOP control and VF stability
was demonstrated, with patients who had an IOP less than 18 mmHg at all visits (group A, mean IOP of 12.3 mmHg) showing no change in mean VF score.
was demonstrated, with patients who had an IOP less than 18 mmHg at all visits (group A, mean IOP of 12.3 mmHg) showing no change in mean VF score.
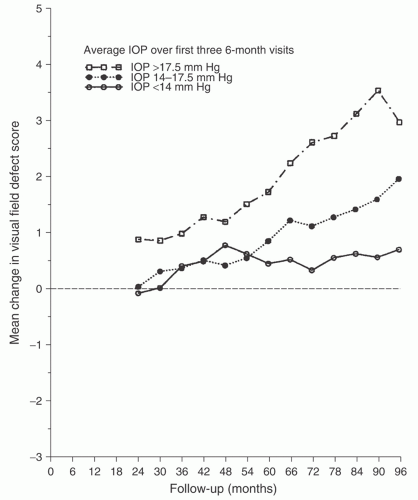 FIGURE 6.6 Predictive analysis. Mean change from baseline in visual field (VF) defect score by intraocular pressure classified according to average value over the first three 6-month visits. Reprinted with permission from Am J Ophthalmol. 2000;130:434. |
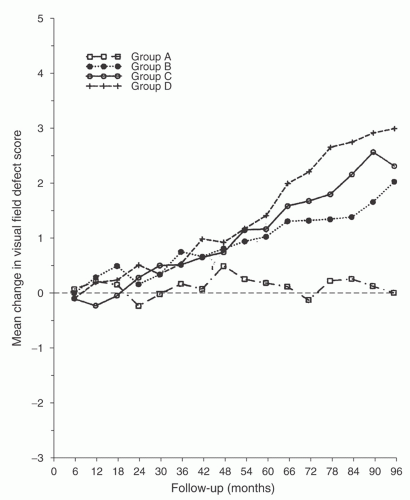 FIGURE 6.7 Associative analysis. Mean change in visual field (VF) defect score by percent of visits over 6 years at which an eye presented with intraocular pressure <18 mmHg (group A is 100%, group B is 75% to < 100%, group C is 50% to <75%, and group D is 0% to <50%.). Reprinted with permission from Am J Ophthalmol. 2000;130:437. |
The AGIS also showed that the rate of cataract development was higher in the TAT sequence than in the ATT sequence (56% and 47%, respectively). Additionally, younger age and higher preintervention IOP were risk factors for both ALT and trabeculectomy failure, while diabetes and postoperative complications were associated with trabeculectomy failure. Male gender was found to be a risk factor for bleb encapsulation.
Clinical Implications
Strengths of AGIS include its large size, long follow-up period, racially heterogeneous patient population, and numerous subgroup analyses. Criticisms of AGIS include the lack of well-defined endpoints for treatment failure as well as the changing use of antimetabolites in filtration surgery during the study period. The types of medications available at the time of AGIS were also much more limited than today, reducing the generalizability of some of the findings.
While AGIS provided some clinically applicable data regarding ALT and trabeculectomy outcomes, the associative and predictive analyses
of IOP control and VF progression have become instrumental in generating IOP targets in advanced glaucoma. Specifically, the associative analysis demonstrated that IOPs consistently below 18 mmHg stabilize the VF in many patients. This subgroup had an average IOP of 12.3 mmHg, which has resulted in many clinicians choosing 12 mmHg as a target in very advanced POAG. However, it is important to note that while there was no change in mean VF score in this subgroup as a whole, individually some patients showed VF deterioration (14.4% had worse VF defect score at 7 years) despite never having an IOP above 18 mmHg. The overall stability of this subgroup’s mean IOP score was due to a counter-balancing improvement in many patients’ VFs.
of IOP control and VF progression have become instrumental in generating IOP targets in advanced glaucoma. Specifically, the associative analysis demonstrated that IOPs consistently below 18 mmHg stabilize the VF in many patients. This subgroup had an average IOP of 12.3 mmHg, which has resulted in many clinicians choosing 12 mmHg as a target in very advanced POAG. However, it is important to note that while there was no change in mean VF score in this subgroup as a whole, individually some patients showed VF deterioration (14.4% had worse VF defect score at 7 years) despite never having an IOP above 18 mmHg. The overall stability of this subgroup’s mean IOP score was due to a counter-balancing improvement in many patients’ VFs.
II. MEDICAL MANAGEMENT OF GLAUCOMA
Overview
Despite the lack of recent breakthroughs, over the past two decades the medication options for lowering IOP have improved considerably. Modern topical hypotensive agents show greater IOP-lowering ability with improved side-effect profiles compared to older agents. The drug classes typically used in glaucoma practice include beta-blockers, alpha-agonists, carbonic anhydrase inhibitors, and prostaglandin analogs. There have been numerous clinical trials demonstrating the efficacy of these agents in lowering IOP—the surrogate outcome for most glaucoma medication clinical trials. Given the large number of agents and clinical trials in this area, this section presents important meta-analyses that synthesize some of these trials.
Intraocular Pressure Lowering Effects of All Commonly Used Drugs
Results published 2005
This meta-analysis reported on the IOP-lowering effects of the most commonly used glaucoma drugs, including beta-blockers, alpha-agonists, prostaglandin analogs, and carbonic anhydrase inhibitors, based on data from RCTs, primarily within populations of patients with POAG and ocular hypertension.36
Included Studies
A total of 28 eligible RCTs of sufficient quality were identified for inclusion in the meta-analysis.
Major Inclusion Criteria for Studies
RCTs (either comparison of two drugs or drug vs. placebo)
At least 85% of patients in study with POAG or ocular hypertension
IOP as the study’s primary endpoint
Outcome Measure
The outcome measure analyzed was the change in IOP from baseline to the 1-month follow-up visit. In studies where IOP at 1 month was not reported, the first measurement after 1 month was accepted up to a maximum of 6 months after drug initiation. Both peak and trough measurements were analyzed.
Clinical Implications
These results support the shift among many clinicians to utilizing prostaglandin analogs as first-line agents in medical monotherapy for POAG and ocular hypertension. However, the results underscore the efficacy of all of the listed drugs. Hence, an assessment of variables such as cost, likelihood of compliance, and side effects is also necessary in making rational therapeutic choices for individual patients.
Intraocular Pressure Lowering Effects of All Commonly Used Drugs in Normal-Tension Glaucoma
Results published 2009
This meta-analysis focused on RCTs evaluating commonly used glaucoma medications in the treatment of normal-tension glaucoma.37
TABLE 6.1 Relative Change in Intraocular Pressure in POAG and Ocular Hypertension | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


