General Posterior Segment Techniques
STRATEGIES
All surgery requires a strategy, game plan, or algorithm before being undertaken. The complexity of high-technology vitreoretinal surgery requires extensive preoperative planning. The surgical algorithm must include an expected series of events but must contain branches to allow for the contingencies and discoveries that occur in the course of surgery. The main branches of the algorithm are determined by the expected techniques, such as lens removal, endophotocoagulation, silicone oil, gas, scleral buckling, etc. Equipment, disposables, gas, oil, buckles, etc. must be available for any possible additional techniques driven by the individual case and any intraoperative findings or complications.
SPECULUM
A heavy wire speculum is an effective means of retracting the eyelids. Larger bladed specula that lift the lids may interfere with the contact lens and infusion cannula. The drape should not have a precut hole; it should be placed with the lids open and cut so the flaps completely cover both lid margins using the speculum to hold them in place. Covering the lashes and lid margins is done to reduce the chance of endophthalmitis and to prevent cilia from being entrapped in tissue. Aspirating speculums reduce fluid runoff under the drape or onto the foot pedals, surgeon’s feet, and floor but tend to be bulkier.
INFUSION FLUID
High-quality infusion fluid containing dextrose, glutathione, and a bicarbonate buffer should be used for all cases. This should be freshly prepared just prior to the operation. High-quality commercial solutions (Balanced Salt Solution, BSS Plus, Alcon Laboratories) should be utilized in all cases. Use of BSS Plus reduces corneal endothelial cell loss as well as trabecular meshwork and lens damage compared to other solutions. The authors do not add glucose, epinephrine, or antibiotics to the fluid to reduce the chances of using incorrect agents or concentrations as well as to reduce the risk of corneal, lens, and retinal toxicities. Plastic infusion fluid containers should be avoided because air diffuses through the plastic during storage, causing bubbles. Two-component infusate systems should be designed so that the substance in the actual infusion container is safe if the second component is inadvertently omitted, as is the case with BSS Plus.
IMPORTANCE OF VISUALIZATION
Optimal visualization is essential to safe vitrectomy. While it is obviously desirable to preserve the corneal epithelium and the lens, neither one is as important as the ability to perform a safe vitrectomy. This simple principle is often overlooked with adverse consequences.
Pupillary Dilation
The preoperative administration of topical adrenergic (phenylephedrine 2.5%-10%) and anticholinergic (tropicamide 1%, cyclopentolate 1%, hyoscine 0.25%, or homatropine 2.5%) dilating drops is critical to safe vitrectomy. Minimization of hypotony and mechanical iris trauma usually allow the preoperative dilation to be sustained throughout the case. If pupillary constriction occurs, a small pulse of intraocular epinephrine can redilate the pupil. This epinephrine should be labeled “for injection,” contain minimal amounts of sodium bisulfite antioxidant, and be diluted to 1:10,000 (1). Intracardiac injection preparations, although labeled as containing no preservative, contain too much sodium bisulfite and are potentially toxic to the corneal endothelium. Surgical pupillary sphincterotomies should be avoided unless the above steps fail and the fundus cannot be seen adequately for safe surgery. Iris surgery leads to postoperative glare, photophobia, and cosmetic problems, as well
as increased postoperative inflammation. Iris retractors and sutures cause iris trauma, inflammation, longer operating time, and increased cost and should only be used if there is no other option for surgical visualization. Contact wide-angle visualization systems with a trained assistant obviate the need for iris retractors, iris surgery, and intracameral epinephrine in almost all cases.
as increased postoperative inflammation. Iris retractors and sutures cause iris trauma, inflammation, longer operating time, and increased cost and should only be used if there is no other option for surgical visualization. Contact wide-angle visualization systems with a trained assistant obviate the need for iris retractors, iris surgery, and intracameral epinephrine in almost all cases.
Lens Removal
If lens removal is necessary, phaco or lensectomy should be performed before proceeding with vitrectomy, unless the lens is subluxated or dislocated. Relative miosis may occur as the vitrectomy progresses, and early lens removal permits better access to the periphery and prevents unnecessary iris surgery. The view is always better in aphakic or pseudophakic eyes, and safe, effective vitrectomy should never be compromised to preserve the lens, even if it is relatively clear. Saving the anterior lens capsule until the end of the operation in lensectomy cases hinders the view and offers no significant advantages. Forceps removal of the lens capsule in lensectomy cases facilitates total capsule removal without iris touch and resultant miosis and inflammation.
Wound Construction Issues for Microincisional Vitrectomy Surgery
A transconjunctival, sutureless vitrectomy technique was introduced by Eugene de Juan, to reduce pain, inflammation, and operating time, although from the outset, concern regarding hypotony and endophthalmitis was expressed with this technique, as with sutureless, small-incision cataract surgery (2). de Juan recommends leaving vitreous in the wound to reduce the incidence of wound leaks, but the authors disagree with this approach because leaving vitreous in the sclerotomies increases the likelihood of vitreous wick (and therefore increases the likelihood of endophthalmitis) and increases the likelihood of subsequent hypocellular contraction of the collagen fibers and retinal breaks immediately posterior to the sclerotomies (3). In the authors’ opinion, vitreous wicks are more likely to be a factor in endophthalmitis than hypotony with retrograde flow of tear film into the eye.
Angulated Wound Construction
Although the authors initially used straight-in wound construction for 25-gauge vitrectomy, they changed to angulated wound construction after the technique was introduced for 23-gauge vitrectomy. The purpose of angulated wound construction is to create a scleral tunnel that functions as a flap valve, similar to no-stitch cataract surgery incision. It is not, however, considered a biplanar wound; the change in trocar insertion angle is to avoid intraocular contact. The wound already has been made at the point of trocar insertion. Some surgeons call the uptilt in insertion angle supination, which is incorrect. A single plane, 15 degree incision produces the best scleral tunnel and is less likely to result in an inadvertent suprachoroidal infusion than a flatter (5 degree) itrajectory.
Stabilization of the Eye
Traditionally, surgeons have attempted to stabilize the eye to offset translational and rotational forces acting on the eye during trocar-cannula insertion. An alternative approach is to allow the eye to move deeper into the orbit but prevent eye rotation by rigidly enforcing the correct geometric relationship between the trocar and the eye (4). Using the forefinger on the surgeon’s hand to triangulate the trocar support on the insertion hand facilitates better control of hand and trocar attitude. Some surgeons have described this technique as pressing down on the eye; while this is true, the key point is to maintain the correct insertion angle and direction by continuously modifying the handle angle while allowing the eye to freely move. Initially, this hand holds the cotton-tip applicator used to displace the conjunctiva, but the cotton-tip applicator is dropped after the trocar impales the conjunctiva against the sclera, maintaining the displaced position. Incidentally, the authors use the same two-handed approach when performing intravitreal injections and retrobulbar blocks.
The surgeon should allow a large service loop before adhesively fastening the infusion line to the drape to avoid traction and inadvertent suprachoroidal infusion or cannula pullout during ocular rotation. Unless a filtering bleb or other conjunctival conditions prevent this approach, the sclerotomies should be placed to facilitate the greatest possible angular intraocular access.
The infusion cannula port is traditionally placed inferotemporally near the lower border of the lateral rectus, but it is better to move it closer to the 3 o’clock or 9 o’clock position to avoid contact with the lower lid. The superonasal sclerotomy should be placed on a virtual line from the lowest point of the bridge of the nose to the center of the pupil, facilitating better angular movement. Similarly, the superotemporal incision should be placed on a virtual line extending from the lowest point of the supraorbital rim to the center of the pupil. The position of the 25-gauge cannulas may require modification in the presence of a filtering bleb, an area of previous trauma with a sclera wound, or if there is underlying choroidal effusion or hemorrhage.
The authors initially made the sclerotomies 3.5 mm posterior to the limbus but have found that moving them to 4.0 mm posterior to the limbus reduces the chance of air in the anterior chamber of phakic or pseudophakic eyes during fluid-air exchange (FAX).
Conjunctival Displacement
The concept of conjunctival displacement for sutureless, 25-gauge surgery was developed by de Juan; some surgeons using 23-gauge systems have abandoned conjunctival
displacement (in the authors’ opinion, unwisely) because various techniques to stabilize the globe made displacement difficult. Tornambe Torpedoes (Insight Instruments, Stuart, Florida) and other chandelier systems are inserted without conjunctival displacement, which removes vitreous at the site, or without angulated wound construction; both a lack of conjunctival displacement or failure to perform angulated wound construction increases the likelihood of endophthalmitis (5).
displacement (in the authors’ opinion, unwisely) because various techniques to stabilize the globe made displacement difficult. Tornambe Torpedoes (Insight Instruments, Stuart, Florida) and other chandelier systems are inserted without conjunctival displacement, which removes vitreous at the site, or without angulated wound construction; both a lack of conjunctival displacement or failure to perform angulated wound construction increases the likelihood of endophthalmitis (5).
Reduction of Wound Leaks
The senior author first reported the use of FAX to reduce wound leaks after 25-gauge straight-in wound construction, but with the adoption of scleral tunnel wound construction, the author currently utilizes the FAX technique to reduce wound leaks only in patients with a high degree of myopia or Marfan syndrome or in other patients with thin sclera.
Logically, wounds made during 20-gauge (0.89-mm tools) and 23-gauge (0.75-mm tools) surgeries are significantly larger than wounds made during 25-gauge (0.5-mm tools) surgery, increasing the likelihood of wound leaks and making wound construction more challenging. Tools used in 23-gauge surgery were developed to address tool stiffness and flow restriction issues associated with the first-generation 25-gauge tools (6). Subsequent generations of 25-gauge tools have increased tool stiffness and reduced flow restriction; therefore, the authors do not see an advantage of 23-gauge surgery.
When withdrawing the cannulas at the end of a case, the surgeon should take care to avoid wound eversion. Cannulas should be withdrawn slowly on the same trajectory as they were inserted, because the sclera is relatively inelastic and the goal is to close the scleral tunnel. Scleral tunnel closure is also dependent on leaving the infusion set at least 25 mm Hg, which will cause the intraocular pressure (IOP) to press on the inside of the wound. The surgeon should use point pressure with smooth forceps, not a cotton-tip applicator, on the scleral tunnel to press on the outside of the tunnel, similarly to how pressure is placed when withdrawing a needle or IV line from the antecubital vein. The conjunctiva should be repositioned while point pressure is applied on the tunnel. Some surgeons withdraw the cannulas over the endoilluminator. Withdrawing on the insertion trajectory, leaving the infusion turned on, and point pressure on the tunnel are far more important in achieving tunnel closure, though.
If the wounds leak, then they should be sutured without hesitation with a single, transconjunctival absorbable polyglycolic suture such as 8-0. PolySorb. PolySorb has been associated with less irritation than polyglactin (Vicryl, Novartis, Basel, Switzerland) (7). It is not necessary to open the conjunctiva to suture the sclerotomy. Some surgeons unwisely use sutured-on contact lens support rings, which can damage the conjunctiva (8).
Transconjunctival 23-gauge and 25-gauge, sutureless vitrectomies allow flexibility in cannula location. The surgeon should avoid filtering blebs, previous conjunctival wounds, areas of pars plana scarring, high choroidals, or suprachoroidal hemorrhage to ensure that the cannula extends into the vitreous cavity and not in the suprachoroidal space. If required, contiguous placement of all cannulas on the same hemisphere or quadrant can be performed. Additionally, the infusion port with some vitrectomy systems (Accurus and Constellation Vision System, Alcon, Fort Worth, Texas) can be moved from one cannula to another to facilitate tool access to pathology.
Several early studies demonstrate an apparent increase in endophthalmitis rates after 23-gauge and 25-gauge surgeries. The Wills study has been widely quoted, but the surgeons involved in the study now believe that the factors resulting in the apparent increase in endophthalmitis are no longer significant (9,10). Although hypotony is considered a factor for endophthalmitis, the author believes that vitreous wicks and omission of subconjunctival antibiotics are more important issues and are bigger risk factors for the development of endophthalmitis. Some vitreoretinal surgeons stopped using subconjunctival antibiotics after cataract surgeons abandoned the practice; however, topical antibiotics achieve minimum inhibitory concentration antibiotic levels in the anterior chamber but not in the vitreous cavity of phakic or pseudophakic eyes. Harry W. Flynn, as well as the author, recommend using both an antibiotic effective against common Gram-positive organisms and one effective against virulent Gram-negative organisms. The authors prefer administering 20 mg tobramycin subconjunctivally and ceftazidime 50 mg; vancomycin 25 mg is a good alternative to ceftazidime if the patient is allergic to penicillin. Injection in the inferior cul-de-sac may help the surgeon avoid reflux of the aminoglycoside into the eye and, therefore, the possibility of retinal toxicity.
VITRECTOMY OBJECTIVES
Vitreous removal requires a thorough understanding of surgical anatomy and must proceed in a systematic fashion. The vitreous body should be thought of in terms of discrete surfaces that are removed in a specific order. The goals should not be band cutting, obtaining a view on the posterior pole, or core vitrectomy only but should be directed at management of the underlying vitreoretinal process. When vitrectomy was performed using rotating cutters with syringe-controlled suction, the surgeon was able to remove much of the vitreous without moving the instrument from the center of the vitreous cavity. This occurred because of excessive suction and cutter winding, which drew the vitreous inward; however, such traction is now recognized to be dangerous. From this traction-induced central relocation of the vitreous arose the erroneous concept of “core vitrectomy.” In fact, many eyes with sufficient vitreoretinal disease to require vitrectomy do not even have a vitreous “core.” Recent trauma, rarely recent retinal detachments, and macular hole cases may have relatively normal vitreous requiring core vitrectomy.
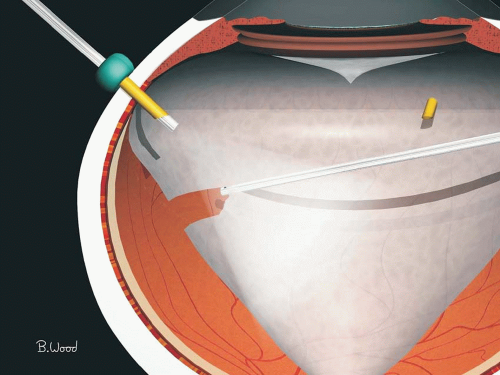 Figure 6.1 ▪ Penetration through the opaque PVC should be made nasally or into an area known to have PVD and no detachment if possible as determined by ultrasound or ophthalmoscopy. |
Better cutters, high cutting rates, fast fluidic controllers, and proportional (linear) suction control facilitate cutting the vitreous without moving it from its original position. The surgeon accustomed to low-performance systems may at first be confused by the better systems’ minimal pulsatile traction and may falsely conclude that they are not working.
If the eye is aphakic at the commencement of vitrectomy, the anterior vitreous cortex (AVC) should be removed first, starting centrally and progressing peripherally. Any attachments to anterior segment wounds or the iris should be removed before proceeding posteriorly. In phakic eyes, the AVC is frequently adherent to the posterior lens capsule, making removal difficult without lens damage. A clear AVC not causing traction should be avoided in eyes without retinal detachment to reduce lens damage. Similarly, the AVC should be retained in pseudophakic eyes to reduce the chances of fogging due to condensation on the intraocular lens (IOL) in eyes that have had a YAG capsulotomy.
Pars plana infusion cannulas permit the surgeon to change sides between the vitrectomy instrument and the endoilluminator, thereby gaining access to the whole posterior curve of the lens. Removal of the AVC in a phakic eye requires direct microscope viewing and coaxial plus endoillumination without a contact or wide-angle system to avoid lens damage. A combined nasal and temporal approach is best for AVC removal in phakic eyes. Eyes with fibrovascular proliferation on or near the pars plana or a significant inflammatory component should have lensectomy with forceps capsule removal as a precaution against the formation of a cyclitic membrane at the lens-AVC interface.
After removal of the AVC, the second objective is usually the removal of the posterior vitreous cortex (PVC). Eyes requiring trans-pars plana vitrectomy usually have total vitreoretinal contact, partial posterior vitreous detachment (PVD) with a conical vitreous configuration, or total PVD with a frontal plane configuration. Entry into the PVC should be made in an area nasally (Fig. 6.1) or preferably known to have a PVD by ophthalmoscopy or ultrasound. The portions of PVC extending between areas of vitreoretinal adherence are known as bridging and are areas where tangential traction occurs. All portions of the PVC not in contact with the retina, that is, both the conical surface and the bridging portions, must be removed to relieve traction. However, the vitreous “skirt,” which is the anterior edge of the truncated cone, must be treated differently. Because retinal breaks can be caused by surgically induced traction on the skirt, only enough skirt should be removed to allow satisfactory surgical visualization and to prevent the superior skirt from covering any portion of the view when the patient is upright. If blood products are incorporated in the layers of the skirt, they should be carefully debulked to diminish postoperative hemolytic and erythroclastic glaucoma.
EPIRETINAL MEMBRANES
The PVC may include new collagen and glial cells on its surface at sites of vitreoretinal adherence in addition to hypocellular contraction of preexisting vitreous collagen. This type of pathoanatomy is usually referred to as an epiretinal membrane (ERM). The treatment of ERM is a challenging and essential component of management or vitreoretinal cases. The approach to ERM varies with the disease; specific techniques will be discussed with the specific diseases.
Forceps membrane peeling, scissors segmentation, and scissors delamination are all useful approaches to ERM. The goal of ERM surgery is to reattach the retina while minimizing recurrences and complications. If the membrane is loosely adherent and can be removed without iatrogenic retinal breaks or bleeding, forceps membrane peeling is the best approach. In diabetes, retinopathy of prematurity (ROP), and some trauma and proliferative vitreoretinopathy (PVR) cases, the membrane is usually quite adherent, requiring scissors segmentation and/or delamination. Excellent visualization is necessary for ERM dissection.
Simplified Epiretinal Membrane Dissection
Current approaches to vitreoretinal surgery utilize a wide variety of techniques and technologies. The techniques for PVR, proliferative diabetic retinopathy (PDR), ROP, epimacular membranes (EMMs), macular holes, and other causes of vitreoretinal traction typically vary considerably with the disease process. Fibrin syndrome, corneal problems, cataract, light toxicity, postanesthesia complications, postoperative pain, lid and conjunctival hyperemia, and edema are more frequent after longer procedures. Postoperative atelectasis, infection, pulmonary embolism, and increased length of stay have been associated with longer operating times in the surgical literature. The principal author has observed a relationship between number of tools used, longer operating times, and worse surgical outcomes. A unified, all-disease approach to tools, techniques, and algorithms could theoretically reduce costs associated with longer operating times, staff training time, setup time, and instrument acquisition and maintenance. Advancements in manufacturing technology generally decrease the cost while increasing the quality of the product by reducing the number of steps or processes. A central theme of this book is to present a simplified, faster, less-step, less-tool approach to vitreoretinal surgery.
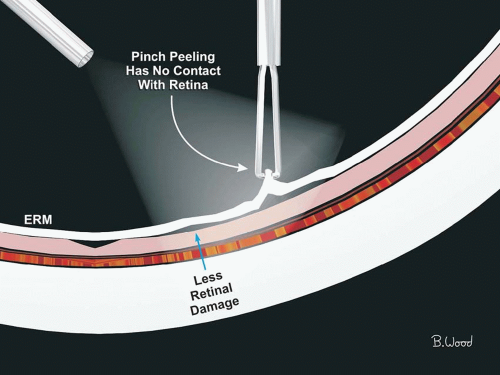 Figure 6.2 ▪ Membrane peeling with end-grasping forceps does not require entering into the potential space between the retina and the membrane or finding an edge; therefore, it is much less likely to damage the retina than a pic or an approach using a forceps blade under the retina. |
At present, the authors use end-grasping forceps for all epiretinal and subretinal membrane peeling and fine curved scissors for all segmentation and delamination. Pics and bent needles are not needed for EMM dissection and increase the potential for retinal trauma. End-grasping forceps and curved scissors are the only dissection tools used by the authors for virtually all vitreoretinal surgery. The following section describes a unified approach to tool and technique selection for vitreoretinal surgery that was developed for use by novice and advanced surgeons alike.
Management of Epiretinal Membranes
Membrane Peeling
Robert Machemer, developed ERM peeling only 2 years after he developed pars plana vitrectomy. He used a bent 23-gauge needle to peel macular puckers, which we now call EMMs. His technique, although effective, required a sharp needle tip adjacent to the retina surface. Conor O’Malley, soon thereafter introduced the pic—a rounded tip instrument, safer for membrane peeling. The principal author developed forceps membrane peeling using end-grasping forceps and a pinch peeling, en face technique because membranes slip off the needles and pics and because forceps were still required to remove the membrane from the eye. A single-step, end-grasping forceps membrane peeling approach is safer and faster than initiating peeling with a blade, pic, or membrane scraper and subsequently removing the ERM with forceps (Fig. 6.2). End-grasping forceps are
used with both blades on the anterior surface of the ERM, a safer approach than attempting to place one blade under the membrane risking retinal damage similar to peeling with needles, microvitreoretinal (MVR) blades, or pics. Using pics or MVR blades requires finding or constructing an “edge,” which is a potentially dangerous maneuver. Finding the outer perimeter of an ERM can be difficult with thin, so-called “glassy,” membranes; retinal surface damage can result from using this approach. Making an edge involves using an MVR blade to slice through the ERM, a potentially dangerous maneuver if the patient moves or the visualization is not optimal. The senior author developed the MVR blade and was an early adopter of pics but has used only end-grasping forceps membrane peeling for more than three decades. An end-grasping forceps technique requires perfect alignment of the forceps blades at the tip, which cannot be maintained with blades with long axial gripping surfaces, particularly with multiple cleaning and sterilization cycles for reusable tools or, worse yet, reuse of disposable forceps. Smaller 23-gauge and 25-gauge forceps are more vulnerable to damage during cleaning and sterilization; the authors use disposable 25-gauge Grieshaber Revolution DSP ILM (Alcon, Ft. Worth, Texas) forceps for all ERMs, PVR membranes, and internal limiting membrane (ILM) peeling without pics or MVR blades. The senior author developed conformal forceps so that the blade tips would have the same radius of curvature as the retinal surface in contrast to the Eckardt forceps (Dutch Ophthalmic USA, Exeter, New Hampshire) that have sharp corners that tend to grasp retina. The DSP ILM forceps are small enough that the radius of curvature is not a significant issue.
used with both blades on the anterior surface of the ERM, a safer approach than attempting to place one blade under the membrane risking retinal damage similar to peeling with needles, microvitreoretinal (MVR) blades, or pics. Using pics or MVR blades requires finding or constructing an “edge,” which is a potentially dangerous maneuver. Finding the outer perimeter of an ERM can be difficult with thin, so-called “glassy,” membranes; retinal surface damage can result from using this approach. Making an edge involves using an MVR blade to slice through the ERM, a potentially dangerous maneuver if the patient moves or the visualization is not optimal. The senior author developed the MVR blade and was an early adopter of pics but has used only end-grasping forceps membrane peeling for more than three decades. An end-grasping forceps technique requires perfect alignment of the forceps blades at the tip, which cannot be maintained with blades with long axial gripping surfaces, particularly with multiple cleaning and sterilization cycles for reusable tools or, worse yet, reuse of disposable forceps. Smaller 23-gauge and 25-gauge forceps are more vulnerable to damage during cleaning and sterilization; the authors use disposable 25-gauge Grieshaber Revolution DSP ILM (Alcon, Ft. Worth, Texas) forceps for all ERMs, PVR membranes, and internal limiting membrane (ILM) peeling without pics or MVR blades. The senior author developed conformal forceps so that the blade tips would have the same radius of curvature as the retinal surface in contrast to the Eckardt forceps (Dutch Ophthalmic USA, Exeter, New Hampshire) that have sharp corners that tend to grasp retina. The DSP ILM forceps are small enough that the radius of curvature is not a significant issue.
Yasuo Tano, MD, developed the diamond-dusted membrane scraper, which some surgeons have adopted. The authors prefer the end-grasping forceps technique because it is less likely to damage the retinal surface, especially in smaller 23-gauge and 25-gauge form factors that produce greater force per unit area.
Internal Limiting Membrane Peeling
ILM peeling was introduced for macular hole surgery and has been widely accepted; it is generally agreed that it improves closure rates. A few papers suggested that ILM produced worse visual outcome despite hole closure; the authors believe that this is due to indocyanine green (ICG) toxicity, not ILM peeling. The standard justification for ILM peeling is to remove “tangential traction.” Successful ILM peeling guarantees removal of vitreomacular traction, residual PVC not contiguous with the detached vitreous, and any ERM that might be present. The principal author believes that an additional and critical role for ILM peeling is increasing retinal compliance by approximately 50% so that the inward-directed surface tension force from a gas bubble can almost immediately reapproximate the inner margins of the hole.
Anslem Kampnik, MD, has emphasized that ILM peeling in EMM surgery produces a reduction in recurrence rates. The authors have been following his recommendations by peeling ILM in all EMM cases for several years; they agree with his observation and believe that an additional benefit is the elimination of residual striae, thereby producing better visual outcomes and faster improvement.
Staining and Particulate Marking
Many surgeons still use ICG staining of the ILM, although its use is decreasing. The authors have never used ICG because of concerns about the toxicity of the agent and vehicle and because it is simply unnecessary. One factor driving dangerous and unnecessary ICG use is using noncontact optical systems such as the BIOM and EIBOS systems that decrease both axial and lateral resolutions. An additional factor driving ICG use is using inadequate forceps that are incapable of end grasping.
Triamcinolone particulate marking, often incorrectly referred to as staining, is not specific to ILM or ERMs. The optimal use for triamcinolone is for visualizing the vitreous. Triamcinolone is more often required with a Tornambe Torpedo (Alcon) or a chandelier illumination system that produces diffuse illumination, making visualization of the vitreous, ILM, and ERMs difficult. Triamcinolone is useful when learning vitrectomy and for the identification of the PVC anatomy in complex cases.
Scissors Segmentation and Delamination
The principal author developed scissors segmentation of ERMs more than three decades ago to address the issue of iatrogenic retinal tears caused when attempting to peel adherent ERMs, which are common in diabetic traction retinal detachment cases. Segmentation is used to reduce tangential force on the retina by separating an ERM into “epicenters,” (Fig. 6.3) better termed vascularized adherence sites. Segmentation is performed by placing one blade of the scissors under the ERM, between the retina and the ERM, and the other blade above the ERM. Although this was initially performed with “vertical scissors,” curved scissors are far superior for segmentation. Because blade width is much greater than blade thickness, vertical scissors require more space between the retina and the ERM than curved scissors (Fig. 6.4). Segmentation is now primarily used for access segmentation to expose the delamination plane. Using curved scissors expedites transitioning from access segmentation to delamination without tool exchange.
The principal author developed scissors delamination 2 years after developing segmentation to address the issue of residual ERM after segmentation. Residual ERMs in diabetic traction retinal detachment cases resulted in small areas of chronic retinal elevation that ultimately caused atrophic retinal holes and late rhegmatogenous retinal detachments.
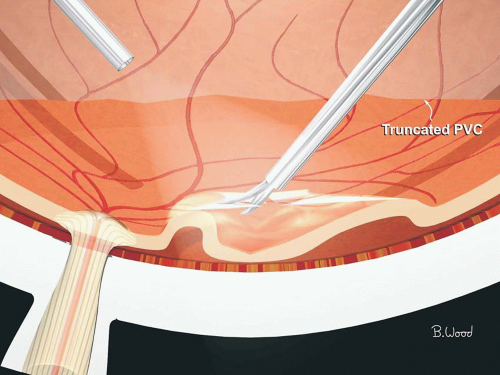 Figure 6.3 ▪ Scissors segmentation of ERMs reduces tangential traction but leaves epicenters, which may bleed on the cut edges. The blood acts as a substrate for glial recurrence. Residual ERM may cause residual elevation and late retinal detachment from atrophic holes. Segmentation is used when the membrane is too adherent to peel and the retina too thin for delamination. |
Scissors delamination is performed by inserting both scissors blades in the potential space between the ERM and the retina and severing the attachment points (Fig. 6.5). Simplistically, segmentation means to cut up the ERM, and delamination means to cut it off. Initially, delamination was performed with “horizontal” scissors, actually 135 degrees. For almost two decades, the senior author has used only curved scissors for conformal delamination. Curved scissors are preferred to “horizontal” scissors because the curvature of the scissors matches the curvature of the retina, reducing the likelihood of impaling the retina with scissors tips. The same design concept is used for skis—the tips curve up. If the scissors are introduced under the ERM with the blades wide open and then closed, attachment points will be ripped instead of sheared,
which causes retinal breaks (Fig. 6.6). When the scissors are introduced under the ERM with the blades closed and then opened similar to the technique used for blunt dissection in general surgery, attachment points will be ripped instead of sheared, creating retinal breaks. The optimal technique is to open the scissors just enough to engage an attachment point, cut, pull back slightly, move laterally to the next attachment point, advance slightly, and cut again (Fig. 6.7). It is not necessary to lift or stabilize the ERM when disposable scissors or reasonably new reusable scissors are used. Because an ERM is taut and there is a pressure gradient across the retina, the ERM will scroll up and separate from the retina without lifting.
which causes retinal breaks (Fig. 6.6). When the scissors are introduced under the ERM with the blades closed and then opened similar to the technique used for blunt dissection in general surgery, attachment points will be ripped instead of sheared, creating retinal breaks. The optimal technique is to open the scissors just enough to engage an attachment point, cut, pull back slightly, move laterally to the next attachment point, advance slightly, and cut again (Fig. 6.7). It is not necessary to lift or stabilize the ERM when disposable scissors or reasonably new reusable scissors are used. Because an ERM is taut and there is a pressure gradient across the retina, the ERM will scroll up and separate from the retina without lifting.
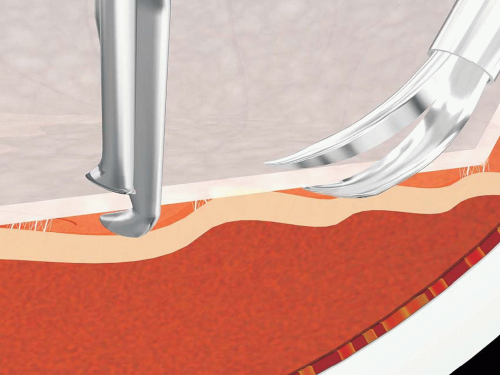 Figure 6.4 ▪ Fine curved scissors are better than vertical scissors for segmentation because blade width is greater than blade thickness and the curve is conformal with retinal contour, reducing iatrogenic retinal breaks. |
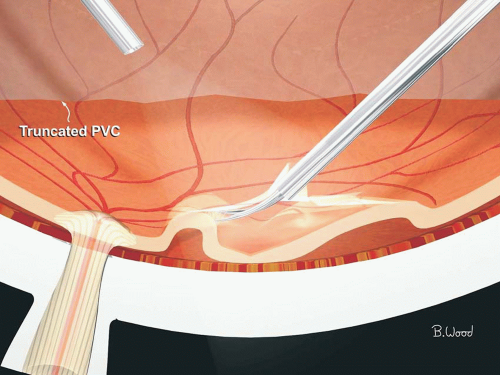 Figure 6.5 ▪ Scissors delamination of ERMs is the preferred method of removing adherent membranes as it permits complete removal of ERM. |
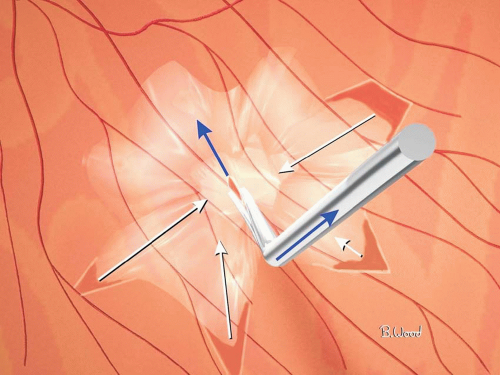 Figure 6.6 ▪ The shear point of scissors moves forward as the scissors close, creating an exclusion force that can tear the retina. |
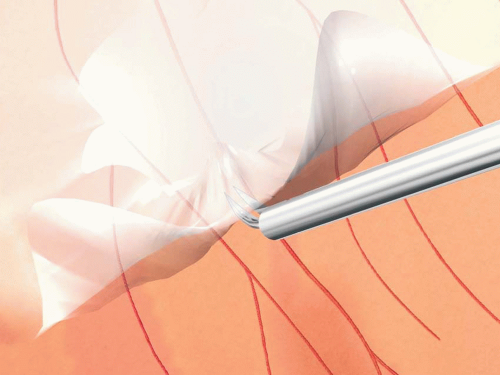 Figure 6.7 ▪ The scissors are moved back and forth while making small cuts with the tips barely opening; the ERM will scroll up because of inherent elasticity, rarely requiring lifting. |
Inside-Out Versus Outside-In Technique
Robert Machemer, used an outside-in technique for bent needle membrane peeling, and many surgeons emulate this technique when using delamination. A better approach for end-grasping forceps membrane peeling, scissors segmentation, and scissors delamination is to initiate the dissection centrally and peel, segment, or delaminate outward. Inside-out dissection is safer because the retina is thicker and 100 times stronger centrally than in the periphery, especially in ischemic patients and postpanretinal photocoagulation; the retina is redundant centrally in traction retinal detachment cases, and the view is better centrally.
En Bloc Dissection
En bloc dissection, as initially described, utilized an outside-in technique and advocated using the PVC to lift the ERM. Putting traction on the PVC results in peripheral retina breaks while the surgeon is focusing on the ERM dissection. En bloc is a poor term when applied to ERM dissection; it is only meaningful in cancer surgery where the notion is to minimize the dispersion of cancer cells. A better way to think about this issue is to forget the outdated notion that the standard surgical algorithm is first performing core vitrectomy, then creating a PVD, and finally dissecting ERMs. If a posterior vitreous separation PVD is not present in a diabetic traction retinal detachment (TRD) case, proceed directly to an inside-out delamination starting at or near the optic nerve head. It is not necessary to remove all ERM in one piece as suggested by the term en bloc; it is preferable to segment in several pieces, each of which will be contiguous with the PVC. When most or all the ERM has been delaminated using an inside-out direction, creation of PVD will be accomplished as well or it will be irrelevant because there are no longer any posterior attachment points.
Bimanual Surgery
Bimanual surgery is a poor term; surgeons have always used both hands. The point of bimanual surgery is to accomplish what the author calls “forceps stabilization of epiretinal membranes,” using forceps to offset the scissors push-out force (Fig. 6.8). Scissors cut at a point that starts near the pivot point and moves toward the tip, creating undesirable push-out force. By contrast, a vitreous cutter cuts on a curved line, which makes manufacturing much more difficult and requires vacuum for imbrications into the port but eliminates push-out force. An unintended consequence of bimanual surgery is to inadvertently lift the ERM, thereby creating iatrogenic retinal breaks. Making small delamination cuts with scissors almost closed obviates the need to lift the ERM and visualize the attachment points. Bimanual surgery requires the use of either illuminated tools, which are not available in 23-gauge or 25-gauge systems, or a chandelier or Torpedo, which produces diffuse illumination, making visualization of vitreous, ILM, and transparent membranes more difficult.
Viscodissection
Viscodissection is performed by injecting a viscoelastic in the potential space between the ERM and the retina. Viscodissection is seldom performed because it has not been shown
to be advantageous and it increases cost and operating time. Viscodissection pressurizes the potential space between the ERM and the retina, which can result in a hydraulic retinal break if the ERM is tightly adherent. If the ERM is adherent with no gap between the ERM and the retina, the viscocannula may create a retinal break during introduction. Viscoelastic substances significantly decrease the interfacial tension of silicone oil, increasing the likelihood of emulsification. It is virtually impossible to remove the viscoelastic; the viscous material potentially increases glial recurrence rates by retaining cells, fibronectin, and cytokines such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and transforming growth factor beta.
to be advantageous and it increases cost and operating time. Viscodissection pressurizes the potential space between the ERM and the retina, which can result in a hydraulic retinal break if the ERM is tightly adherent. If the ERM is adherent with no gap between the ERM and the retina, the viscocannula may create a retinal break during introduction. Viscoelastic substances significantly decrease the interfacial tension of silicone oil, increasing the likelihood of emulsification. It is virtually impossible to remove the viscoelastic; the viscous material potentially increases glial recurrence rates by retaining cells, fibronectin, and cytokines such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and transforming growth factor beta.
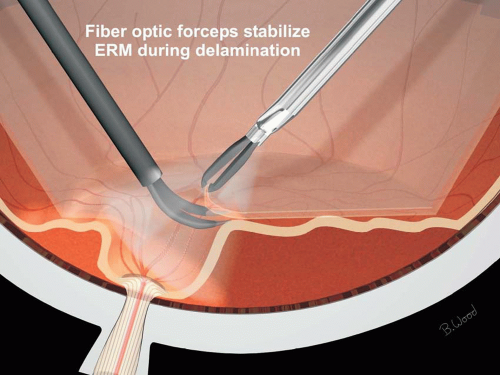 Figure 6.8 ▪ Illuminated forceps allow stabilization of the ERM to offset peeling, segmentation, or delamination forces. |
Power Scissors and Forceps
Power scissors and power forceps address the problem of inadvertent motion of the tool tip during manual actuation. A potentially offsetting issue is inadvertent hand motion due to whole leg motion while moving the foot pedal. Older generation power scissors and power forceps were too heavy and did not have high-fidelity proportional control; the Constellation (Alcon) power scissors and forceps have solved these design issues and also have a single foot pedal control mode for bimanual surgery.
Hemostasis
Endolaser is better than diathermy for treating the severed vessel ends of attachment points after delaminating ERMs in diabetic traction retinal detachment surgery. The authors believe that using excessive diathermy on retinal surface bleeders can result in subclinical retinal necrosis and late atrophic holes. On occasion, larger vessels may require diathermy before or after transection, especially in delayed trauma surgery and when performing retinectomy.
Stabilized Surgery
Retinal movement in response to fluidic or mechanical dissection forces is often an indication that retinal tearing may be imminent. Ideal vitreous and ERM removal would not cause any force on the retina but is impossible as described above. Many techniques have been developed that, although promoted for a variety of reasons, primarily function by reducing surgically induced retinal motion: (a) flow limiting using high cutting rates and 25-gauge fluidics, (b) forceps stabilization of ERM (bimanual surgery), (c) perfluorocarbon liquids used during ERM dissection, and (d) viscodissection.
Perfluorooctane has twice the specific gravity of balanced salt solution. Therefore, it produces twice the gravitational force on the retina (11).
In addition, inertial stabilization, because of the F = MA relationship, offsets pulsating fluidic forces. Perfluorocarbon liquids are immiscible in balanced salt solution, blood, and subretinal fluid (SRF) and are therefore used because of surface tension properties (interfacial tension) to unfold giant breaks and remove SRF in all types of retinal detachments (Fig. 6.9). The interfacial tension effect also prevents transretinal fluid flow (uveal-scleral outflow) and tends to reduce retinal edema while the perfluoron (PFO) is present.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


