Extraocular Muscles, Strabismus, and Nystagmus
Deborah Pavan-Langston
Nathalie Azar
I. Normal Anatomy and Physiology of the Extraocular Muscles
Innervation and action. All four recti muscles and the superior oblique (SO) muscle originate at the orbital apex (Fig. 12.1). The four recti muscles arise from the annulus of Zinn. The inferior oblique originates at the inferior medial aspect of the inferior orbital rim.
The medial rectus (MR) muscle courses anteriorly along the medial aspect of the globe to insert 5.5 mm posterior to the limbus. Innervation is by the third cranial nerve. Contraction of the muscle causes the eye to turn inward (adduct) toward the nose.
The lateral rectus (LR) muscle courses anteriorly along the temporal aspect of the globe to insert 6.9 mm posterior to the limbus. Innervation to this muscle is by the sixth cranial nerve. Contraction causes the eye to turn outward (abduct) horizontally.
The superior rectus (SR) muscle runs over the dorsal aspect of the eye to insert 7.7 mm posterior to the limbus. Innervation is via the third cranial nerve. Contraction produces various combinations of vertical, horizontal, and rotary movement, depending on the angle of gaze of the eye. As the muscle runs forward at an angle of 23 degrees to the axis of the globe and inserts anterior to the center of rotation of the eye, the movement produced by contraction of the muscle would be pure elevation if the eye were at a horizontal starting position of 23 degrees abduction. If the eye were adducted inward to a position of 67 degrees, the only movement on contraction of the SR would be intorsion of the globe. With the eye in the primary position of straight-ahead gaze, contraction of the muscle produces combined elevation and intorsion with slight adduction.
The inferior rectus (IR) muscle courses along the ventral aspect of the globe at an angle of 23 degrees to the axis of the globe to insert 6.5 mm posterior to the limbus. Innervation to this muscle is also via the third cranial nerve. Contraction produces various combinations of vertical, horizontal, and rotary movement, depending on the horizontal position of the eye. With the eye at a position of 23 degrees abduction, the only movement is depression. If the eye is adducted inward to a position of 67 degrees, the only movement is extorsion as the muscle inserts anterior to the center of rotation of the globe. When the eye is in the primary position, contraction of the IR produces depression and extorsion with minimum adduction.
The SO muscle runs forward along the superomedial wall of the orbit to pass through the trochlea, where it turns backward temporally, traveling at an angle of 51 degrees to the globe axis over the dorsal aspect of the globe but ventral to the SR muscle. It inserts on the posterotemporal surface. Innervation to this muscle is by the fourth cranial nerve. Contraction results in various combinations of vertical, horizontal, and rotary movements, depending on the location of the eye horizontally. With a starting position of 39 degrees of abduction, the only movement is intorsion. With
a starting position of 51 degrees of adduction, the only movement is depression. If the eye is in the position of primary gaze, the motion is combined intorsion and depression with minimum abduction. Abduction is secondary to the muscle insertion being posterior to the ocular rotation center when the eye is in the primary position.
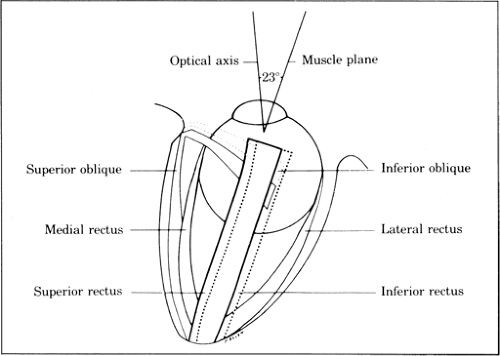
Figure 12.1. Dorsal view of extraocular muscle attachments to the eye. Dotted lines are muscles inferior to the globe. (Adapted from
von Noorden G, Manumenee AE. Atlas of strabismus. St. Louis: Mosby, 1967.)
The inferior oblique (IO) muscle originates at the posterior aspect of the orbital rim nasally and runs backward and temporally at an angle of 51 degrees to the globe axis to insert under the LR muscle in the macular area. The inferior oblique muscle runs ventral to the inferior rectus muscle. Innervation to this muscle is by the inferior division of the third cranial nerve. Contraction produces various combinations of vertical, rotary, and horizontal movements. Starting from a 39-degree position of abduction, the only movement is extorsion. If the starting position is 51 degrees of adduction, the only movement is elevation. Contraction of the muscle with the eye in the primary position produces a combined extorsion and elevation with minimum abduction secondary to the insertion being posterior to the center of rotation.
The spiral of Tillaux is a theoretic line connecting the insertions of the four rectus tendons. The medial rectus is closest to the limbus at 5.5 mm posterior to it. The IR insertion is at 6.5 mm, the LR is at 6.9 mm, and the SR is at 7.7 mm.
Hering’s law of motor correspondence states that equal and simultaneous innervation is given to yoke muscles (or muscle groups concerned with a desired direction of gaze). The law is applicable to voluntary and some involuntary muscle movement.
In practical application, during left gaze the right MR and left LR muscles receive equal innervation. If the head is tilted to the right, the muscle groups concerned with cycloduction (intorsion) of the right eye and excycloduction (extorsion) of the left eye will receive equal and simultaneous innervation.
Diagnosis of paralytic strabismus is aided by knowledge of Hering’s law in determining primary and secondary deviations. Because the amount of innervation to both eyes is determined by the fixating eye, the angle of deviation
will vary depending on the eye used for fixation. Primary deviation occurs when the nonaffected eye is fixing; secondary deviation occurs if fixation is with the paretic eye. The examiner may detect a paretic muscle or muscle group in noncomitant strabismus (measured deviation unequal in different directions of gaze) by measuring the deviation of the eyes in diagnostic positions of gaze with each eye fixating in turn. For example, in paralysis of the right LR, normal innervation moves the normal left eye to place it in primary gaze. The paretic right eye does not follow outward because the normal amount of innervation received by the paretic right eye is not sufficient to overcome the paresis of the right LR, resulting in what is called primary deviation. However, when the paretic eye fixates in primary gaze an excessive amount of innervation is released in an attempt to keep the right eye in the primary gaze. By Hering’s law, the same increased level of innervation will be transmitted to the normal MR of the contralateral eye, resulting in an excessive adduction of that eye. This is secondary deviation and is greater in magnitude than the primary deviation. It points to the right LR as the paretic muscle.
Sherrington’s law of reciprocal innervation states that increased innervation of an extraocular muscle is associated normally by diminished innervation activity of its antagonist muscle. Therefore, on right gaze, there is increased contraction of the left MR and the right LR, accompanied by decreased tone of the antagonistic left LR and right MR. During convergence, there is increased activity of both MR muscles with associated decreased activity of both LR muscles. When the head is tilted to the right shoulder there is contraction and relaxation of antagonistic muscle groups on levocycloversion.
Ductions refer to the movement of just one eye. Abduction is the horizontal movement away from the midline vertical axis and is a function of LR contraction and MR relaxation. Adduction is the horizontal movement toward the midline vertical axis and is accomplished by the contraction of the MR muscle and relaxation of the lateral muscle. Infraduction is a vertical movement or depression inferior to the horizontal axis of the eye and results from combined contraction of the IR and SO muscles. Supraduction is a vertical movement or elevation superior to the horizontal axis of the eye, and results from the combined contraction of the SR and IO muscles and the combined relaxation of the IR and SO muscles. Incycloduction or intorsion is a rotary movement of the eye about the anteroposterior (AP) axis such that the superior pole of the cornea is displaced medially and results from combined contraction of the SO and SR muscles with relaxation of the IO and IR muscles. Excycloduction or extorsion is a rotary movement of the eye around the AP axis displacing the superior pole of the cornea laterally and results from the combined contraction of the IO and IR muscles with concomitant relaxation of the SO and SR muscles.
Binocular movements are divided into two categories: versions and vergences.
A version refers to the simultaneous conjugate movement of both eyes (in the same direction). Versions, like ductions, normally adhere to Hering’s and Sherrington’s laws, and include right and left lateral horizontal and vertical gaze.
Dextroversion and levoversion. Dextroversion, the movement of both eyes to the right, is the result of contraction of the right LR and left MR muscles. Levoversion, the movement of both eyes to the left, is accomplished by contraction of the left LR and right MR with simultaneous relaxation of the left MR and the right LR.
Vertical versions are elevation or depression. Elevation, or upgaze, is the result of bilateral contraction of the SR and IO muscles with simultaneous relaxation of the inferior recti and SO muscles in the primary position. Depression, or downgaze, in the primary position is the result of increased innervation to the IR and SO.
Cycloversion is the simultaneous and equal tilt of the superior corneal poles to the right or left. Dextrocycloversion is the result of contraction of the
extorters of the right eye (IR and IO) and the intortors of the left eye (SR and SO) with concomitant relaxation of their antagonist muscles. Levocycloversion is the mirror image of this action, with increased innervation to the extorters of the left eye and the intortors of the right eye and decreased innervation to their antagonistic muscle groups.
A vergence is the equal simultaneous, disconjugate movement of the eyes (in opposite directions). Convergence is inward movement of both eyes; divergence is a simultaneous outward movement. Convergence is the result of contraction of both medial recti and relaxation of the lateral recti; divergence results from contraction of the lateral recti with concomitant relaxation of the medial recti. Vertical vergences result in contraction of the elevators of one eye and the depressors of the contralateral eye with subsequent opposing vertical movements. Cyclovergence is simultaneous equal tilting of the corneal superior poles inward or outward.
The primary position of gaze is the position assumed by the eyes when fixating a far distant object directly ahead. Secondary positions are any eye positions other than primary and include near-fixation, the cardinal positions, and midline vertical positions.
The near-fixation position is usually taken at 0.33 m from the eyes. This reflex involves convergence and accommodative action.
The cardinal positions are six positions of gaze that compare the horizontal and vertical eye alignment resulting from the isolated action of each of the six extraocular muscles (Fig. 12.2).
II. Single Binocular Vision
is a conditioned reflex, the prerequisites for which are straight eyes starting in the neonatal period and similar images presented to each retina. Patients with congenital strabismus lack central single binocular vision, but early elimination of the strabismus may result in peripheral single binocular vision. The age at which congenitally strabismic patients may develop single binocular vision after
surgical straightening is unknown, but the current estimate is by 2 years of age. Simultaneous perception fusion, and stereopsis are three different perceptual phenomena comprising single binocular vision. They may function simultaneously or in decreasing degrees, with stereopsis being the most highly developed and simultaneous perception the least developed in normal eyes. For each retinal point in one eye there is a corresponding retinal point in the opposite eye, within which the same image must project if the two are to be fused into a single image. The further this retinal point is from the fovea, the larger the corresponding area in the opposing eye. If the retinal sites are anatomically identical, normal retinal correspondence (NRC) is present (see Section VI.C).
surgical straightening is unknown, but the current estimate is by 2 years of age. Simultaneous perception fusion, and stereopsis are three different perceptual phenomena comprising single binocular vision. They may function simultaneously or in decreasing degrees, with stereopsis being the most highly developed and simultaneous perception the least developed in normal eyes. For each retinal point in one eye there is a corresponding retinal point in the opposite eye, within which the same image must project if the two are to be fused into a single image. The further this retinal point is from the fovea, the larger the corresponding area in the opposing eye. If the retinal sites are anatomically identical, normal retinal correspondence (NRC) is present (see Section VI.C).
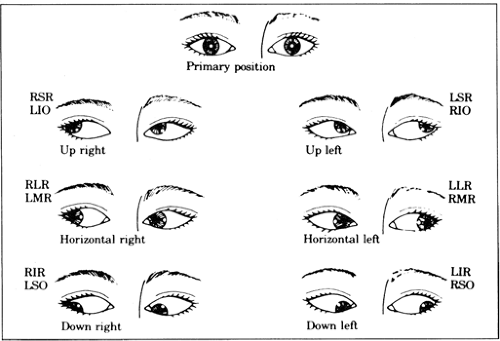 Figure 12.2. Normal cardinal positions of gaze and extraocular muscles involved as primary movers in a given field of gaze. R, right; L, left; SR, superior rectus; IO, inferior oblique; LR, lateral rectus; MR, medial rectus; IR, inferior rectus; SO, superior oblique. |
In simultaneous perception, all objects projecting their images outside of corresponding retinal areas are not fused, but they may be perceived simultaneously. This may result in double vision or diplopia unless the patient is inattentive to these images.
Fusion is the result of all objects projected onto corresponding retinal points, with their two images fused at the level of the central nervous system (CNS) into one perception.
Stereopsis is the perception of the third dimension (i.e., the relative nearness and distance of object points as obtained from fused but slightly disparate retinal images). The Titmus test for stereopsis is described under tests for retinal correspondence (see Section VI.C.3.a).
III. Strabismus Classification
The general order of examination for strabismus is as follows:
History
Deviation: Age of onset, description of deviation, frequency and duration, symptoms, and previous treatment. A review of unposed photographs of the patient at various ages is useful.
Personal: Pre- and postnatal factors, course of pregnancy, delivery, growth and development, medications, and surgery.
Family: Strabismus in blood relatives.
General observation
Abnormal head posture or nodding.
Spontaneous closure of one eye (squint).
Visual acuity
Without glasses and with glasses, if worn.
Near and distance vision.
Amblyopia testing, isolated versus linear letters, crowding.
Motor
Ductions and versions of extraocular muscles.
Near point of convergence.
Near point of accommodation, where indicated.
Measurement of deviation:
Cover tests (phoria or tropia) distance and near, without and with glasses, if worn; with +3.00 add at near; with eyes in all nine positions of gaze and head tilt when indicated.
Accommodative convergence-accommodation (AC/A) ratio.
Sensory tests (depending on age and cooperation)
Worth four-dot test near and distance, without and with glasses, if worn.
Stereopsis.
Amblyoscope: After image, Bagolini lenses where indicated.
Fusional vergence reserves.
Double Maddox rods where indicated.
Fixation
Monocular, alternating, binocular.
Nystagmus type.
Visuscope: Foveal, or eccentric fixation.
External examination.
Anterior segment examination.
Fundus examination
Assess fundus torsion.
Cycloplegic refraction.
Pseudostrabismus
Pseudoesotropia or apparent turning in of the eyes may result from a prominent epicanthal skin fold that obscures part of the normally visible nasal aspects of the globe, thereby giving a false impression that esotropia is present. As the infantile flat nasal bridge develops, this excessive epicanthal skin is raised and the condition self-corrects.
Pseudoexotropia is seen in hypertelorism, in which there is an abnormally wide separation of the eyes as a result of disproportionate growth of the facial bones, or as a primary deformity. Despite the physical appearance, the eyes are aligned normally.
Pseudohypertropia may result from orbital or palpebral asymmetry simulating a vertical ocular deviation.
Angle kappa is the angle between the line of sight that connects the point of fixation with the nodal points at the fovea and the pupillary axis with the line through the center of the pupil perpendicular to the cornea. The angle is positive when the corneal light reflex is displaced nasally and negative when it is displaced temporally. A positive angle kappa up to 5 degrees is considered physiologic in emmetropic eyes. The angle kappa is measured on a perimeter with the patient fixating on the central mark. A light is moved along the perimeter until its reflex is centered on the cornea. The difference in the position of the light and the center mark is indicated in degrees of arc on the perimeter and constitutes the angle kappa, which can also be measured with an amblyoscope using a special slide. This angle is significant in that a positive angle kappa may simulate an exodeviation. This is particularly common in retinopathy of prematurity where the macula is dragged temporally. A negative angle kappa may simulate esodeviation unless the cover test is performed. Ocular misalignment may be missed in an apparently normally alignment if a positive angle kappa is associated with a small angle esotropia or a negative angle kappa with a small exotropia.
Orthophoria indicates that the eyes are aligned with no latent deviation even when fusion is artificially disrupted by the examiner.
Heterophoria is a latent deviation controlled by torsion. The eyes have a tendency to drift out of alignment when fusing is disrupted. It may be detected by the tests described in Section IV.
Heterotropia is the manifest misalignment of the eyes. The cover-uncover test is used to document the presence of a tropia (Fig. 12.3).
Horizontal deviations consists of esotropia, in which the eyes are convergent (inward deviation of the eyes), and exotropia, in which the eyes are are divergent (outward deviations of the eyes).
Vertical deviations include hypertropias, in which the fellow eye is higher than the fixing eye, and hypotropia, in which the fellow eye is lower than the fixing eye.
Torsional deviations include incyclotropia, in which the superior poles of the corneas are tilted medially, and excyclotropia, in which the superior poles of the corneas are tilted temporally.
IV. Diagnostic Tests
in strabismus are many. The most commonly used tests fall into four basic categories: (a) cover tests, which depend on the fixation reflex; (b) corneal reflex tests, which are based on the ability of the corneal surface to reflect the examining light; (c) dissimilar image tests, which are based on patient response to double vision produced by converting an isolated object of regard into separate images on each retina; and (d) dissimilar target tests, which are based on patient response to dissimilar images when different targets are presented to each eye. Many of these tests involve eliciting diplopia (double vision) as a means of evaluation.
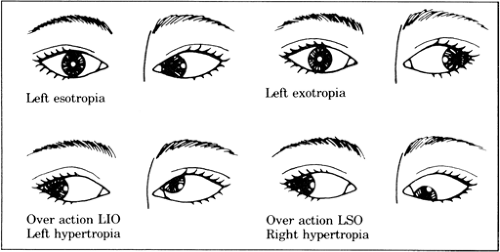 Figure 12.3. Common heterotropic muscle imbalances. LIO, left inferior oblique; LSO, left superior oblique. |
Cover tests. The cover test and cover-uncover test are qualitative tests used to determine whether a heterophoria or heterotropia is present. These tests are performed using fixation targets at both distance and near.
Cover tests for detection of heterotropias. If heterotropia is present, tests for fusion are negative because one eye is not aligned with the fixation target. Covering the fixating eye will require the deviated eye to move to take up fixation, and this movement in the uncovered eye is looked for by the observer. If the nonfixating deviated eye is covered, however, there will be no movement of the fixating eye. Consequently, each eye must be covered in turn and the fellow eye watched for a fixation shift to determine whether tropia is present or not. If the eye moves outward to fixate, esotropia is present; if the eye moves inward to fixate, exotropia is present. If the uncovered eye moves downward, a hypertropia exists. If the uncovered eye moves upward, a hypotropia exists. Tropias of any type may be quantitated by placing prisms of increasing strength before the deviating eye until no fixation movement occurs on uncover: base-out for esodeviation, base-down for hyperdeviation, base-up for hypodeviation, and base-in for exodeviation (Fig. 12.4).
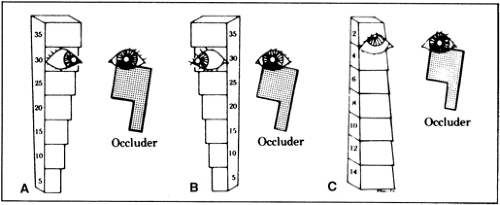
Figure 12.4. Use of prism bar. A: Horizontal prism bar run base-out to measure esodeviations. B: Horizontal prism bar run base-in to measure exodeviations. C: Vertical prism bar base-down over hypertropic right eye (or base-up over hypotropic left eye alternative).
Cover-uncover tests for heterophoria detection. Phoria deviations are kept latent by fusion mechanisms as long as both eyes are in simultaneous use. When fusion is disrupted by occluding one eye, the latent deviation will become evident. Each eye is covered separately in turn for 2 to 3 seconds and the occluder then quickly removed. The examiner must note whether the eye under cover makes a movement inward or outward to pick up fixation again. If there is no movement of either eye when it is covered and then uncovered, there is either no latent phoria present or a microtropia syndrome is present and must be tested for (see Section X.A). If, when uncovered, an eye moves outward to fixate, esophoria is present. If the eye moves inward to fixate, exophoria is present. A movement down to fixation reveals hyperphoria, and a movement upward to fixate reveals hypophoria. A disadvantage of this test is that small-angle phorias may be missed, but these may be picked up later with the Maddox or base-out prism tests (see Sections III.B and C).
The simultaneous prism-cover test measures the manifest deviation and is most useful in patients with small-angle heterotropia. The examiner covers the fixating eye and simultaneously slips a prism of known power and appropriate base direction in front of the uncovered eye. This may need to be repeated until the prism power selected equals the heterotropic angle and no movement occurs as the eye behind the prism takes up fixation.
The prism alternate cover test quantifies the total deviation made up of the manifest and latent deviation together. The prism is placed over one eye, and the cover is alternately placed in front of each eye. The uncovered eye is observed for movement, and the prism power is increased until the eye movement is neutralized. The power of the neutralized prism corresponds to the amount of deviation present.
Quantitative measurement of strabismic deviation by corneal reflex tests
Hirschberg test. A fixation light is held 33 cm from the patient, and the deviation of the corneal light reflex from the center of the pupil in the nonfixating (turned) eye is estimated. Each millimeter of decentration corresponds to 7 degrees of ocular deviation. Therefore, a 3-mm inward deviation of the light reflex corresponds roughly to a 21-degree exotropia, whereas a 4-mm outward deviation of the light reflex corresponds roughly to 28 degrees of esotropia. One degree equals roughly two prism diopters of deviation.
Modified Krimsky test. Asymmetric positions of the corneal reflex in the pupils of each eye are indicative of strabismus, which may be measured by placing successively increasing prism power before the fixating eye until the reflection is similarly positioned in both eyes. Base-out prism is used for esotropia, and base-in prism is used for exotropia (Fig. 12.4). This is a direct reading of the squint angle.
The major amblyoscope is a haploscopic device that consists of a medial septum between the two eyes with angled mirrors that reflect separate targets for each eye. These targets are set at the focal distance of the lenses in the eyepiece; thus, viewing the targets simulates optical infinity or distance fixation. addition The of -3.00 spheres into the eyepiece stimulates accommodation and near convergence so that a reading of the deviation at near can be made. Adjusting the tubes so that the corneal reflexes of illumination are centered in each pupil gives the examiner an approximation of the angle of deviation. By alternately occluding the light sources and having the patient fixate on the lighted target, the alternate cover test can be performed and the angle of deviation can be read directly.
Dissimilar image tests
Maddox rod testing for heterophoria or tropia is diplopia testing with dissimilar images of the same object. The Maddox rod is a red- or white-ribbed lens. A point source of light shined through this lens is seen as a red or white streak 90 degrees away from the axis of the multiple cylinders of the rod. Horizontal alignment may be checked by orienting the rod so that the streak is vertical, and
vertical alignment checked by orienting the rod so that the streak is horizontal. The patient views the fixing light with both eyes open. If the streak appears to run through the center of the light both vertically and horizontally as the lens is turned, orthophoria is present in both directions. If the streak is displaced away from the light, misalignment is present. A phoria cannot be distinguished from a tropia by this test.
Horizontal deviations. If the patient sees the vertical rod streak on the same side of the light as the eye that has the rod in front of it, uncrossed images are present and indicative of esodeviation. If the patient sees the streak on the other side of the fixation light from the eye behind the Maddox rod, crossed images are present and indicative of exophoria or exotropia. The degree of phoria or tropia may be measured directly by increasing the amount of prism power presented before one eye with base-out for esodeviation and base-in for exodeviation until the streak is aligned in the center of the light. The measurement may then be read directly from the prism power producing this effect. Maddox rod measurements are valid only with NRC.
Vertical deviation may be measured by presenting base-down prism to a hypertropic eye or base-up prism to a hypotropic eye until the horizontal streak is aligned with the fixation light.
Cyclodeviations may be checked by placing Maddox rods, one red and the other white, before each eye at the same axis setting for each eye. The axis settings of the rods are then adjusted until they appear parallel to the patient. The difference in degrees in cyclodeviation may then be measured directly from the trial frame in which the rods are set. Cyclodeviations may also be measured with an amblyoscope.
The red glass test is straightforward diplopia testing utilizing the image seen by the fovea of the fixating eye and the extrafoveal image of the deviated eye. It is performed by placing a plain red lens in front of one eye. This test is similar to the Maddox rod tests in horizontal and vertical deviations but is of no value in cyclodeviation measurement. Prisms with bases oriented toward the appropriate direction for the types of deviation (see Section III.C.1) are used to eliminate the horizontal or vertical diplopia of white light and red light when the patient is viewing the fixation bulb, thereby yielding a direct measure of the deviation in the presence of NRC. The Maddox rod and red glass tests can be used to measure deviations in the diagnostic positions of gaze.
Separate image tests. In the presence of NRC, the point at which two separate images, one presented to each eye, appear superimposed provides a direct reading of the patient’s alignment.
Lancaster red-green projection. The patient wears glasses with a red filter before one eye and a green filter before the other and views a white screen marked with a grid calibrated in squares of 7 degrees (14 pds) from a distance of 1 m. A linear red light and a linear green light are shined on the screen simultaneously, one light held by the patient and the other by the examiner (light held by the examiner determines the fixating eye), and adjusted until they are seen as superimposed by the patient. Any actual disparity between the location and angle of the red and green lights gives the examiner a direct reading in centimeters of any deviation—horizontal, vertical, and torsional.
The major amblyoscope is used to show the patient dissimilar objects that are simultaneously seen, one with each eye. The patient is asked to adjust the angle of the tubes so that one image is superimposed on the other. In the presence of NRC, horizontal, vertical, and torsional deviations may be read directly from the scales on the instrument, which indicate the deflection of the tubes away from 0 in these three planes.
V. Measurement of Fusional Reserves (Vergences)
Patients with heterophoria and microtropia may be asymptomatic by virtue of their relative fusional reserves. These reserves may be measured using accommodative targets at near and distance on a major amblyoscope. To measure divergence reserves, the examiner
increases base-in prism over one eye until the patient reports blurring or diplopia of the target. To measure convergence reserves, base-out prism is increased to a similar end point. Vertical fusional reserves, positive, are determined by placing prism base-down before the right eye and, negative, by placing prism base-down before the left eye. Normal divergence reserves are in the range of 6 D with rapid recovery at distance, 10 to 14 D at near. Normal convergence reserves are 20 to 30 D at distance with rapid recovery and slightly more at near. Vertical reserves average 2 to 4 D at near or distance.
increases base-in prism over one eye until the patient reports blurring or diplopia of the target. To measure convergence reserves, base-out prism is increased to a similar end point. Vertical fusional reserves, positive, are determined by placing prism base-down before the right eye and, negative, by placing prism base-down before the left eye. Normal divergence reserves are in the range of 6 D with rapid recovery at distance, 10 to 14 D at near. Normal convergence reserves are 20 to 30 D at distance with rapid recovery and slightly more at near. Vertical reserves average 2 to 4 D at near or distance.
VI. Sensory Evaluation
Visual acuity. Early determination of visual acuity is critical in evaluation of any patient with strabismus. An estimation of visual acuity may be obtained in infants by observing behavior as each eye is alternately covered. If vision is equal or nearly equal in either eye, an infant or very young child will not object to having either eye covered. If visual acuity is reduced in one eye, however, the child will cry or push the occluder away when the normal eye is covered. If this occurs, ocular disease, amblyopia (nonorganic visual loss), or high refractive error should be suspected.
The preferential looking technique permits reliable measurements of visual acuity to be made in infants from birth to age 1 year. At present this technique, as well as evoked potential estimates of acuity, is still available at specialized university medical centers. Before assuming that amblyopia is present (see Section VI.D), it is essential that the examiner establish that visual loss is not the result of organic disease. This is done by taking a past medical history on the child, including any circumstances during or after pregnancy that may have contributed to ophthalmic disease in the child. An examination of the ocular anterior segments under magnification is essential. A dilated fundus examination, with the indirect ophthalmoscope, to rule out retinal pathology is an essential part of every examination.
Visual acuity may be determined in the illiterate and in preschool children (age 36 to 60 months) using the E game. The parent instructs the child at home how to respond to the examiner’s test, by indicating with the hand, or with a test letter that he or she holds, the direction in which the three bars of a test letter E held by the examiner are pointing. The illiterate Es can also be projected. An alternate means is the use of Allen preschool vision test on cards or projected Allen figures, which are small animals and common images that the child age 18 to 36 months is asked to identify. Once the child understands the test, vision may be determined by finding the smallest letter E or Allen figure read with each eye at 20 ft or, alternately, if vision is very poor, designating the optotype read at a specified distance closer than 20 ft.
Suppression testing. Suppression scotomas (areas of decreased retinal sensitivity) are present both in eso- and exotropic patients. The esotropic patient has an area of suppressed vision extending nasally to the hemiretinal line, whereas the exotropic patient has an area of suppressed vision extending over a large area temporal to the hemiretinal line. These scotomas protect the patient from double vision (diplopia) when both eyes are open.
The Worth four-dot test will detect fusion, suppression, and anomalous retinal correspondence (see Section VI.C). The patient wears a red filter before one eye and a green filter before the other, mounted in the glasses frame, and views four lights at near and distance—two green, one red, and one white. Normally the white light is seen as red through the red filter and the green light through the green filter; the green lights are seen through only the green filter, and the red light through only the red filter. A patient who is fusing reports four lights, with the white light usually seen as a mixture of red and green. A patient suppressing the eye with the red filter will see three green lights, and the patient suppressing an eye with the green filter will see two red lights. The examiner may test the macular area by using the Worth dots held at 0.6 m from the patient. Fusion at this distance reveals macular or central fusion. Extramacular fusion (peripheral
fusion) is detected by projecting Worth lights at a distance 0.33 m from the patient. Patients with an esotropia of 10 pd or greater will not fuse the distant Worth four dots. NRC will be identified in strabismic patients if they report that they see five lights (two red and three green), if the position of the lights corresponds to the angle of deviation. The dots seen by the fixating eye will be clear, whereas those seen by the deviating eye will be blurred. Anomalous retinal correspondence is present if the patients report that they see four dots while displaying a manifest deviation.
The red glass test for suppression and detection of retinal correspondence. A heterotropic patient with normal vision in each eye but no diplopia may be suppressing or ignoring the image received by the retina of the deviated eye. With the patient fixating on a bright white light, a red glass placed before the deviated eye will make the second image visible to the patient if it has been ignored. If there is deep suppression present, only the white light will be seen despite the presence of the red lens over the deviated eye. Some examiners prefer holding the red glass over the fixating eye to make the patient aware of diplopia more easily, thereby evaluating the depth of suppression. If NRC is present, the patient sees the red light on the same side as the eye behind the red glass; uncrossed diplopia is present, indicating esodeviation. In crossed diplopia the red image is seen on the opposite side of the eye behind the red glass and indicates an exodeviation. If the red image falls on a suppression scotoma in the deviating eye of an exotropic patient, it is not seen. If the red filter is then placed before the fixating eye, diplopia may be elicited despite the presence of deep suppression. Suppression may be differentiated from anomalous retinal correspondence by holding a prism base-down before the red glass, thereby displacing the retinal image upward and beyond the suppression scotoma. With NRC, the image will appear superiorly and to the right or left of the light. If anomalous retinal correspondence is present, the image will appear horizontally aligned but separated vertically from the fixation light.
The 4-pd base-out test is used to determine whether central fusion (bifixation) or absence of central fusion (monofixation) is present in a patient whose eyes appear straight. With the patient reading letters on the distance vision chart, a 4-pd base-out prism is slipped alternately before one eye and then the other. The prism-covered eye is watched for movement. If the prism is placed before the fixating eye and both eyes move toward the apex of the prism and stay moved, and if the prism is placed before the nonfixating eye, neither eye moves, a microtropia is present. The absence of movement by one eye is proof of a relative macular scotoma on that side. Bifixation may be recognized by each eye moving inward to refixate in response to displacement of the image produced by the prism. Occasionally, a bifixating patient will not make the necessary convergence movement to pick up the moved image, thereby making the test variable in its accuracy.
Blind spot syndrome
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


