Purpose
To evaluate the potential use of fluorescence confocal microscopy (FCM) for ex vivo diagnosis and excision margin assessment of conjunctival neoplasms.
Design
Validity study.
Methods
setting : Single institution. participants : Consecutive patients with clinically suspicious conjunctival lesions. intervention : Conjunctival lesions were excised in toto using a standard “no-touch technique” by a single surgeon (A.I.). Collected specimens were examined with a commercially available laser scanning fluorescence confocal microscope after immersion in a 0.6 mM solution of acridine orange dye for 10–20 seconds. Specimens were subsequently processed with standard histologic analysis. main outcome measures : FCM diagnosis of the nature and extension of conjunctival lesions.
Results
Sixteen consecutive patients were included in the study (11 male, 5 female; mean age 58.1 ± 26.1 years, range 10–90 years). The median time needed to process and analyze a sample with FCM was 15 minutes. Eleven of 16 lesions were identified by FCM as squamous (2 benign papillomas, 2 grade 2 conjunctival intraepithelial neoplasias, 7 in situ squamous carcinomas) and 5 as nonsquamous (1 pingueculum, 1 dermolipoma, 2 melanocytic nevi, 1 melanoma). In all cases FCM was able to detect horizontal and vertical extension of the lesion. All FCM findings were confirmed by corresponding subsequent histologic examination.
Conclusions
FCM provides a fast ex vivo preliminary diagnosis of suspicious conjunctival lesions with good histologic details and margin assessment, and may represent a novel tool for intraoperative and postsurgical management of conjunctival tumors. This is the first study to investigate ex vivo FCM application in ophthalmology.
Among ocular tumors, conjunctival neoplasms encompass a wide range of lesions with different clinical features and management strategies.
The most common conjunctival neoplasm is ocular surface squamous neoplasia (OSSN), a term used to describe neoplastic squamous lesions of the conjunctiva ranging from mild dysplasia to invasive squamous carcinoma, but many other proliferative lesions can be found in clinical practice.
Currently, diagnosis of conjunctival tumors is essentially based on clinical appearance. Postexcision histopathologic examination is considered the diagnostic gold standard for diagnosis of nature and extension of conjunctival lesions. Brushing, exfoliative or impression cytology, and incisional map biopsies can be performed as in-office procedures to aid the diagnosis prior to surgical excision, but are often difficult to interpret. Moreover, these methods can only analyze a superficial and/or limited area of the entire lesion, which may provide partial and misleading information.
The traditional therapeutic approach to conjunctival neoplasms is based on surgical excision with a “no-touch” technique or topical chemotherapy. To this day, only assessment of margin involvement on excised specimens by histopathologic analysis defines whether a certain lesion has been fully excised and determines prognosis and recurrence rate. Because the extension of the lesion is only defined clinically, postexcision recurrences do happen as a consequence of residual disease and/or micrometastases. On the other hand, extensive surgical resection and topical chemotherapy can result in scarring with secondary limbal stem cell deficiency and symblepharon formation.
Confocal microscopy in reflectance mode (reflectance confocal microscopy, RCM) is based on the natural differences between tissues and has been extensively used for in vivo imaging in ophthalmology in a variety of anterior segment diseases. Several studies have preliminarily investigated the use of RCM in the diagnosis of conjunctival neoplasms, but to date RCM has not been incorporated in the diagnostic evaluation of conjunctival lesions.
Confocal microscopy in fluorescence mode (fluorescence confocal microscopy, FCM) uses fluorescent dyes (fluorochromes) to enhance the contrast of cellular and tissue structures on confocal imaging. FCM has been successfully applied ex vivo on surgical specimens to analyze a wide range of neoplastic and nonneoplastic diseases. In fact, fluorochromes in confocal imaging act like dyes in histopathology and allow identification of cellular and tissue structures. The choice of the fluorochrome depends on the wavelength of the exciting light as well as the target cellular or tissue feature.
The aim of the current pilot study was to investigate whether ex vivo FCM could be employed to rapidly define the nature and the extension of excised conjunctival lesions, in order to provide intraoperative guidance to the surgeon.
Methods
Patients and Surgery
Consecutive patients with conjunctival lesions evaluated at a single institution (Cornea and External Eye Diseases Clinic, Department of Ophthalmology, Arcispedale Santa Maria Nuova – IRCCS, Reggio Emilia, Italy) were included in the study.
The study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Intramural Review Board. Informed consent was obtained from all participants.
Surgical excision of conjunctival lesions was performed under local anesthesia by a single surgeon (A.I.) with a standard “no-touch” technique. All excised samples were placed on filter paper with a schematic drawing of the ocular surface to provide precise orientation of the specimen and dipped in 0.9% balanced salt solution for FCM.
Fluorescence Confocal Microscopy Analysis
FCM analysis was performed by a single pathologist (M.R.) skilled in reading FCM images. In this study, the VivaScope 2500 confocal microscope (Mavig, GmbH, Munich, Germany) was used for FCM. Technical characteristics of the instrument are described elsewhere.
All samples placed on filter paper were recovered from balanced salt solution and immersed for 10–20 seconds in a 0.6 mM solution of acridine orange, a fluorescence dye that stains nuclear DNA and cytoplasmic RNA. Acridine orange is particularly useful for studying epithelial neoplasms; therefore it is particularly indicated for conjunctival lesions. The samples were gently dabbed with tissue paper to remove excessive fluorescent solution and then analyzed with FCM.
The images were scanned in 2 dimensions along x- and y-axes by using a diode laser illumination at a wavelength of 488 nm (blue fluorescence wavelength) with a ×30, 0.9 numerical aperture water immersion objective lens. The horizontal optical resolution was <2 μm at the center of field of view, and the vertical (axial) optical resolution was <5 μm at the center of field of view. The maximum depth of imaging was up to 250 μm, depending on tissue type. Because the microscope is confocal, only the in-focus plane is visualized. Because penetration of the fluorophore within the specimen is not consistent (ie, more intense on the outside, weaker in the middle owing to less penetration of fluorophore), the focus plane had to be adjusted throughout the specimen by moving the objective lens up or down. Depth measurements can be obtained from the z-axis precision stepper motor by setting zero at the most superficial layer before scanning vertically into the tissue.
Time for image acquisition depends essentially on sample size. In our study, sample size ranged from 7 × 3 mm to 12 × 12 mm and images were created in a time that ranged from a few seconds to 5 minutes accordingly. The time needed for FCM analysis was recorded in each case.
For each sample, FCM analysis was performed in 2 sequential steps:
- (1)
Analysis of the histopathologic nature, horizontal extension (x, y), and excision margins: The sample was placed between silicon-sealed glass slides “en face” (ie, as it would appear on the ocular surface) and mounted on a specific support of the confocal microscope over the instrument window. In 1 case, in which the dimensions of the sample exceeded the size of the instrument window, the sample had to be divided in half and the 2 halves analyzed separately.
- (2)
Evaluation of vertical extension: A central transversal section of the excised lesion was then obtained, immersed again in acridine orange for 10–20 seconds, mounted transversally on the glass slides, and analyzed similarly with FCM to define the depth (z) of tissue involvement.
For each oriented specimen, a fast sequence of bidimensional high-resolution bitmap images was acquired. The single images were then assembled into a “mosaic” that displayed the entire area of the tissue specimen. The size of the mosaic corresponded to the size of the specimen and ranged from 7 × 3 mm to 12 × 12 mm.
Higher-magnification images were then obtained by digitally zooming the acquired mosaic in and out. The display has 1000 × 1000-pixel resolution, so image resolution when “zoomed out” depended on the size of the mosaic. Image resolution ranged from 0.75 μm/pixel in a single bitmap image to 12 μm/pixel in a 12 mm × 12 mm mosaic, when viewing the entire mosaic at once.
The instrument converts acridine orange fluorescence signal into grayscale with an analyzing software and the brightness of the resulting image is proportional to the DNA/RNA content. When the nuclei are packed together, as in high-grade epithelial dysplasia, the fluorescence is high and the images are bright. In the absence of a fluorescent signal (ie, when the tissue is hypocellular, as in fibrous or in adipose tissue), the background is darker because the signal intensity is lower. Consequently, specific FCM characteristics allowed broad definition of the lesion’s nature (epithelial, fibrous, adipose, etc), as well as the resection margin status.
Owing to acridine orange fluorescence decay time, a maximum of 2 images per sample were acquired. No image selection was made, and all acquired images were analyzed.
Conventional Histopathology
Following FCM the samples were formalin-fixed and paraffin-embedded. Care was used to keep the same spatial orientation for FCM and to preserve tissue during the cutting procedures. Three-millimeter-thick slices of the embedded tissue were mounted on glass slides and stained with hematoxylin and eosin (H&E) with a standard protocol for histologic evaluation. Histologic diagnosis was rendered according to WHO criteria by a single pathologist (S.P.). Features of FCM images were compared side by side with pathology sections.
The pathologists performing FCM analysis was aware of clinical suspicion. The pathologist conducting standard histopathology was masked to preoperative FCM analysis results.
Results
Sixteen patients (11 male, 5 female; mean age 58.1 ± 26.1 years, range 10–90 years) with conjunctival lesions were included in the study ( Table 1 ).
| Patient | Lesion | Time for FCM Image Acquisition and Analysis (Minutes) | Margins Involvement, FCM | Margins Involvement, Histology | Recurrences | Postoperative Follow-up (Months) |
|---|---|---|---|---|---|---|
| 1 | CIS | 20 | N | N | N | 26 |
| 2 | Squamous papilloma | 10 | Y (corneal) | Y (corneal) | Y | 24 |
| 3 | Pingueculum | 6 | N | N | N | 22 |
| 4 | CIS | 20 | N | N | N | 22 |
| 5 | CIS | 15 | Y (corneal) | Y (corneal) | Y | 21 |
| 6 | CIS | 20 | N | N | N | 19 |
| 7 | Dermolipoma | 6 | N | N | N | 13 |
| 8 | Invasive squamous carcinoma | 20 | N | N | N | 12 |
| 9 | CIS | 15 | N | N | N | 9 |
| 10 | Melanocytic nevus | 8 | N | N | N | 8 |
| 11 | CIN grade 2-3 a | 15 | N | N | N | 4 |
| 12 | CIS | 20 | N | N | N | 2 |
| 13 | CIN grade 2-3 a | 15 | Y | Y | N | 2 |
| 14 | Squamous papilloma | 10 | N | N | N | 2 |
| 15 | Spitz melanocytic nevus | 12 | N | N | N | 1 |
| 16 | Melanoma | 9 | N | N | N | 1 |
Following surgical excision, FCM analysis was performed on all samples in an average time ≤20 minutes (range 6–20 minutes; median time 15 minutes) for both sequential steps. Time required for FCM analysis was primarily related to sample size. Postexcision follow-up ranged between 1 and 26 months (median follow-up time: 10.5 months). FCM was capable of identifying lesion margins and depth of involvement in all cases, in perfect accordance with histopathology. Unequivocal diagnosis of the lesion’s nature was only possible for squamous neoplasia; for nonsquamous lesions, a presumptive diagnosis of nature could be made based on FCM findings but ultimately needed histopathology confirmation (see following description).
Representative lesions are described below and summarized in Table 2 .
| Type of Sample | FCM Characteristics | Histopathology Characteristics |
|---|---|---|
| Normal squamous epithelium | Few layers of bright round monomorphous spots evenly spaced and becoming flat at the surface, corresponding to the normal-maturing squamous cells. | Multilayered, nonkeratinizing squamous epithelium, loosely adherent to the underlying tissue. Epithelial cells are round, monomorphous, and evenly spaced. |
| OSSN | Thicker epithelium composed of bright spots with different sizes and shapes, haphazardly distributed and crowded without visible maturation. | Acanthotic, thicker squamous epithelium with cytologic atypia, dyskeratinocytes, and partial (in dysplasia) or complete (in SCC) loss of polarity and maturation. |
| Conjunctival degeneration (pingueculum) | Normal squamous epithelium (see above). Grayish hypofluorescent subepithelial connective tissue with numerous hyperfluorescent thin disarranged bands, corresponding to elastosis. | Normolayered or atrophic squamous epithelium overlying a band-like zone of actinic elastosis. |
| Connective lesions (dermolipoma) | Normal thin epithelium (see above). Subepithelial mass composed of grayish hypofluorescence bundles and black spaces surrounded by a thin network of fluorescent lines (adipose tissue). Fluorescent appendageal structures could be identified (eg, hair follicles). | Normolayered squamous epithelium overlying a subepithelial nodule of dense collagenous bundles and mature adipose tissue. |
| Melanocytic nevus | Subepithelial dark spaces encircled by a double layer of bright spots corresponding to the conjunctival epithelial enfolding. | Bland-looking, heavily pigmented melanocytes located in the subepithelial connective tissue and intimately admixed with the cystic inclusions of the conjunctival epithelium. |
| Melanoma | Fluorescent elongated cells disposed in nests and cords, hiding the epithelial lining. | Atypical, sometimes elongated, overcrowded melanocytes growing haphazardly in the connective tissue, scarce pigment; thinning of superficial epithelium. |
Ocular Surface Squamous Neoplasia
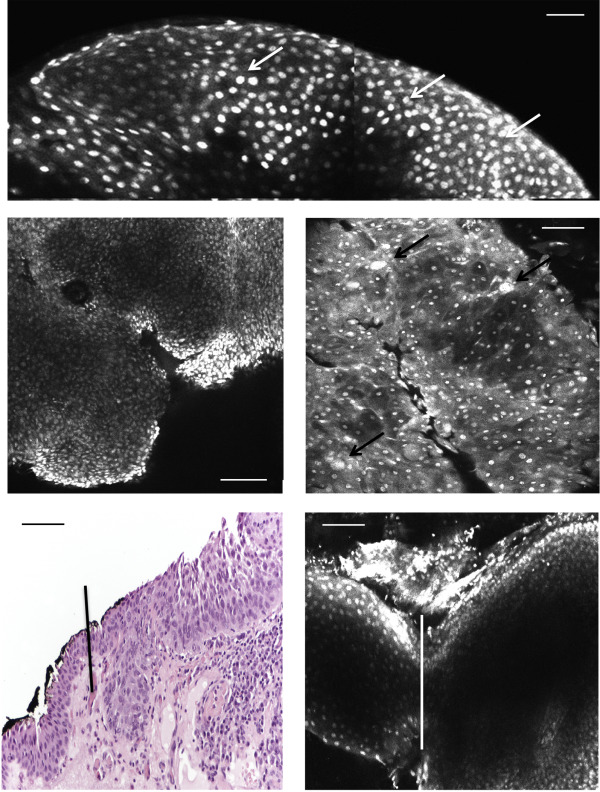
OSSN constituted the majority of the analyzed cases. Seven cases were squamous carcinoma in situ, and 2 cases showed high-grade dysplasia. In all cases FCM was able to recognize high-grade dysplasia (conjunctival intraepithelial neoplasia grade 2–3)/squamous carcinoma in situ (CIS) from normal epithelium ( Figure 1 ). Nondysplastic squamous epithelium of the conjunctiva was thin and composed of evenly spaced bright spots, which became flat at the surface of the epithelium, corresponding to the normal maturing squamous cells ( Figure 1 , Top). High-grade dysplasia showed crowded bright spots corresponding to enlarged nuclei, and sometimes atypical nuclei were also evident ( Figure 1 , Center left, Center right). An abrupt transition between healthy and dysplastic epithelium was also visible in the transversal section ( Figure 1 , Bottom left, Bottom right).
Case 1
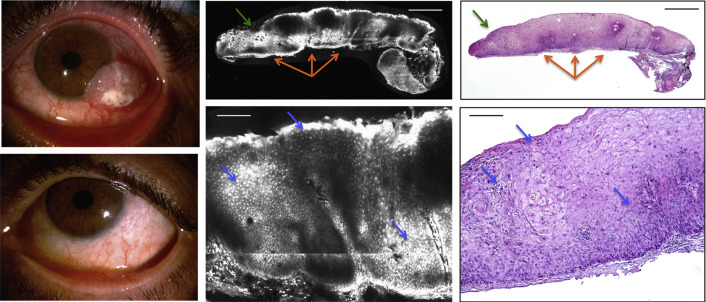
An otherwise healthy 54-year-old man was referred to our clinic for a mass that had been growing in his left eye over the past year. Slit-lamp examination showed a voluminous left limbal gelatinous lesion with superficial leukoplakia ( Figure 2 , Top left). On FCM, fluorescent spots corresponding to epithelial cells were irregularly shaped within a cohesive architecture ( Figure 2 , Top center, Bottom center). Some scattered fluorescent elongated nuclei, corresponding to subepithelial fibroblasts on H&E, were also visible and highlighted the distinction between epithelium and connective tissue. No epithelial invasion through the basal membrane was identified in the sample. These findings were consistent with squamous CIS. Subsequent histopathologic examination confirmed the diagnosis ( Figure 2 , Top right, Bottom right).
Case 2
A 33-year-old woman came to our attention with a right lower lid papillomatous lesion with superficial neovascularization ( Figure 3 , Left). The lesion had been previously excised twice. Upon FCM analysis, papillary structures were distinguishable as arborescent projections made up of scanty bright spots (nuclei of fibroblasts that make up the fibrovascular stalk) and surrounded by a thicker, irregular bright ribbon, representing the epithelial cells’ nuclei ( Figure 3 , Center left, Center right). The latter were extremely monomorphous and regularly spaced, suggesting a benign papillomatous epithelial proliferation ( Figure 3 , Right). The findings were further confirmed by histopathology, and the lesion was identified as a benign squamous papilloma ( Figure 3 , Center right).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


