Purpose
To report the natural history and management outcomes of full-thickness macular hole (MH) caused by momentary exposure to a high-power handheld blue laser device and highlight the dangers of such easily available devices.
Design
Retrospective consecutive case series.
Methods
A chart review of all patients presenting with full-thickness MH from exposure to blue-light high-powered lasers from January 2012 to May 2014 at 2 institutions was performed. Evaluation included a full ophthalmic examination, fundus photography, macular spectral-domain optical coherence tomography, and fundus fluorescein angiography. The main and secondary outcomes were MH closure and final visual acuity, respectively.
Results
There were 17 eyes of 17 patients with full-thickness MH. Best-corrected Snellen visual acuity (BCVA) at presentation ranged from 20/30 to 2/200 (mean: 20/210). The MH minimum diameter ranged from 168 μm to 620 μm (mean: 351 μm). Fourteen eyes underwent pars plana vitrectomy, internal limiting membrane peeling, and gas or silicone oil tamponade. Eleven of the 14 (78.6%) operated eyes had complete closure of the macular hole. Of the 3 unoperated eyes, only 1 eye with the smallest macular hole (minimum diameter: 168 μm) closed spontaneously with observation. Final BCVA in all cases had a mean of 20/62 (range: 20/20–4/200).
Conclusion
Full-thickness MH can result from momentary exposure to high-power handheld laser devices. While spontaneous closure may occur in rare cases, most cases require early surgical intervention. Vitrectomy may be successful in closing the macular hole with visual acuity improvement in most of the cases.
Since the description of macular hole (MH) in the late 1800s by Knapp, several conditions have been associated with macular hole formation. In addition to the commonly encountered idiopathic MH, other etiologies of MH include ocular trauma, retinal vascular disease, retinal detachment, macular pucker, myopia, lightning strike, electric shock, and accidental laser injury. Retinal injuries attributable to different kinds of laser exposure have been reported in the medical literature.
The recent emergence of low-cost, high-power (up to 1400 mW), handheld laser devices has led to a new wave of maculopathies in the young population in Saudi Arabia. Despite the fact that the US Food and Drug Administration has released a safety notification regarding these devices, they continue to be easily obtainable through the Internet.
We recently reported the clinical presentation of a series of patients with macular injuries caused by momentary exposure to high-power, handheld blue laser, including 4 eyes with full-thickness MH. Since then, the number of patients seen with such injuries has more than quadrupled. Also, several cases of handheld laser-induced retinal injuries in the United States and Europe were reported.
The purpose of this study is to report the natural history as well as the anatomic and visual outcomes of 17 eyes of 17 patients with full-thickness MH caused by a high-power handheld blue laser device.
Patients and Methods
The case series presented herein is part of a larger comprehensive study of laser-induced ocular injuries that aims to highlight the emerging dangers of high-powered lasers. It was approved by the Internal Review Board/Ethical Committee at King Khaled Eye Specialist Hospital (KKESH), Riyadh, Saudi Arabia. An informed consent to render treatment was obtained from every patient (or legal guardian, if minor) prior to surgery. From January 2012 to May 2014, 17 patients presented to King Khaled Eye Specialist Hospital and King Abdulaziz University Hospital, Riyadh, Saudi Arabia with full-thickness MH following monocular exposure to a handheld blue laser device. The clinical features of 4 of the 17 patients were previously published. All patients recognized the laser device when they were shown a sample on presentation. Based on the label, this laser device has a wavelength of 450 nm and a power of up to 2000 mW.
Initial and follow-up evaluation included Snellen best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, color fundus photography, and macular spectral-domain optical coherence tomography (SD OCT) scanning (Spectralis HRA; Heidelberg Engineering, Heidelberg, Germany, or Cirrus; Carl Zeiss Meditec, Inc, Dublin, California, USA). The macular hole minimum diameter and base diameter (at the level of retinal pigment epithelium) of the macular hole were measured using the caliper of the software at the horizontal line scan crossing the macular hole center.
The surgeries were performed by multiple surgeons and general anesthesia was used because of the young age of the patients. The surgical technique in all patients consisted of 23 gauge pars plana vitrectomy, posterior hyaloid peeling, brilliant blue–assisted internal limiting membrane peeling, and fluid-air exchange, followed by gas (sulfur hexafluoride or perfluoropropane) or 5000 centistokes silicone oil tamponade. The choice of tamponade was according to the surgeon’s preference. All patients were instructed to assume strict face-down positioning for at least 5 days postoperatively. Snellen BCVA was converted to logarithm of the minimal angle of resolution (logMAR) for statistical analysis.
Results
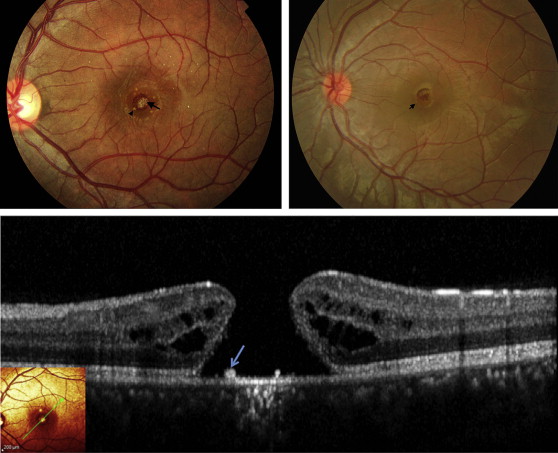
There were 17 eyes of 17 patients with full-thickness MH ( Table ). All patients were young and male with a mean age of 18 (±4.3) years (range, 11–30 years). All injuries were inflicted by others during play, except for 1 patient in whom the injury was self-inflicted. Based on patients’ description, the duration of exposure was estimated to be less than a second in all cases. The approximate distance from the device to the victim’s eye was 0.5–2 meters (mean: 0.95 meters). The interval from the time of injury to presentation to the hospital ranged from 2 days to 16 months. BCVA at presentation ranged from 20/30 to 2/200 (mean: 1.02 logMAR; Snellen equivalent 20/210). Clinically, a round or oval-shaped full-thickness MH was detected in all eyes. In addition, faint whitening was observed at the base of the MH in all eyes. Also, tiny yellowish dots were seen in the bed as well as under the margins of the MH in 6 eyes. These findings were present in both acute and chronic cases ( Figure 1 , Top left and Top right). On SD OCT the presence of a full-thickness MH was confirmed in all eyes. Cystic changes at the margin were seen in 16 out of 17 eyes. The yellowish dots seen on fundus examination appeared as excrescences at level of the apical surface of the retinal pigment epithelium (RPE) on SD OCT (RPE) ( Figure 1 , Bottom). The MH size was variable. The mean macular hole minimum diameter at presentation was 351 μm (ranging from 168 to 620 μm; SD ± 151.7 μm) and the mean macular hole base diameter was 733 μm (ranging from 184 to 1150 μm; SD ± 331 μm).
| Patient No. | Age (y) | Interval From Injury to Presentation | Initial BCVA | Interval Between Injury and Surgery | Preoperative BCVA | Surgical Procedure | Last FU After PPV | BCVA at Last Follow-up | Distance of Laser Device From Eye (m) | MH Size (MD/BD) at Presentation (μm) | MH Size (MD/BD) Prior to Surgery (μm) | Postoperative OCT |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 30 | 2 mo | 20/70 | 8 wk | 20/70 | PPV + ILM peeling + SF6 20% | 18 mo | 20/25 | 0.5 | 401/999 | NA | Closed (focal defect) |
| 2 | 11 | 1 wk | 20/200 | 15 wk | 20/400 | PPV + ILM peeling + SO | 16 mo | 20/30 | 0.5–1 | 170/249 | 150/802 | Closed (focal defect) |
| 3 | 15 | 2 d | 20/400 | 16 wk | 20/400 | PPV + ILM peeling + SF6 20% | 21 mo | 20/25 | 0.5 | 319/633 | 315/607 | Closed (focal defect) |
| 4 | 18 | 2 mo | 20/200 | 16 wk | 20/200 | PPV + ILM peeling + C3F8 15% | 15 wk | 20/20 | 0.5 | 185/216 | 231/276 | Closed |
| 5 | 17 | 2 mo | 20/200 | 12 wk | 20/200 | PPV + ILM peeling + C3F8 15% | 12 mo | 20/25 | 1 | 504/1150 | No FU | Closed |
| 6 | 17 | 2 d | 20/30 | 9 mo | 20/60 | PPV + ILM peel + C3F8 15% | 14 wk | 20/30 | 0.5 | 388/933 | 454/1219 | Closed (focal defect) |
| 7 | 16 | 1 wk | 20/400 | 8 mo | 20/60 | PPV + ILM peeling + SF6 20% | 15 wk | 20/25 | 0.5 | 237/530 | 322/605 | Closed |
| 8 | 14 | 2 wk | 20/100 | NA | NA | None | 5 mo a | 20/60 | 0.5 | 183/327 | 225/378 | Refused surgery |
| 9 | 23 | 2 d | 20/400 | NA | NA | None | 9 mo a | 20/300 | 1 | 168/184 | Closed | Closed (spontaneously) |
| 10 | 20 | 2 mo | 20/80 | NA | NA | None | Lost FU a | NA | 1 | 473/868 | Lost FU | Lost FU |
| 11 | 14 | 1 mo | 2/200 | 4 wk | 2/200 | PPV + ILM peeling + SF6 20% | 3 wk | 20/200 | 2 | 284/641 | NA | Closed; disrupted ellipsoid zone |
| 12 | 15 | 2 wk | 4/200 | 2 wk | 4/200 | PPV + ILM peeling + SF6 20% | 3 wk | 20/100 | 2 | 620/843 | NA | Closed; disrupted ellipsoid zone |
| 13 | 20 | 1 mo | 20/200 | 6 wk | 20/200 | PPV + ILM peeling + SF6 20% | 12 mo | 20/125 | Not known | 270/809 | NA | Closed; disrupted ellipsoid zone |
| 14 | 18 | 16 mo | 20/160 | 17 mo | 20/160 | PPV + ILM peeling + SF6 20% | 12 wk | 20/60 | Not known | 304/1068 | NA | Closed; disrupted ellipsoid zone |
| 15 | 20 | 1 mo | 20/200 | 8 mo | 20/200 | PPV + ILM peeling + C3F8 10% | 4 wk | 20/125 | Not known | 561/958 | 800/1242 | Open |
| 16 | 18 | 8 mo | 20/100 | 11 mo | 20/100 | PPV + ILM peeling + SF6 20% | 3 wk | 20/100 | 1 | 310/857 | NA | Open |
| 17 | 21 | 9 mo | 20/300 | 9 mo | 20/300 | PPV + ILM peeling + SO | 3 wk | 4/200 | 1.5 | 593/1208 | NA | Open |
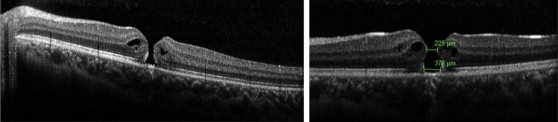
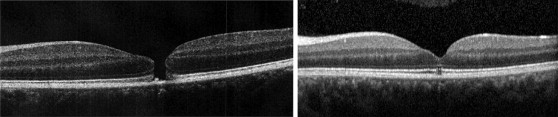
Eight patients were observed for a period ranging from 3 to 9 months, of which 7 elected to be observed for longer than 3 months owing to their reluctance to proceed with surgery. These were reassessed according to physician best judgment at an interval of 2–3 months with examination and SD OCT. In all observed patients, the mean macular hole minimum diameter at presentation was 276 μm (ranging from 168 to 561 μm; SD ± 139.9 μm) while the mean macular hole base diameter was 503.7 μm (ranging from 184 to 958 μm; SD ± 313.7 μm). After observation, the mean macular hole minimum diameter was 312 μm (ranging from 0 to 800 μm; SD ± 237.9 μm) while the mean macular hole base diameter was 641.5 μm (ranging from 0 to 1242 μm; SD ± 437 μm). In 6 of these patients (6 eyes), the MH enlarged in size ( Figure 2 ). In 1 patient the MH size remained stable and in only 1 patient, whose eye had the smallest MH (minimum diameter 168 μm and base diameter 184 μm) in this series, did the MH close spontaneously ( Figure 3 ). The faint whitening that was seen in all cases did not change in appearance with observation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


