Cough is a common and troublesome symptom that can be difficult to treat. New therapeutic options that are safe and more effective than those currently available are needed. In this article, the authors offer opinion on future directions in the treatment of cough, with a particular emphasis on the clinical syndrome associated with cough reflex hypersensitivity. In addition, the article provides an overview of some of the diagnostic technologies and promising drug targets likely to emerge from current clinical and scientific endeavor.
Over the last four decades, considerable advances in basic and applied science have improved the understanding of the physiology and pathophysiology of cough. During this time, there also have been advances in the clinical management of cough with the development of systematic and protocol-based algorithms for diagnosing and treating cough. This approach has formed the basis of current management guidelines for both adult and pediatric patients with cough. In recent years, however, there has been a sense that progress has slowed with debate over the strength of the evidence base for current treatment recommendations, the withdrawal of some established therapies following safety concerns, and the recognition in both primary and secondary care of greater proportions of symptomatic patients with idiopathic or unexplained cough. Such pessimism, however, seems misplaced given the number of developments over this time in diagnostic and experimental techniques relevant to cough. This article provides the authors’ opinion on the future direction of the treatment of cough. The authors suggest that this requires a refinement of existing management protocols and fresh thinking on the clinical syndrome of cough with more emphasis on the common triggers and aggravating factors. Therefore, this article focuses on two main areas: the optimization of existing recommendations for the management of cough and the clinical features and consequences of cough reflex hypersensitivity associated with common acute and chronic cough syndromes. Throughout this article, to the authors highlight important gaps in knowledge and identify areas where advances may be made to improve the treatment of cough in the future.
Acute and chronic cough—the extent of the problem
The exact prevalence of cough in the general population is difficult to quantify with certainty, but depending on the population surveyed and the tools used, reported figures range from 3.3% to 33%. Cough remains the most common reason for which patients seek medical advice, with an estimated 84 million consultations in the United States during 1 year alone. Cough associated with the common cold is usually self-limiting, but many individuals self-medicate, as reflected in the considerable expenditure on over-the-counter (OTC) preparations. In 2008, a total of £102.9 million was spent in the United Kingdom on cough syrups alone, and in the United States, the figure for OTC cold remedies has been estimated in the range of $3 billion. The social and financial burden of cough may be even greater if school and work absenteeism associated with the common cold (estimated at between 40 and 100 million absences per year) are considered. A more complete review of the worldwide problem of cough is covered elsewhere in this series.
Optimizing the existing protocols for the management of cough
Several consensus statements have been produced to help physicians assess and treat patients with cough. In general, the recommended approach in both adult and pediatric settings is to undertake a systematic, integrated evaluation of the patient beginning with history and physical examination, baseline investigations followed by a combination of diagnostic tests, and therapeutic trials based on a suspected cause(s). At present, there is no agreement as to the optimal sequence of tests or empiric trials and no strong evidence that such protocols are associated with superior outcomes to a nonprotocolized approach. A cost-effectiveness analysis of the contrasting management strategies suggested that the test all then treat approach, although the most expensive, had the shortest duration to treatment success compared with a protocol of sequential trials of empiric therapy.
Concerns over health care costs may become the major driver for change in the management of patients with cough. The use of allied health care professionals to manage clinical problems has been suggested as a means of controlling health care expenditure. Arguing that such an approach could reduce the physician workload, decrease patient wait times, and prove cost-effective, Field and colleagues undertook a study comparing the outcomes of patients with chronic cough (defined as greater than 4 weeks duration) managed by physicians with those managed by certified respiratory educators (CREs, ie, a group of allied health care professionals with specialist training and knowledge in respiratory diseases). Patients initially were screened, and those with potentially serious underlying disease were excluded. The primary endpoint was the number of patients reporting cough resolution (subjective improvement) at the 8-week follow-up. The authors reported a greater number reporting improvement in cough (although similar improvements in quality of life), a shorter referral wait time, and lower costs per successfully treated patient in the CRE arm compared with physician-treated arm. Although limited in its design, this study demonstrates that randomized controlled clinical trials of cough management protocols can be undertaken. In the future, such studies will need to be conducted to establish the most practical and cost-effective approach to managing cough. Widespread access to the World Wide Web also has influenced the manner in which the general population access health care information. Dettmar and colleagues reported their initial findings of a prospective cohort study of patients accessing an Internet-based cough clinic diagnostic site designed to suggest a probable diagnosis and offer treatment advice based along international recommendations. Over 8500 individuals completed the online 16-item diagnostic questionnaire and based on responses the causes for cough were identified as reflux (46%), asthma/asthma syndrome (39%), or rhinitis (15%). Unfortunately, the authors were only able to report follow data on a minority (approximately 12%) of participants, and while most of those found the site easy to use, less than two thirds took the recommended treatment. The online cough clinic represents a novel departure from current management of cough, but it may only prove useful for suitably motivated cough patients.
Optimizing the existing protocols for the management of cough
Several consensus statements have been produced to help physicians assess and treat patients with cough. In general, the recommended approach in both adult and pediatric settings is to undertake a systematic, integrated evaluation of the patient beginning with history and physical examination, baseline investigations followed by a combination of diagnostic tests, and therapeutic trials based on a suspected cause(s). At present, there is no agreement as to the optimal sequence of tests or empiric trials and no strong evidence that such protocols are associated with superior outcomes to a nonprotocolized approach. A cost-effectiveness analysis of the contrasting management strategies suggested that the test all then treat approach, although the most expensive, had the shortest duration to treatment success compared with a protocol of sequential trials of empiric therapy.
Concerns over health care costs may become the major driver for change in the management of patients with cough. The use of allied health care professionals to manage clinical problems has been suggested as a means of controlling health care expenditure. Arguing that such an approach could reduce the physician workload, decrease patient wait times, and prove cost-effective, Field and colleagues undertook a study comparing the outcomes of patients with chronic cough (defined as greater than 4 weeks duration) managed by physicians with those managed by certified respiratory educators (CREs, ie, a group of allied health care professionals with specialist training and knowledge in respiratory diseases). Patients initially were screened, and those with potentially serious underlying disease were excluded. The primary endpoint was the number of patients reporting cough resolution (subjective improvement) at the 8-week follow-up. The authors reported a greater number reporting improvement in cough (although similar improvements in quality of life), a shorter referral wait time, and lower costs per successfully treated patient in the CRE arm compared with physician-treated arm. Although limited in its design, this study demonstrates that randomized controlled clinical trials of cough management protocols can be undertaken. In the future, such studies will need to be conducted to establish the most practical and cost-effective approach to managing cough. Widespread access to the World Wide Web also has influenced the manner in which the general population access health care information. Dettmar and colleagues reported their initial findings of a prospective cohort study of patients accessing an Internet-based cough clinic diagnostic site designed to suggest a probable diagnosis and offer treatment advice based along international recommendations. Over 8500 individuals completed the online 16-item diagnostic questionnaire and based on responses the causes for cough were identified as reflux (46%), asthma/asthma syndrome (39%), or rhinitis (15%). Unfortunately, the authors were only able to report follow data on a minority (approximately 12%) of participants, and while most of those found the site easy to use, less than two thirds took the recommended treatment. The online cough clinic represents a novel departure from current management of cough, but it may only prove useful for suitably motivated cough patients.
Developments in the diagnosis and treatment of the common triad of cough etiologies
Asthma, gastroesophageal reflux disease (GERD), and upper airway cough syndrome (UACS) remain the most commonly recognized causes of cough presenting to primary and secondary care physicians. Over the last few decades, there have been few if any changes in the treatment options available for these patients. This is unlikely to change in the immediate future, but several technological developments (in particular noninvasive diagnostic tools) may improve the capacity to accurately identify patients most likely to respond to disease specific therapies. Success in this area would represent a significant advance and influence the approach to treatment of cough in the future. The new developments relevant to each condition in the common triad of cough etiologies will be discussed below.
Asthma/Eosinophilic Airway Cough Syndromes
A trial of inhaled corticosteroids or a short course of oral steroids remains an important strategy in the management of chronic cough. Current guidelines suggest assessing airway inflammation in all patients presenting with cough and giving trials of corticosteroids. This is based on strong evidence that asthma/eosinophilic airway syndromes commonly cause cough. Cough variant asthma (CVA) is characterized by normal spirometry, evidence of bronchial hyper-responsiveness on bronchoprovocation challenge testing, and improvement in cough with bronchodilators or corticosteroids; CVA accounts for between 24 to 35% of those referred to specialist cough clinics. Eosinophilic bronchitis (EB) is characterized by eosinophilic airway inflammation and a steroid responsive cough; unlike asthma, however, it is not associated with bronchial hyper-reactivity or variable airflow obstruction. There is no consensus on the optimal method of assessing airway inflammation, the dose and duration of oral corticosteroid trials, and the required length of treatment with inhaled corticosteroids.
Although well described, the routine use of induced sputum for the assessment of airway inflammation in cough clinics has not been adopted widely. Some of the reluctance to do so relates to the costs and technical expertise required to provide a reliable service. The usefulness of exhaled nitric oxide (eNO) measurements as a surrogate marker of both airway inflammation and hyper-responsiveness has been studied. The measurement of fractional eNO (FeNO) is relatively simple and noninvasive, and levels correlate well with eosinophilic airway inflammation. As FeNO levels are increased in asthmatic coughers and patients with EB, the measurement of FeNO represents an attractive means of selecting patients for steroid treatment. Several studies have sought to identify baseline cutoff values most likely to identify treatment responders. In a study by Prieto and colleagues, 45% of subjects responded well to 4 weeks of treatment with fluticasone (100 mcg twice daily), but their chosen baseline FeNO cutoff value of 20 parts per billion (ppb) was poor at predicting response with a sensitivity and specificity of 53% and 63%, respectively.
The inhalation of mannitol is known to cause bronchospasm and cough possibly by inducing an osmotic effect on the airway, leading to activation of inflammatory cells. Asthmatics cough more than healthy controls, and with the development of mannitol dry powder administration devices, mannitol may prove to be a practical and superior alternative to other indirect bronchial challenge methods in the identifying cough patients likely to respond to a trial of anti-inflammatory therapy.
GERD
Expert opinion largely has prevailed in the development of existing recommendations for treatment of GERD-associated cough. These have focused mainly on the treatment of acid reflux and based on fairly limited evidence have recommended high-dose acid suppression for an extended duration (3 months or longer). The future management and treatment of GERD-associated cough must extend beyond simply suppressing acid with medical therapy and consider the role of new medicines and evolving surgical techniques in the treatment of nonacid (volume) reflux.
The notion that treating GERD-associated cough with acid suppression has been disputed for some time with doubt about the efficacy of trials of acid suppression and the reliability of existing diagnostic techniques (in particular 24-hour esophageal pH monitoring) in identifying those likely to respond to acid suppression having been raised. Recent attention has focused on multichannel intraluminal impedance (MII-pH) monitoring, which has the advantage of identifying and characterizing both acidic and nonacidic reflux episodes. In a study of healthy volunteers using MII-pH, only 25% of reflux episodes reaching the pharynx were nonacidic. Recent findings suggest that nonacidic reflux episodes are strongly associated with episodes of cough. The value of prokinetic agents or treatments such as baclofen (which act directly on lower esophageal tone) in managing volume reflux remains to be confirmed. More likely to have a prominent place in the future treatment of patients with cough caused by the nonacidic and volume effect reflux are surgical techniques such as laparoscopic fundoplication. There have been several open-label studies of laparoscopic fundoplication offered to patients with refractory cough that have reported promising results. How best to identify patients likely to benefit and the exact form of intervention (especially as technological advances in endoscopic procedures emerge) are unknown.
UACS
Most patients with nasal secretions do not complain of cough, and the idea that postnasal drip represents a distinct disease has been questioned. Nonetheless, rhinitis or rhinosinusitis commonly features in the reported causes of cough. The introduction of the term UACS, which encompasses these two upper airway conditions, has helped the move away from the reliance on a symptom profile (postnasal drip) and toward a causative factor. Current recommendations for treating UACS suggest sedating first-generation antihistamines, which although not universally available on prescription, are preferred over newer agents. Intranasal corticosteroids are recommended, but there is a lack of necessary detail as to the dose and duration of therapy.
As with the asthma/airway eosinophilia syndrome, future treatment strategies would be helped greatly by noninvasive methods (ideally a point-of-care test) to identify those likely to respond to specific therapy. At present, there is no support in the literature for the routine use of sinus computed tomography (CT) scanning for patients with chronic cough, as up to 30% of asymptomatic adults will have mucosal abnormalities on imaging nasal NO (nNO) has gained attention as a noninvasive technique in the diagnosis of chronic rhinosinusitis. Low nNO correlates with patients who have chronic rhinosinusitis with nasal polyps and could prove a quick, noninvasive test to identify those patients likely to benefit from medical or also surgical management of their disease. An open interventional study by Macedo and colleagues reports improvement in cough after 28 days treatment with fluticasone nasules, ipratropium bromide, and azelastine nasal sprays.
The future of treatment in this area will be to accurately identify likely responders and advances being made in both medical and surgical of upper airway disease.
Cough reflex hypersensitivity and its association with common acute and chronic cough syndromes
The cough reflex is hypersensitive in a range of respiratory diseases including acute viral cough, asthma, chronic obstructive pulmonary disease (COPD), and pulmonary fibrosis. It is also heightened in extrapulmonary diseases associated with cough such as GERD and rhinosinusitis. The physiology of the cough reflex and the pathophysiological mechanisms responsible for sensitization (peripheral and central) have been detailed elsewhere in this publication by Canning. In this section, the authors suggest that a broader appreciation of the clinical consequences of cough reflex hypersensitization and more insight into the neuroinflammatory events considered mechanistically important should be a priority in future efforts to improve the treatment of cough.
What are the Clinical Characteristics of Cough Reflex Hypersensitivity?
Patients frequently complain of bouts of coughing triggered by relatively innocuous stimuli such as exposure to aerosols and scents, change in air temperature, or when talking, laughing, or singing. These triggers are recognized by approximately two thirds of patients referred with chronic cough, and because they occur during the patients’ normal daily routine, this aspect of their condition is felt to be the most disruptive. In the development of the two most widely used cough quality-of-life questionnaires, items perceived as important by patients included statements such as “exposure to paint or fumes made me cough,” and “I can no longer sing, for example in church”.
Airway hypersensitivity is not the only clinical symptom reported by cough patients, as many describe an unpleasant sensation such as the urge to cough or the feeling of an itch or choking sensation at the back of the throat, or sometimes central chest discomfort. It is likely that these clinical features arise as a direct consequence of cough reflex sensitization, as vagal anesthesia is known to inhibit them. These symptoms are also absent in patients following bilateral lung transplant. The areas of the cerebral cortex and brainstem that may activated by these vagal lung afferents recently have been identified by researchers using functional magnetic resonance imaging of the brain following inhalation of the tussive agent capsaicin by healthy volunteers.
A more widespread appreciation among general and respiratory physicians of the symptom profile of airway sensory hyper-responsiveness reported by cough patients is required. The development of health status questionnaires that capture the impact of airway sensory hyper-reactivity more completely should be developed. These may provide a novel and clinically relevant study endpoint for therapeutic trials in the future.
Factors Associated with Cough Reflex Sensitization and the Development of Chronic Cough
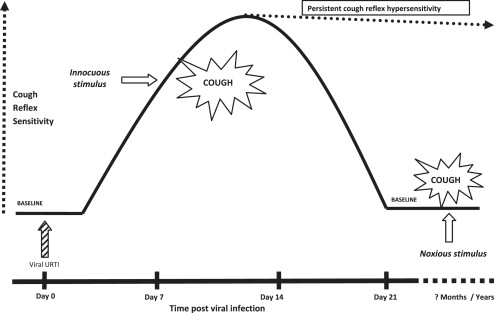
The human cough reflex is in a dynamic state of activation, and several exogenous and endogenous factors may alter the degree of sensitization. One obvious example of this is the change in cough reflex sensitivity following an upper respiratory tract infection. After a viral infection, the cough reflex becomes hyper-reactive and remains in this activated state for a variable period. During this time, the patient is symptomatic, although the cough typically subsides after 2 to 3 weeks, and the hypersensitive cough reflex returns to its baseline state. In some circumstances, however, this hypersensitized state persists long after the initial triggering event, leading to a chronic cough state ( Fig. 1 ). It is unclear if this arises because of direct viral damage of the peripheral sensory nerves or virus-induced changes in central processing of the sensory signal. Several aggravating factors are believed to promote this transition to a chronic cough state, and a schematic of possible relationships has been outlined in the Fig. 2 . Therefore, careful clinical assessment of the patient to identify some of these factors is recommended. In some instances, simply removing the aggravant (angiotensin converting enzyme-inhibitor or cigarette smoke) is sufficient. It is suggested that the coexistence of two or more inflammatory (possibly infective) stimuli to the airway (multiple hit) may be a factor in the development of more severe airway disease. In a recent study of chronic cough patients referred to otolaryngology clinics, Helicobacter pylori infection was detected in 86% of patients compared with 45% of controls. The cough responded to eradication therapy in 75% of cases, suggesting a role for the detection and treatment of H pylori . It is recognized that women are over-represented at cough clinics, but it is not clear why gender has such a strong influence on the development of chronic cough. Females (both healthy and coughers) have a heightened cough reflex compared with males, and there may be hormonal factors that influence airway inflammatory events. On the other hand, this difference may be related to women demonstrating worse cough-related health-related quality of life than men, perhaps related to more urinary incontinence and other adverse effects. Elucidating the mechanisms responsible for this gender association will be an important advance in the development of new treatments for cough.