Purpose
To report the technical aspects, complications, and outcomes concerning fine needle aspiration biopsy (FNAB) in uveal melanoma.
Design
Retrospective cohort study.
Methods
Patients with uveal melanoma who underwent transscleral or transvitreal FNAB at an ocular oncology center were retrospectively evaluated. FNAB was performed if the tumor was more than 5 mm in thickness. Array comparative genomic hybridization analysis was performed on biopsy samples with sufficient tissue. The main outcome measures were success (sample that gave a successful result for biomarker analysis) rate, complications, liver metastasis, and overall survival.
Results
There were 217 (114 male, 52%) consecutive study patients with a mean age of 56.7 (16–84) years. The mean follow-up period was 31 (range 3.6–61.3) months. Mean tumor thickness was 8.4 (range 5–12) mm. The overall success rate of the procedure was 169 patients (77.9%). Thirty-one patients (14.3%) experienced intravitreal hemorrhage, of whom 9 (4.1%) required vitreal surgery. There was no case of endophthalmitis, orbital dissemination, local recurrence, or rhegmatogenous retinal detachment. Thirty-two patients (14.7%) developed metastasis during the study, of whom 20 (9.2%) died. Of the 169 successful samples, 53 patients (31%) were classified as low risk, 41 (24%) as intermediate risk, and 54 (32%) as high risk. Fifteen patients (9%) did not have any detectable chromosomal abnormality and 6 (4%) could not be classified.
Conclusion
FNAB is a relatively safe and successful technique that can be routinely used to obtain tissue for molecular genomic analysis; such analysis helps determine the diagnosis and prognosis in uveal melanoma.
In general oncology, the treatment of malignant tumors requires histologic confirmation of the clinical diagnosis. For intraocular tumors such as uveal melanoma, the most common primary intraocular malignancy in adults, treatment decisions are mostly based on clinical examination. Approximately 50% of the patients with uveal melanoma develop liver metastasis during follow-up in spite of the availability of efficacious therapies for local control of this condition. Death generally occurs within a year of detection of metastasis.
Risk factors for metastasis include clinical and histologic characteristics of uveal melanoma such as the greatest tumor diameter, significant tumor thickness, extrascleral extension, epithelioid cell type, and high mitotic index. Many studies have been performed in the last 15 years on samples obtained from enucleated globes. These and other studies have shown that the prognosis of uveal melanoma is strongly linked to genetic findings in the patient tumor using genomic and transcriptomic analysis.
Fine needle aspiration biopsy (FNAB) enables the sampling of uveal melanoma tumors for molecular analysis without having to perform enucleation. Consequently, FNAB plays an important role in determining prognosis in uveal melanoma; accurate estimation of prognosis helps in effective patient counseling and in implementing guidelines for follow-up of patients and inclusion in adjuvant therapy trials. Further, the identification of patients with poor prognosis, based on molecular genetics results, may allow early detection of metastasis.
The 2 principal routes for tissue sampling with FNAB are either transvitreal or transscleral, depending on the tumor location and surgical practice. Concerns have been raised about possible local complications and systemic risk associated with FNAB following the wider use of this procedure. However, many authors have routinely used FNAB without any serious adverse events. We report, in this retrospective study of 217 patients with uveal melanoma, our experience of FNAB (transvitreal and transscleral) with reference to its technical aspects, complications, and patient outcomes.
Methods
This is a retrospective cohort study that followed the tenets of the Declaration of Helsinki. This study was performed in accordance with French legislation and after approval by the Curie Institute ethics committee: CRI (Comité sur la recherche institutionnelle). The study patients had given fully informed, written consent before undergoing FNAB.
All patients referred to our oncology center with the diagnosis of uveal melanoma were prospectively enrolled in our institutional database: MACRO (version 3.0.75) (InferMed, London, UK). The diagnosis of uveal melanoma was based on complete ophthalmic examination and ultrasonography. Each patient was staged according to the collaborative ocular melanoma study classification and the guidelines of the 7th edition of the American Joint Committee on Cancer (AJCC) TNM (Tumor Node Metastasis) staging system. The data recorded in our database included age, sex, tumor diameter, tumor thickness, exact tumor location, and invasion of the ciliary body during transillumination of the globe. Tumor thickness was measured by ultrasonography. The largest tumor diameter was measured during the surgical procedure, using transillumination if possible. The information obtained using FNAB has been recorded in our database since 2009.
The case records of 217 consecutive patients with uveal melanoma who underwent FNAB in our institute between January 2009 and August 2014 were retrospectively evaluated. Inclusion criteria were patients with a diagnosis of uveal melanoma, with tumor thickness ≥5 mm, treated with proton beam therapy or iodine 125 brachytherapy, and who had undergone FNAB. Exclusion criteria were patients with a small uveal melanoma (thickness less than 5 mm) or large tumors that required primary enucleation (thickness more than 12 mm and/or diameter more than 18 mm). Patients with a doubtful diagnosis of uveal melanoma were also excluded. Tumor samples were obtained by the pathologist from enucleated globes in patients with large tumors that required primary enucleation ; these patients were excluded from the study.
Fine Needle Aspiration Biopsy Techniques
FNAB was performed only if the uveal melanoma was ≥5 mm in thickness. Tumors anterior to the equator were sampled using a transscleral approach, while tumors posterior to the equator were sampled using the transvitreal approach when transscleral biopsy was not possible. Both transscleral and transvitreal biopsies were performed, under sterile conditions, with a needle: 23 gauge for transscleral and 25 gauge for transvitreal. Only 1 biopsy was performed. Four different surgeons with sufficient training and experience performed the FNAB procedures. No histologic examination was performed when tumor sampling was obtained by FNAB.
The first step in FNAB was the localization of the tumor base with transillumination.
Then, FNAB was performed using a transscleral approach targeting the center of the tumor. The specimen was aspirated with a 2 mL syringe connected to the needle by tubing and immediately sent to the ocular pathologist in a tube containing Roswell Park Memorial Institute medium. Cyanoacrylate glue was applied to close the hole to minimize the risk of secondary local dissemination. Transvitreal biopsies were performed under microscopic control and cryotherapy was used to seal the site in order to minimize the risk of secondary dissemination.
Tumor samples were sent to the somatic genetic laboratory to perform array comparative genomic hybridization analysis. There, they were centrifuged at 2000 RPM, decanted to obtain the pellets, and immediately snap-frozen in liquid nitrogen before being stored at −80 C. Then, DNA was extracted according to a standard phenol/chloroform method using Phase Lock Gel Light (Eppendorf, Hamburg, Germany).
The quantity and quality of the obtained DNA were estimated in 2 steps. Firstly, a Nanodrop spectrophotometer was used to assess gDNA purity (for optimal labeling yield, samples should have A260/A280 ≥ 1.8 and A260/A230 ≥ 1.9). Then, a Qubit dsDNA BR Assay Kit (Life technologies, Eugene, Oregon, USA) was used to measure the double-stranded DNA concentration. For each sample having good quality and sufficient quantity, 700–1000 ng of tumor DNA and reference DNA were labeled, purified, and co-hybridized in equal quantity to the NimbleGen Arrays (Roche NimbleGen Inc, Madison, Wisconsin, USA) or Agilent Microarrays (Agilent Technologies, Santa Clara, California, USA) over 12–24 hours. The arrays were washed and scanned according to their technology and manufacturers’ instructions.
For NimbleGen, images were acquired on a GenePix 4000B scanner with GenePix V.6.6 software (Molecular Devices, Sunnyvale, California, USA) and data extracted using the NimbleScan V.2.5 software. Files produced by NimbleScan software were then analyzed on SignalMap V.1.9. For Agilent, images were acquired on a SureScan microarray scanner using CytoScan software V.2.7 and then analyzed with CytoGenomics software V.2.7. All the 169 obtained profiles were interpretable with good-quality reports based on the classical parameters for array comparative genomic hybridization (aCGH) such as the sex mismatch dynamics between the control and the tested sample, standard deviation of the Log2(R) around zero, and thickness of the smoothing signal.
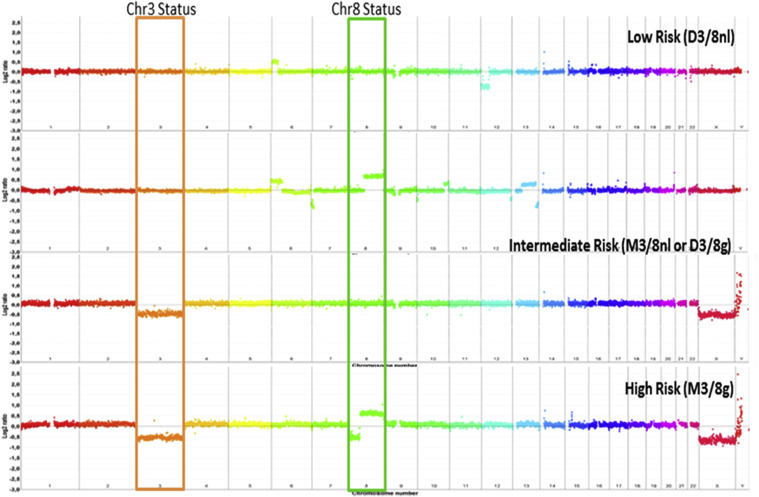
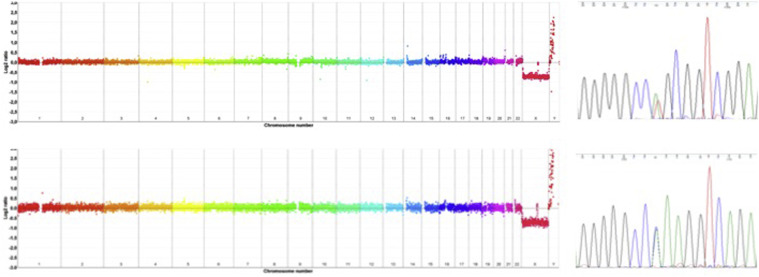
The patients were then classified into low-risk, intermediate-risk, and high-risk categories according to genomic results based on the work of Cassoux and associates, who defined 4 genomic types based on the status of chromosomes 3 and 8. Tumors with disomy 3 and normal dosage of chromosome 8 (termed “D3/8nl”) were classified as low risk. Both monosomy 3 and normal dosage of chromosome 8 (termed “M3/8nl”) and disomy 3 and any type of gain of chromosome 8 (“D3/8g”) were classified as intermediate risk. Finally, monosomy 3 with any type of gain of chromosome 8 (“M3/8g”) was classified as high risk ( Figure 1 ). For patients with no detectable aberration, classical GNAQ/11 Sanger sequencing was performed to assess the tumoral content of the sample ( Figure 2 ).
Patient Follow-up
The first follow-up visit was scheduled 1 month after the treatment and then every 6 months; these follow-up visits involved comprehensive ophthalmic examinations (visual acuity, slit-lamp biomicroscopy, fundus examinations, and ultrasonography) and ultrasound scan of the liver.
All complications occurring after FNAB were recorded during the follow-up period and potentially included any of the following: endophthalmitis, retinal detachment, intravitreal hemorrhage, secondary dissemination, local recurrence, and FNAB failure. Intravitreal hemorrhages were classified as localized or diffuse. Surgical vitrectomy was performed for diffuse hemorrhages that were associated with severe loss of vision and were still persistent at the 1 month posttreatment visit. Endoresection was also performed at the same time if the thickness of the tumor was more than 8 mm. Liver metastases were confirmed by histologic examination and the patients were then referred to general oncologists. Clinical, pathologic, and genomic data at diagnosis and during follow-up were retrospectively collected from the institutional database. The French Death Registry was consulted to determine the status of patients who were lost to follow-up.
Statistical Analysis
All statistical analyses were performed using R software, version 2.13.2. from CRAN PROJECT ( www.r-project.org ). The means and medians have been provided with their respective range. Proportions were compared by χ 2 test or Fisher exact test when theoretical assumptions were not verified. The overall survival was estimated using the Kaplan-Meier method. The relevant time was calculated from the date of diagnosis to the date of death or to the date of the last contact. P values less than 5% ( P < .05) were considered as statistically significant.
Results
A total of 217 patients were enrolled in this study, of whom 5 were lost to follow-up but were still alive based on information from the French Death Registry. The study group comprised 114 men (52%) and 103 women (48%) with the median age at diagnosis of 56.7 (range 16–84) years. The median follow-up was 31 (range 3.6–61.3) months. The mean tumor diameter was 13.9 (7–18.4) mm and the thickness was 8.4 (4.5–11.8) mm. According to the AJCC (7th edition, 2010) clinical staging of uveal melanoma, the classification was as follows: 50 patients T2 and 167 T3.
One hundred and ninety-nine patients (91.7%) were treated with proton beam therapy and 18 (8.3%) with iodine 125 brachytherapy. One hundred and eighty-five patients (85%) underwent transscleral biopsy and the remaining 32 (15%) underwent transvitreal biopsy.
Concerning postoperative complications, no patients developed rhegmatogenous retinal detachment in the follow-up period, although 2 patients experienced worsening of their exudative detachments. There were 31 (14.3%) intravitreal hemorrhages, of which 17 were diffuse and 14 localized. Twenty-one of these patients (67.7%) had undergone a transvitreal biopsy and 10 (32.3%) a transscleral biopsy. Considering the route of FNAB, intravitreal hemorrhage occurred in 21 transvitreal biopsy patients (65.5%) compared with 10 transscleral biopsy patients (5.5%). Nine patients (4.1%) required surgical vitrectomy for refractory diffuse hemorrhages; 6 were secondary to transvitreal biopsies (18.8% of transvitreal patients) and 3 to transscleral biopsies (1.6% of transscleral patients). By 6 months postoperatively, the vitreous hemorrhages had spontaneously cleared in the remaining 22 patients. We did not observe any case of endophthalmitis, orbital dissemination, or local treatment failure during the follow-up period.
One hundred and sixty-nine samples were sufficient for successful molecular analysis, giving an overall success rate of 77.9%. The success rate was 75.1% in transscleral biopsy and even higher (93.8%) for transvitreal procedures. Of the 169 patients with positive biopsy (sample with a successful result for biomarker analysis), 53 patients (31%) were classified as low risk (D3/8nl), 41 (24%) as intermediate risk (M3/8nl) or (D3/8g), and 54 (32%) as high risk (M3/8g). Fifteen patients (9%) did not have any chromosomal abnormality (flat profile on comparative genomic hybridization analysis). Six patients (4%) could not be classified because they had partial loss of chromosome 3. Genomic classification was possible in an additional 9 patients (1 low risk, 3 intermediate risk, 2 high risk, 1 with partial chr3q loss, and 2 flat profiles) following secondary endoresection.
The 15 patients without chromosomal aberration visible by aCGH were genotyped for GNAQ/11 mutation assessment, since these genetic mutations are specific markers of uveal melanoma. Six were mutated (5 in GNAQ and 1 in GNA11) and could be classed as low risk, 7 were wild type (ie, no mutation of GNAQ/11), and 2 were indeterminate. We reconsidered the diagnosis of uveal melanoma in these 7 patients and hence reviewed their case records; retinal photography and ultrasonography were, however, always consistent with uveal melanoma.
Thirty-two patients (14.7%) developed metastasis during the follow-up period; of these, 19 (59%) had a high-risk profile, 5 (16%) had intermediate risk, and 1 (3%) had low risk. Seven patients (22%) did not have sufficient material for genetic analysis. Twenty patients (9.2%) died during the follow-up period owing to metastatic disease. The estimate for the overall survival at 36 months was 87.7% (82.3%–93.4%) using the Kaplan-Meier curve ( Figure 3 ).



